Page 5 of 13
CM12.3-5 | CM12.3-5 | Prevention, Early Needs Identification and Elderly Programme — SDL Guide
Learning Objectives
- Describe the three levels of prevention applicable to health problems of the aged
- State the objectives, structure, and components of the National Programme for Health Care of the Elderly (NPHCE)
- Describe tools for early identification of health needs in elderly individuals
- Apply a systematic approach to identifying elderly at risk in community and PHC settings
INSTRUCTIONS
Knowing that the elderly carry a high burden of disease and functional decline is necessary but insufficient — the public-health imperative is to act on that knowledge before disability becomes permanent. This module moves from epidemiology to action: how do we prevent health problems in the elderly, what has India committed to through NPHCE, and — most critically — how do we identify who needs help before they lose independence? CM12.5 (identifying health needs at the earliest) is a skill competency that demands practical knowledge of screening tools and a systematic field approach.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 26th ed. Ch. 12 — Health in Old Age; Ch. 7 — National Health Programmes (textbook)
- Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18. International Institute for Population Sciences, Mumbai (survey)
- National Programme for Health Care of the Elderly (NPHCE) — Ministry of Health and Family Welfare, Government of India (2010) (policy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
During a community health camp in a rural village, an ANM finds an 78-year-old widow living alone. She has been managing on her own for two years since her son migrated for work. She complains only of 'weakness.' A quick screen reveals: she cannot rise from a chair without using her arms (slow gait/low grip strength), she forgot the name of the current Prime Minister (memory complaint), and she admits she has stopped attending temple 'because the path is uneven and I am afraid of falling.' She has no documented diagnosis and no medications. She has never been screened for hypertension, diabetes, or depression. What should the ANM do — and what tools and programmes exist to support her? This module answers those questions.
WHY THIS MATTERS
The elderly are the fastest-growing segment of India's population, yet they remain the most systematically under-screened. The Longitudinal Ageing Study in India (LASI) found that over 75% of elderly Indians with hypertension were either undiagnosed or inadequately controlled. A substantial proportion of elderly depression goes unrecognised because it presents with somatic complaints rather than mood symptoms. Falls, which affect 30% of community-dwelling elderly annually, are almost entirely preventable with the right interventions — yet most elderly are never assessed for fall risk in primary care. The gap between the burden of preventable morbidity in the elderly and the coverage of preventive services is one of the largest in Indian public health. NPHCE — launched in 2010 — was the Government of India's recognition that this gap requires dedicated infrastructure, not just more beds in general wards.
RECALL
Three prior concepts are essential scaffolding for this module. First, the levels of prevention (Leavell and Clark): primary prevention acts before disease onset (health promotion, risk factor reduction), secondary prevention identifies disease early before symptoms emerge (screening), and tertiary prevention limits disability after disease has occurred (rehabilitation). All three levels apply to the elderly but with a distinctive emphasis on function, not just disease. Second, the functional assessment framework from the previous module: ADL (basic self-care) and IADL (complex daily activities) scales, and the concept of frailty as a state of heightened vulnerability. These are the outcome measures that prevention and needs-identification aim to protect. Third, the National Health Mission (NHM) as the structural vehicle through which India's primary and secondary health services are delivered — NPHCE operates within NHM's framework.
Burden of Preventable Morbidity in the Elderly
Before describing preventive strategies, it is essential to establish what proportion of the elderly health burden is actually preventable. The answer — a large proportion — provides the epidemiological justification for investing in geriatric prevention rather than treating all elderly morbidity as inevitable consequences of ageing.
Hypertension affects 45–57% of elderly Indians (LASI Wave 1), yet more than half of those with hypertension in rural areas are unaware of their diagnosis. Uncontrolled hypertension is the primary modifiable risk factor for stroke (the leading cause of long-term disability in the elderly) and for accelerated kidney disease. The attributable fraction of stroke in the elderly that is preventable through blood pressure control exceeds 50% — meaning that if hypertension in elderly Indians were detected and managed, stroke incidence could be halved.
Type 2 diabetes affects approximately 20–30% of elderly Indians, and its complications — diabetic retinopathy (leading to blindness), peripheral neuropathy (contributing to falls), nephropathy (progressing to dialysis-dependency), and cardiovascular disease — are substantially prevented by glycaemic control initiated before end-organ damage occurs. Tobacco use in older adults — still prevalent among elderly men in India — drives COPD, cardiovascular disease, and oral cancer, all of which have substantially higher preventable fractions than most communicable diseases.
Falls deserve special attention as a preventable syndrome with catastrophic consequences. Thirty per cent of community-dwelling elderly fall at least once per year; 10% sustain a serious injury (hip fracture, head injury, joint dislocation). Hip fracture in the elderly carries a 12-month mortality of 20–30%, and survivors often never regain pre-fracture independence. The modifiable risk factors for falls are well-established: polypharmacy (especially sedatives, antihypertensives, anticholinergics), muscle weakness (sarcopenia), impaired balance, poor vision, and environmental hazards. Structured fall-prevention programmes — exercise, medication review, vision correction, home modification — reduce falls by 20–35%.
Depression in the elderly is preventable through social integration programmes, bereavement support, and management of chronic pain — and is treatable once identified. Its prevention and early identification are among the most cost-effective public-health interventions in geriatrics.
Primary and Secondary Prevention of Elderly Health Problems
The application of Leavell and Clark's prevention model to the elderly requires adaptation: the elderly are often already at a secondary or tertiary stage for one or more conditions while simultaneously being at a primary stage for others. A comprehensive geriatric preventive approach must therefore address all three levels simultaneously for the same individual.
Primary prevention in the elderly focuses on modifiable risk factors and health promotion behaviours that remain efficacious even in old age. Key primary preventive actions include:
- Physical activity: Even in those ≥75 years, regular moderate-intensity exercise (30 minutes, 5 days/week) reduces all-cause mortality, falls risk, depression, cognitive decline, and cardiovascular events. The benefits of initiating exercise in elderly individuals who have been sedentary are well-documented — there is no age threshold beyond which exercise stops helping.
- Nutrition and micronutrient supplementation: Protein-adequate diets prevent sarcopenia; calcium and vitamin D supplementation reduces osteoporosis and fractures; vitamin B12 and folate supplementation addresses deficiencies that drive cognitive decline and neuropathy in Indian elderly (where vegetarian diets are common).
- Tobacco cessation: Quitting smoking at any age reduces cardiovascular and respiratory disease risk; even at 70, cessation reduces 5-year cardiovascular mortality.
- Vaccination: The elderly are primary targets for influenza vaccine (annual, reduces influenza-pneumonia mortality by 30–40% in elderly populations) and pneumococcal vaccine (PCV13 or PPSV23 — reduces invasive pneumococcal disease). Neither vaccine is currently included in India's national immunisation programme for adults, but both are recommended in NPHCE guidelines.
- Social engagement: Maintaining social networks, cognitive stimulation (reading, community participation), and purpose-driven activities (volunteering, religious participation) are independently protective against cognitive decline and depression.
Secondary prevention through screening is particularly important in the elderly, where asymptomatic disease is common and presentations are atypical. Key screening interventions:
- Blood pressure measurement (hypertension screening) — detects undiagnosed HTN; recommended at every primary care contact for all elderly
- Fasting blood glucose or HbA1c (diabetes screening) — recommended annually for all elderly
- Visual acuity and hearing assessment — detects treatable sensory deficits before they produce falls and isolation
- Depression screening (GDS-15) — recommended for all elderly at first contact and annually thereafter
- Cognitive screening (MMSE or MoCA) — recommended when there is memory complaint or functional decline
- Fall risk assessment — standardised tools (STRATIFY, Timed Up and Go test) identify high-risk individuals for targeted intervention
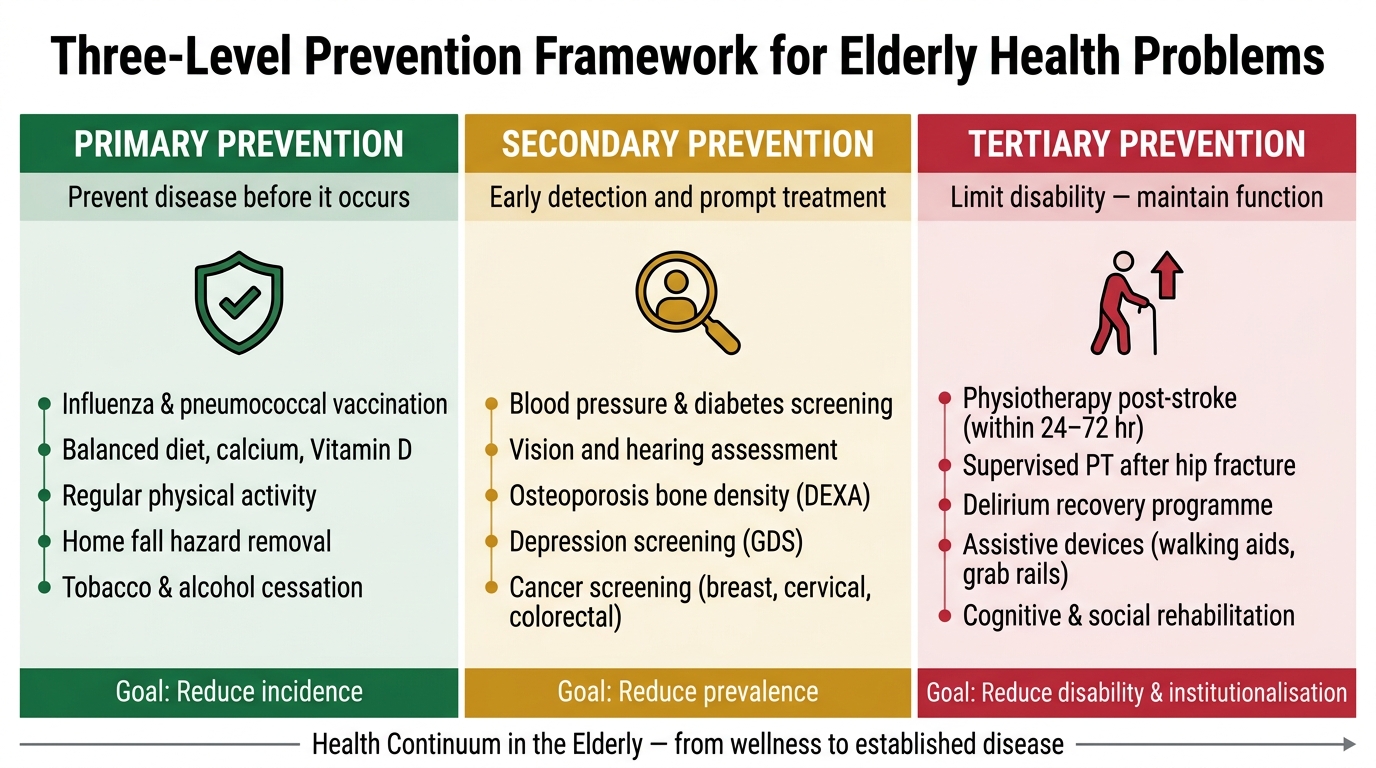
Three-Level Prevention Framework for Elderly Health Problems
Tertiary Prevention and Rehabilitation in the Aged
Tertiary prevention aims to limit disability and improve quality of life in those who already have established disease. In the elderly, this is not a niche concern — the majority of elderly patients who enter the health system already have at least one chronic condition. The goal of tertiary prevention in geriatrics is to maintain maximum functional independence and avoid unnecessary institutionalisation.
Rehabilitation is the cornerstone of tertiary prevention and encompasses physical, cognitive, and social rehabilitation. After a stroke, physiotherapy and occupational therapy can recover significant motor function if initiated early (within 24–72 hours) and maintained over weeks to months. After hip fracture, supervised physiotherapy is the difference between returning to independent ambulation and permanent wheelchair dependency. After delirium, a structured recovery programme (orientation, early mobilisation, sleep hygiene, dehydration correction) reduces delirium duration and the progression to permanent cognitive impairment. These are not luxuries — they are cost-effective interventions that reduce the need for long-term institutional care.
Assistive devices — walking aids, grab rails, non-slip mats, hearing aids, spectacles — are among the most cost-effective tertiary prevention tools in geriatrics and yet are dramatically underutilised in India, largely due to cost and stigma. NPHCE specifically includes provision of assistive devices for the elderly poor in its programme scope.
Caregiver training is a critical but often overlooked component. In India's predominantly family-based caregiving model, the quality of care an elderly person with Parkinson's disease, advanced COPD, or dementia receives depends almost entirely on the knowledge and capacity of their family caregiver. Training caregivers in safe transfer techniques, pressure ulcer prevention, medication management, and when to seek emergency care prevents complications and delays institutionalisation.
Palliative care — the proactive management of symptoms (pain, breathlessness, nausea) and psychological distress in those with advanced, irreversible disease — is the ultimate form of tertiary prevention in geriatrics: preventing suffering when cure is no longer possible. India's National Palliative Care Programme (operating under NHM) is the vehicle for this, though coverage remains very limited outside major cities.
SELF-CHECK
An 80-year-old man with COPD and heart failure comes to the PHC. He is on 8 medications and has fallen twice in the past 3 months. Which of the following represents a SECONDARY prevention action MOST appropriate at this visit?
A. Prescribing vitamin D supplementation to prevent osteoporosis
B. Conducting a fall risk assessment using the Timed Up and Go test
C. Referring for physiotherapy to improve his exercise tolerance
D. Providing a walking aid to reduce fall consequences
Reveal Answer
Answer: B. Conducting a fall risk assessment using the Timed Up and Go test
Secondary prevention identifies disease or risk before it causes harm — here, fall risk assessment screens for a high-risk state (he has already fallen, but a structured assessment identifies specific modifiable factors for intervention). Option A (vitamin D) is primary prevention of osteoporosis. Option C (physiotherapy for exercise tolerance) is tertiary prevention — limiting disability from existing COPD/HF. Option D (walking aid) is also tertiary prevention — reducing disability after a condition is established. The Timed Up and Go test is a validated fall risk screening tool that is appropriate in a PHC setting — it takes under 2 minutes and identifies high-risk individuals for targeted intervention.