Page 6 of 13
CM12.3-5 | CM12.3-5 | Prevention, Early Needs Identification and Elderly Programme — SDL Guide (Part 2)
National Programme for Health Care of the Elderly (NPHCE)
The National Programme for Health Care of the Elderly (NPHCE) is India's dedicated national programme for the health of elderly persons (≥60 years). It was launched in 2010-11 under the 11th Five-Year Plan by the Ministry of Health and Family Welfare, Government of India, operating within the National Health Mission framework. Its launch represented an explicit governmental acknowledgement that the elderly population had distinct health needs that could not be met by general health services alone.
The objectives of NPHCE are to: (i) provide accessible, affordable, and high-quality long-term, comprehensive, and dedicated care services to an ageing population; (ii) build a strong institutional framework to serve the growing numbers of elderly; (iii) build capacity for promotion of health and well-being of the elderly through family and community involvement; and (iv) provide referral services to the elderly for complex conditions at appropriate levels of health care.
NPHCE operates through a four-tier structure corresponding to India's existing health system architecture:
Tier 1 — Sub-centre and Village level: ASHAs and ANMs conduct house-to-house surveys to identify elderly with health needs, provide health education, distribute basic medicines (vitamins, analgesics) and assistive devices (spectacles, hearing aids, walking aids), and facilitate referrals. This is the grassroots, community-level arm of NPHCE — the most important for early identification of need.
Tier 2 — Primary Health Centre (PHC): Dedicated elderly clinics (OPDs) held at least once per week; basic screening (blood pressure, blood glucose, weight, vision, hearing, depression, cognitive status); management of stable chronic conditions; referral for complex cases. The PHC is the primary point of organised clinical contact for most rural elderly.
Tier 3 — District Hospital: Dedicated geriatric OPD (at least 2 days per week), dedicated geriatric ward (10 beds minimum), physiotherapy and occupational therapy services, day-care services, and counselling. The district hospital is the secondary referral point and serves as the hub for physiotherapy, specialist medications, and rehabilitation services not available at the PHC.
Tier 4 — Regional Geriatric Centres at Medical Colleges: Eight dedicated regional geriatric centres were established at government medical colleges under NPHCE. Each provides a specialist geriatric OPD, a geriatric ward, a memory clinic, a day hospital, physiotherapy, occupational therapy, social work, and caregiver training. These also serve as training centres for the wider health workforce in geriatric medicine.
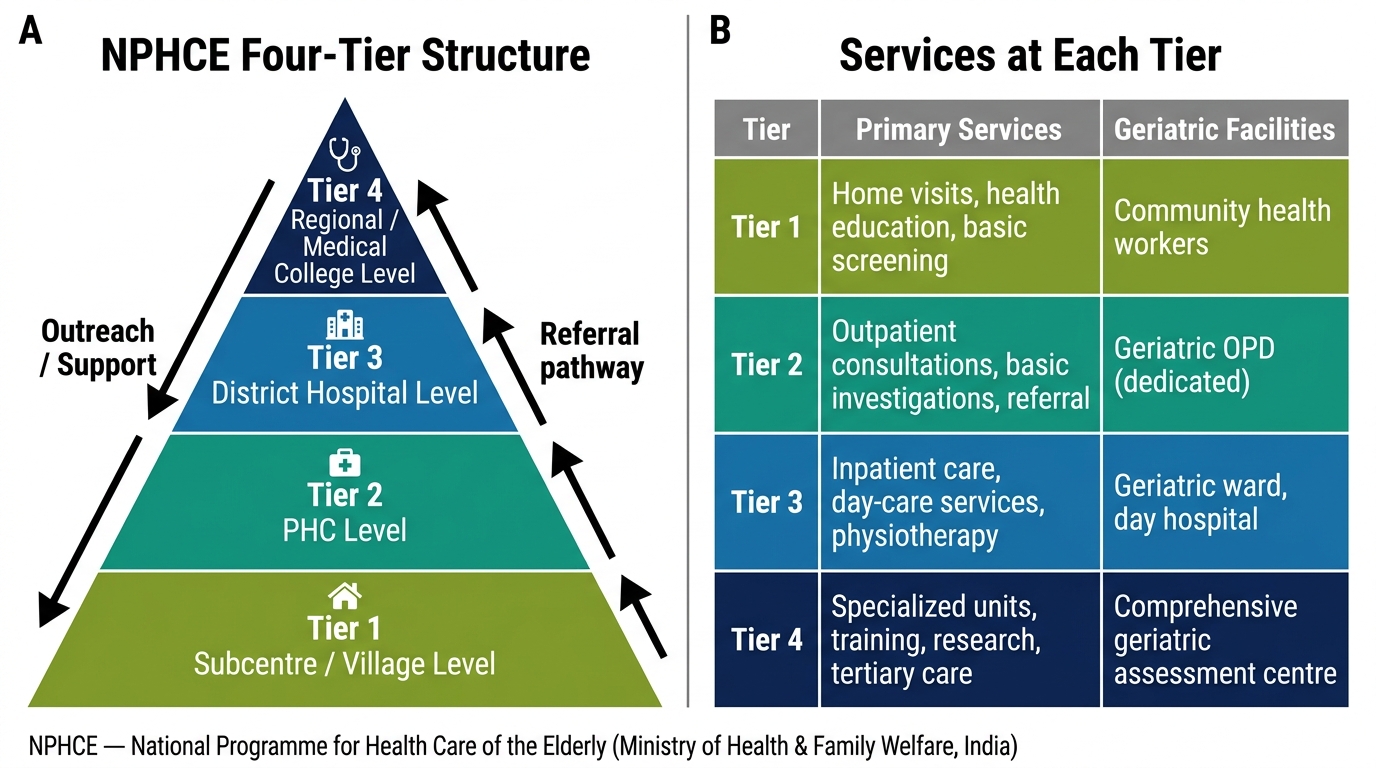
NPHCE Four-Tier Structure and Geriatric Services at Each Level
NPHCE Components and Implementation
Beyond the structural tiers, NPHCE is defined by its specific service components and the implementation mechanisms built into the programme. Understanding these components is important for any doctor who will work within or alongside the NPHCE system.
Dedicated OPDs: The creation of dedicated geriatric OPDs — separate from general medicine — is a foundational NPHCE commitment. The rationale is not luxury but efficiency: elderly patients with multi-morbidity, cognitive impairment, and polypharmacy require longer consultation times, a different clinical approach, and a different team. When elderly patients are managed within general medicine OPDs, time pressure and physician orientation toward single-disease diagnosis produces worse outcomes.
Geriatric wards: Dedicated geriatric wards at district hospitals and regional centres allow nursing staff trained in geriatric care to apply principles that reduce delirium, prevent pressure ulcers, encourage early mobilisation, and manage medication complexity — all of which differ from general medical ward nursing.
Day-care services: Day hospitals — where elderly patients attend for monitoring, physiotherapy, social interaction, and medication review during the day and return home in the evening — reduce the need for hospitalisation, provide caregiver respite, and maintain social engagement. These are particularly important for elderly with Parkinson's disease, post-stroke disability, and early dementia.
Home-based care: For elderly who cannot attend a facility — whether due to disability, distance, or social circumstances — NPHCE mandates ASHA/ANM home visits for monitoring, health education, and basic care. The home visit protocol includes blood pressure measurement, medication adherence check, functional status assessment, and identification of new problems.
Mental health component: Depression and dementia screening are explicitly included in NPHCE's service package, linking it to the National Mental Health Programme. District hospitals and regional centres are expected to provide counselling services and, where needed, referral for psychiatric care.
Caregiver training: NPHCE explicitly includes programmes to train family caregivers in the care of elderly dependents — covering safe mobility assistance, pressure ulcer prevention, medication management, and recognition of emergency signs.
Physiotherapy and occupational therapy: Physiotherapy (mobility, strength, balance) and occupational therapy (ADL training, home modification assessment) are core NPHCE services at the district and regional level. These are among the most cost-effective tertiary prevention interventions in geriatrics.
SELF-CHECK
Under NPHCE, which tier is specifically responsible for conducting house-to-house surveys to identify elderly individuals with health needs in rural areas?
A. Regional geriatric centres at medical colleges
B. District hospital geriatric wards
C. Primary Health Centre elderly OPD
D. Sub-centre and village level (ASHA/ANM)
Reveal Answer
Answer: D. Sub-centre and village level (ASHA/ANM)
NPHCE's Tier 1 — the sub-centre and village level, staffed by ASHAs and ANMs — is responsible for house-to-house surveys, identification of elderly in need, basic health education, distribution of assistive devices, and referral facilitation. This grassroots community outreach is the foundation of the programme's early identification mission. Regional geriatric centres (Tier 4) provide specialist services; district hospitals (Tier 3) provide secondary-level care; PHCs (Tier 2) hold regular elderly OPDs. All are important, but community-level identification begins at Tier 1.
Monitoring NPHCE and Evaluating Elderly Programme Coverage
Evaluating a national programme like NPHCE requires a defined indicator framework covering input, process, output, and outcome measures. Without systematic monitoring, programme funding does not translate into health gains.
Input indicators measure whether the resources are in place: number of dedicated geriatric OPDs established at PHC level (target: all PHCs with elderly OPD at least 1 day/week); number of geriatric wards established at district hospitals (target: minimum 10 beds per district hospital); number of regional geriatric centres operational; number of health workers (ASHAs, ANMs, PHC doctors) trained in elderly care under NPHCE.
Process indicators measure whether the programme is being implemented: number of elderly registered in the NPHCE database per district; percentage of registered elderly receiving an annual comprehensive health check-up; number of elderly receiving physiotherapy sessions; number of assistive devices distributed.
Output indicators measure immediate programme outputs: number of elderly screened for hypertension, diabetes, depression, cognitive impairment; number of referrals made from PHC to district hospital geriatric units; number of home visits made to homebound elderly per ASHA per month.
Outcome indicators measure health impact: prevalence of uncontrolled hypertension in elderly enrolled in NPHCE vs not enrolled; fall-related injury hospitalisation rates; depression detection rates before and after programme implementation; functional status of enrolled elderly (ADL/IADL scores at enrolment vs 12 months).
The key monitoring challenge for NPHCE has been coverage data: while the programme has established physical infrastructure in many states, functional coverage — the proportion of India's 140 million elderly who have actually been screened, assessed, and reached by NPHCE services — remains far below the target. LASI data provide the closest proxy for unmet need, showing that the majority of elderly Indians with NCDs remain undiagnosed or under-treated despite the programme's existence. This gap between infrastructure and coverage is the central monitoring challenge for NPHCE in the current decade.