Page 2 of 13
CM12.1-2 | CM12.1-2 | Geriatric Services and Health Problems — SDL Guide (Part 2)
Physical Health Problems of the Aged
The elderly carry a disproportionate and distinctive burden of physical morbidity. Unlike younger adults where single-disease episodes are the norm, older adults typically present with multi-morbidity — two or more chronic conditions managed simultaneously — which complicates diagnosis, treatment, and drug safety.
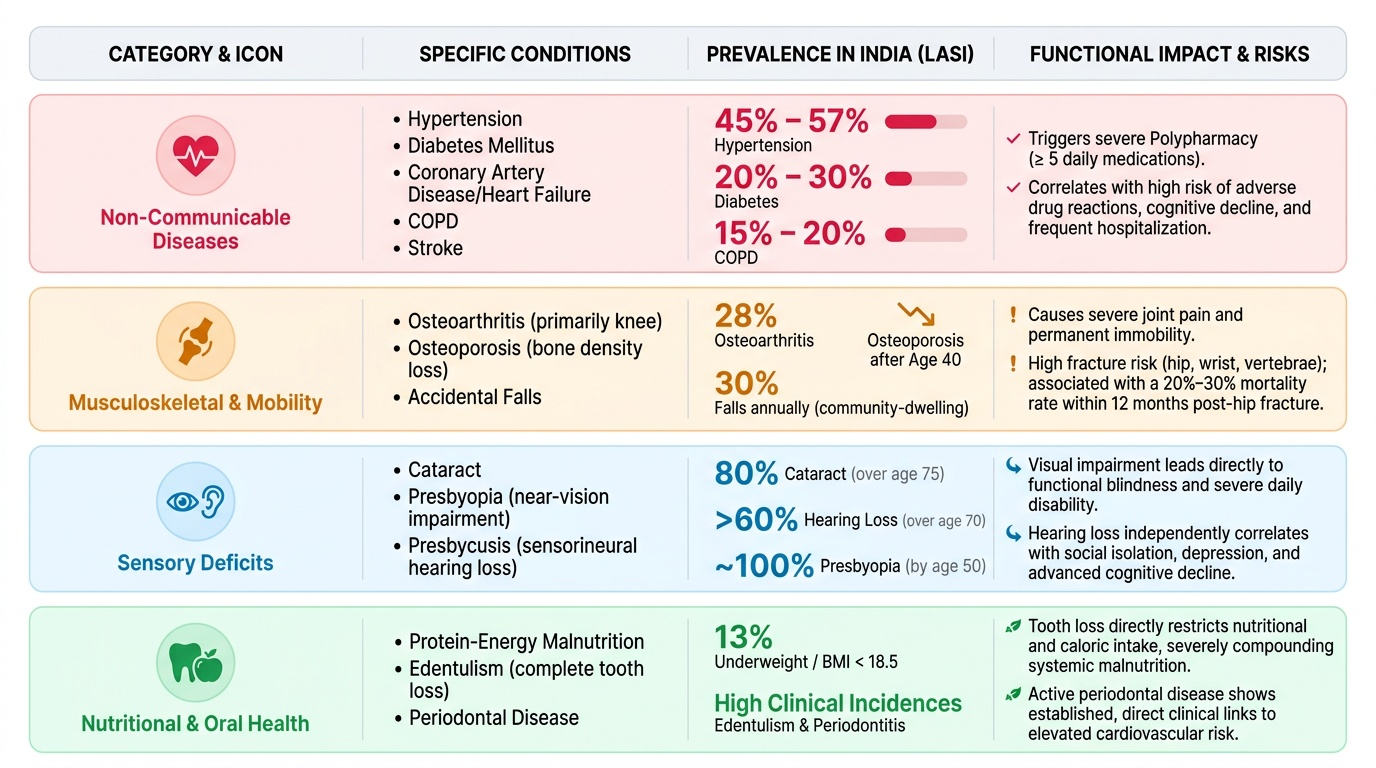
The non-communicable diseases (NCDs) dominate: hypertension affects 45–57% of elderly Indians (LASI data), diabetes approximately 20–30%, coronary artery disease and heart failure are leading causes of mortality, chronic obstructive pulmonary disease (COPD) affects 15–20%, and stroke survivors (with residual disability) constitute a major subgroup needing rehabilitation. The co-occurrence of multiple NCDs exponentially increases the medication burden — polypharmacy (typically defined as ≥5 regular medications) affects more than half of elderly patients and is independently associated with adverse drug reactions, falls, cognitive impairment, and hospitalisation.
Musculoskeletal problems are the leading cause of disability: osteoarthritis affects up to 28% of elderly Indians (particularly knees), producing pain and immobility. Osteoporosis is the silent disease — bone mineral density declines progressively after the 4th decade; fractures (hip, vertebral, wrist) are the clinical consequence, and hip fracture in the elderly carries a 12-month mortality of 20–30% and a high risk of permanent functional loss. Falls are the single most common cause of injury, hospitalisation, and injury-related death in the elderly; 30% of community-dwelling elderly fall at least once per year.
Sensory deficits accumulate with age. Presbyopia (age-related near-vision loss, affects virtually all by age 50) and cataract (leading cause of blindness in India, affecting 80% of those over 75 to some degree) produce functional disability out of proportion to their perceived severity. Presbycusis (sensorineural hearing loss with age) affects over 60% of those >70 years and is independently associated with social isolation, depression, and cognitive decline. Oral health deteriorates — edentulism (tooth loss) affects nutritional intake; periodontal disease is linked to cardiovascular risk.
Malnutrition is paradoxically common among Indian elderly: the LASI survey found that 13% of elderly are underweight (BMI <18.5), with protein-energy malnutrition particularly prevalent in rural women. Even among overweight/obese elderly, micronutrient deficiencies (vitamin D, vitamin B12, folate, iron) are common and contribute to musculoskeletal deterioration, cognitive decline, and neuropathy.
Provided image
| Category | Key Conditions | Approximate Prevalence in Elderly (India) | Major Functional Impact |
|---|---|---|---|
| NCDs | HTN, diabetes, COPD, IHD | HTN 45–57%, diabetes 20–30% | Medication burden, hospitalisation |
| Musculoskeletal | Osteoarthritis, osteoporosis, falls | Arthritis ~28%, falls ~30%/year | Immobility, fractures, pain |
| Sensory | Cataract, presbycusis | Cataract 80% by 75 yrs, hearing loss 60% by 70 yrs | Isolation, communication, fall risk |
| Nutrition | Underweight, micronutrient deficiency | Underweight 13% (LASI) | Sarcopenia, cognitive decline |
SELF-CHECK
A 68-year-old woman is found to have hypertension, diabetes, and osteoarthritis, and is on 7 regular medications. Which term BEST describes the risk she faces from her medication regimen?
A. Multi-morbidity
B. Polypharmacy-related adverse effects
C. Frailty
D. Homeostenosis
Reveal Answer
Answer: B. Polypharmacy-related adverse effects
While multi-morbidity (≥2 chronic conditions) and frailty are both relevant concepts here, the specific risk from having 7 regular medications is polypharmacy-related adverse effects. Polypharmacy is defined as ≥5 regular medications and is associated with drug interactions, adverse drug reactions, falls, and hospitalisation in the elderly. Multi-morbidity describes the co-occurrence of conditions (this patient has 3); homeostenosis refers to reduced physiological reserve. Frailty is a broader vulnerability state not captured by medication count alone.
Mental and Psychosocial Health Problems of the Aged
Mental health problems in older adults are as burdensome as physical diseases, yet are systematically under-recognised and under-treated — partly because their symptoms are attributed to 'normal ageing' and partly because elderly patients under-report psychological distress. The global burden of disease data identify neuropsychiatric conditions as the leading cause of disability-adjusted life-years in adults over 60.
Depression is the most prevalent and disabling mental health condition in the elderly. Prevalence estimates in community-dwelling Indian elderly range from 25 to 41% (depending on screening tool and setting), far exceeding the younger adult population. Late-life depression presents differently from younger-adult depression: somatic complaints (pain, fatigue, constipation) often dominate; cognitive symptoms (memory complaints, concentration) may be indistinguishable from early dementia (pseudodementia); and depressed elderly often do not acknowledge sadness but present with anhedonia (loss of pleasure/interest). Risk factors include bereavement (especially within 6 months of spousal death), social isolation, chronic pain, multiple physical illnesses, functional dependency, and financial insecurity. Depression in the elderly also significantly increases the risk of suicide — elderly men in India have among the highest suicide rates of any demographic group.
Dementia is a syndrome characterised by acquired, progressive deterioration in multiple cognitive domains (memory, language, executive function, visuospatial function) severe enough to interfere with daily life. The most common cause globally and in India is Alzheimer's disease (~60–70%), followed by vascular dementia (~20%). India is estimated to have over 8.8 million people living with dementia (Dementia India Report), a number that will treble by 2050 as the population ages. Dementia is a particularly heavy burden on families in India's predominant informal caregiving model — caregivers experience high rates of burnout, depression, and economic hardship.
Delirium — an acute, fluctuating disturbance in attention and cognition — is a medical emergency in the elderly. It is precipitated by common triggers (infection, medications, dehydration, pain, anaesthesia) that would be trivial in younger patients. Delirium is associated with prolonged hospitalisation, new institutionalisation, and acceleration of underlying dementia. It is frequently missed because staff attribute altered behaviour to 'confusion in old age.'
Psychosocial health problems include social isolation and loneliness (which increase all-cause mortality independently of physical disease — the evidence is now as strong as for smoking), elder abuse and neglect (physical, psychological, financial, sexual; Indian prevalence estimates range 20–50%), and loss of social roles and identity on retirement. The concept of 'successful ageing' — maintaining physical, mental, and social engagement into later life — has emerged as a positive-health framework that contrasts with the purely deficit-based disease model.
SELF-CHECK
An 80-year-old man admitted for a hip fracture repair becomes agitated and confused on post-operative day 2, with fluctuating levels of alertness. He was oriented on admission. Which condition does this MOST likely represent?
A. New-onset Alzheimer's disease
B. Delirium
C. Vascular dementia
D. Geriatric depression
Reveal Answer
Answer: B. Delirium
The key features here are ACUTE onset, FLUCTUATING course, and a clear precipitant (surgery, anaesthesia, pain, possible infection or dehydration). This is delirium — a medical emergency in the elderly. Alzheimer's disease has an insidious onset over months to years, not hours. Vascular dementia has a stepwise or slowly progressive course. Geriatric depression does not cause this acute confusional picture. Post-operative delirium is extremely common in elderly surgical patients and must be actively screened for and treated.
Geriatric Syndromes and Functional Decline
A defining characteristic of geriatric medicine is the concept of the geriatric syndrome — a clinical presentation unique to older adults that does not fit neatly into a single organ-system disease category and typically results from the interaction of multiple contributing factors across multiple systems. Understanding geriatric syndromes is essential because they are the primary reasons elderly patients present to health services, and yet they are frequently attributed to 'old age' and left unaddressed.
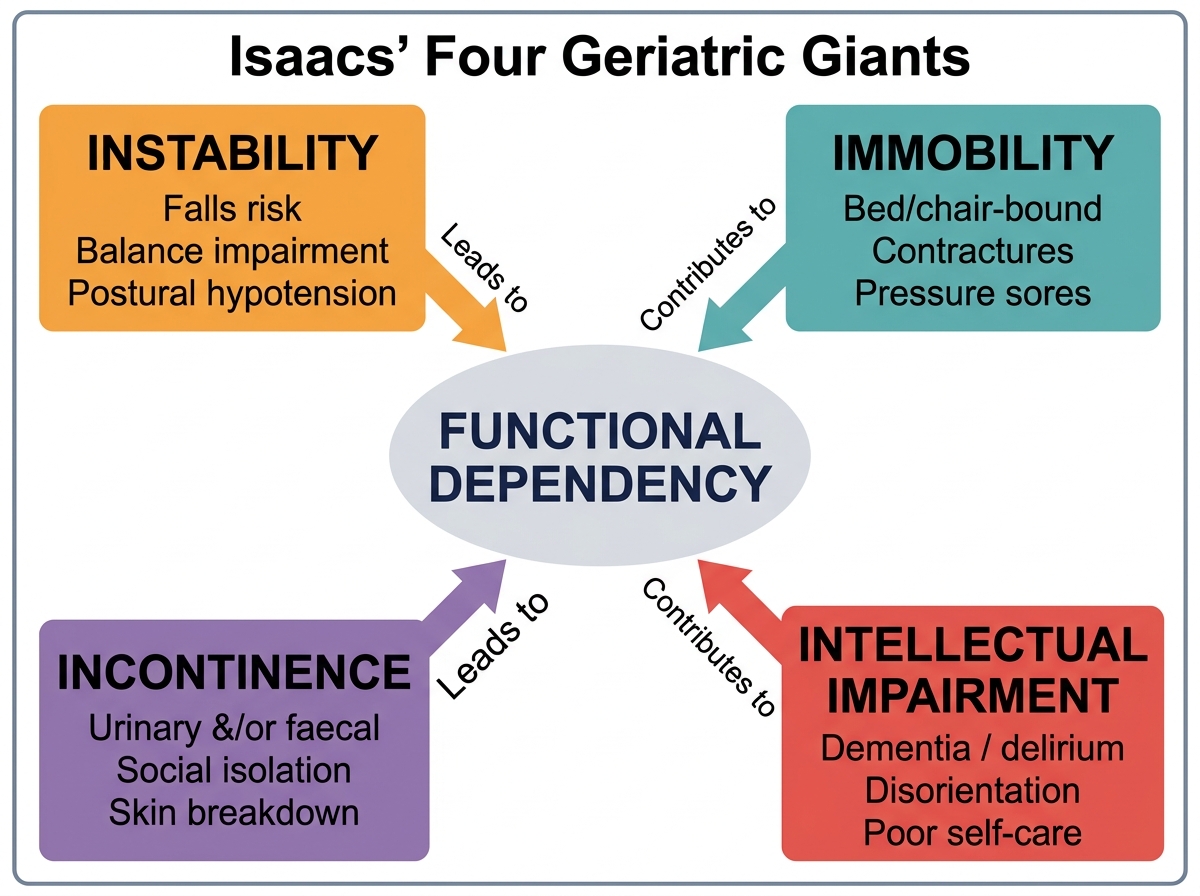
The most clinically important framework is Isaacs' four geriatric giants, described by Bernard Isaacs in 1965 and still the most compact and memorable classification of geriatric syndromes:
- Instability and falls — the commonest cause of injury in the elderly; results from the interaction of age-related balance deterioration, muscle weakness, polypharmacy (particularly antihypertensives, sedatives, antipsychotics), environmental hazards, and visual impairment. A single fall doubles the risk of a subsequent fall and triples hospitalisation risk.
- Immobility — reduced mobility that exceeds what would be expected from a specific disease; driven by pain (arthritis, fractures), fear of falling, neurological disease (Parkinson's, stroke), deconditioning, and inadequate rehabilitation. Immobility is a vicious cycle — inactivity worsens sarcopenia, which worsens falls, which worsens immobility.
- Incontinence — urinary (and to a lesser extent faecal) incontinence affects 30–50% of elderly women and 15–25% of men; it is a major source of embarrassment, reduces social participation, causes skin breakdown, and is a leading reason for institutionalisation — yet it is treatable in the majority of cases.
- Intellectual impairment — covering dementia, delirium, and depression-related cognitive changes; represents the cognitive pole of geriatric vulnerability.
These four syndromes frequently co-occur and are mutually reinforcing — a framework captured by the term frailty. Frailty is a state of increased vulnerability to stressors resulting from the cumulative decline across multiple physiological systems, reducing the body's capacity to maintain homeostasis after a challenge. The Fried frailty phenotype operationalises frailty as the presence of ≥3 of: unintentional weight loss, exhaustion, low physical activity, slow gait speed, and weak grip strength. Frailty predicts falls, disability, hospitalisation, and mortality better than any single disease or age cutoff.
Functional status — the ability to perform daily activities independently — is assessed via the Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) frameworks. The Katz ADL index covers 6 basic self-care activities (bathing, dressing, toileting, transferring, continence, feeding). The Lawton-Brody IADL scale covers 8 higher-order activities (shopping, cooking, managing finances, using the telephone, transportation, housekeeping, laundry, medication management). These scales are the standard functional endpoints in geriatric assessment worldwide and directly capture the impact of geriatric syndromes on independence.
Isaacs' Four Geriatric Giants and Their Convergence on Functional Dependency