Page 1 of 11
CM4.1-2 | CM4.1-2 | Methods of Health Education and Counselling — SDL Guide
Learning Objectives
- Describe and classify the major methods of health education with their advantages and limitations (CM4.1)
- Explain how health promotion, education, and counselling activities are organised across individual, family, and community settings (CM4.2)
- Apply the determinants of method selection to choose appropriate health education approaches for given scenarios
INSTRUCTIONS
Every preventable disease in your community has at least one modifiable behaviour at its root — tobacco use, unsafe water, poor antenatal care, vaccine hesitancy. As a future physician, you will spend thousands of hours trying to change those behaviours. This module equips you with the toolbox: a systematic classification of health education methods, the principles that guide method selection, and the structure of counselling as the most evidence-supported individual-level approach. These are not theoretical concepts — they are the skills you will use on your first day in a Field Practice Area.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 27th ed. Ch. 18 — Health Education and Promotion (textbook)
- WHO Ottawa Charter for Health Promotion, 1986 (guideline)
- Nutbeam D. Health Literacy as a Public Health Goal (2000) — Functional, Communicative, Critical literacy framework (framework)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are posted at a sub-centre in rural Rajasthan. The ANM tells you that despite three home visits and a pamphlet about ORS, the mother of a two-year-old with diarrhoea has not changed her practice — she is still giving jeera water instead of ORS. The pamphlet, she says, 'had too many words.' A visiting NGO worker, meanwhile, convinced twelve women at a self-help group meeting to adopt ORS within forty minutes — using a demonstration and a story. Same message, different methods, wildly different outcomes. The difference was not the doctor's knowledge. It was the choice of method.
WHY THIS MATTERS
Health education is the single most cost-effective intervention in public health. Unlike a drug, it works upstream — it prevents the disease before it begins. But its effectiveness is entirely contingent on using the right method for the right audience in the right setting. As a medical officer at a Primary Health Centre, you will design Immunisation Day outreach, conduct ANC counselling, lead village health and nutrition days, and brief panchayat members on sanitation. Each of these demands a different method. Understanding why certain methods work for certain populations — and why others fail — is a core clinical competency, examined in Written, Viva, Skill Assessment, and OSCE formats (CM4.1, CM4.2).
RECALL
Before we classify health education methods, recall two frameworks from your earlier community medicine sessions:
Levels of prevention — Primary (before disease: behaviour change, vaccination), Secondary (early detection: screening), Tertiary (reducing disability). Health education acts predominantly at the primary level.
Epidemiological triad — Host, Agent, Environment. Health education modifies host factors (knowledge, attitudes, practices) and environmental factors (community norms, policy, access). It rarely acts directly on the agent.
Also recall that KAP — Knowledge, Attitude, Practice — is the outcome framework we use to measure behaviour change. A person may gain knowledge but not change attitude; may change attitude but not practice. Effective health education moves people through all three levels.
The Challenge of Behaviour Change: Why Methods Matter
The global burden of preventable disease attributable to modifiable behaviours is staggering. Tobacco use, physical inactivity, unsafe sexual practices, and inadequate antenatal care together account for a majority of premature deaths in low- and middle-income countries. In India, the National Family Health Survey (NFHS-5) data show persistent gaps in health literacy — the capacity to understand, process, and act on health information — particularly in rural and low-education populations. This gap means that simply making information available is insufficient; how information is communicated determines whether behaviour changes.
Health education is defined by Park as 'a process which affects changes in the knowledge, attitudes, and practices of people and aims at improving individual and community health.' The word process is critical: health education is not a one-time event but a sustained, planned engagement that must match its method to its audience. A mass media campaign that works in an urban literacy-rich population may be completely ineffective in a village where most women do not read. A home visit that changes practice for one family cannot scale to a district of 200,000 people. Understanding the burden — the scale and distribution of these behaviour gaps — is what motivates the systematic study of methods that follows in this module.
The Health Belief Model, one of the most widely cited frameworks in health education theory, holds that a person will only adopt a health behaviour if they perceive the disease as serious and personally susceptible, believe the recommended action to be effective, and perceive the barriers to action as manageable. This model implies that different population groups need different educational emphases: some need risk-perception messages, others need barrier-reduction support, and others need practical skill-building. No single method addresses all three, which is why method selection — and the science of matching method to population — is a core public health competency.
SELF-CHECK
According to the Health Belief Model, which factor — if absent — would most likely prevent a person from adopting an ORS practice even after a health education session?
A. Awareness of the correct ORS preparation steps
B. Perceived susceptibility to child mortality from diarrhoea
C. Access to ORS sachets at the sub-centre
D. Perceived severity of dehydration as a disease
Reveal Answer
Answer: B. Perceived susceptibility to child mortality from diarrhoea
The Health Belief Model requires BOTH perceived susceptibility (personal risk) AND perceived severity to motivate action. Without perceived susceptibility — the belief that 'this could happen to my child' — even correct knowledge and available supplies do not translate into action. Options A and C are barriers/enablers, not belief model constructs. Option D (severity) also matters but susceptibility is the answer most directly tied to non-adoption despite education.
Determinants of Effective Health Education Method Selection
Choosing the right health education method is not intuitive — it requires systematic assessment of six key determinants that interact with each other. Understanding these determinants is what separates a public health professional from someone who simply 'gives health talks.'
The first determinant is audience size and homogeneity. Individual methods are appropriate for one-to-one encounters (a patient in an OPD, a postpartum mother in a hospital ward), group methods for audiences of five to thirty people who share a common characteristic (all pregnant women attending ANC, all school children in a class), and mass methods for reaching thousands simultaneously through television, radio, or print. The larger the audience, the shallower the possible depth of individual engagement.
The second determinant is literacy level. In populations with low literacy, print-based materials (pamphlets, posters with extensive text) have minimal impact. Instead, pictorial materials, demonstrations, folk media such as puppet shows and street plays, and audio-visual content via radio or television are far more effective. The functional health literacy concept — reading a medicine label, understanding a prescription — is distinct from general literacy and often lower.
The third determinant is message complexity. Simple messages ('wash hands before eating') can be delivered via mass media. Complex multi-step behaviours (preparing ORS correctly, recognising early dehydration danger signs, knowing when to go to a facility) require interactive methods — demonstration, counselling, or workshop — where questions can be answered and skills can be practised.
The fourth determinant is available resources — personnel (trained health workers, ANMs, ASHAs), time (a two-minute drug-dispensing encounter vs a thirty-minute dedicated session), and materials (flip charts, models, projectors, vehicles for mobile teams). A method that requires a film projector and generator cannot be used in an off-grid village.
The fifth determinant is cultural acceptability. Folk media, local language, gender-concordant health workers, and community-trusted messengers (religious leaders, elder women, self-help group leaders) all affect whether a message is received or rejected. A demonstration conducted by a male health worker among an exclusively female audience may be less effective than one conducted by a female ANM.
The sixth determinant is setting — whether the activity takes place in a clinic (where patients already seek care), a home (intimate, family-inclusive, trust-building), a school (captive young audience), a workplace (adult learners with common occupational risks), or a community space (community meetings, village health days). Each setting has its own social norms, power dynamics, and constraints that shape which methods are feasible.
Classification of Health Education Methods
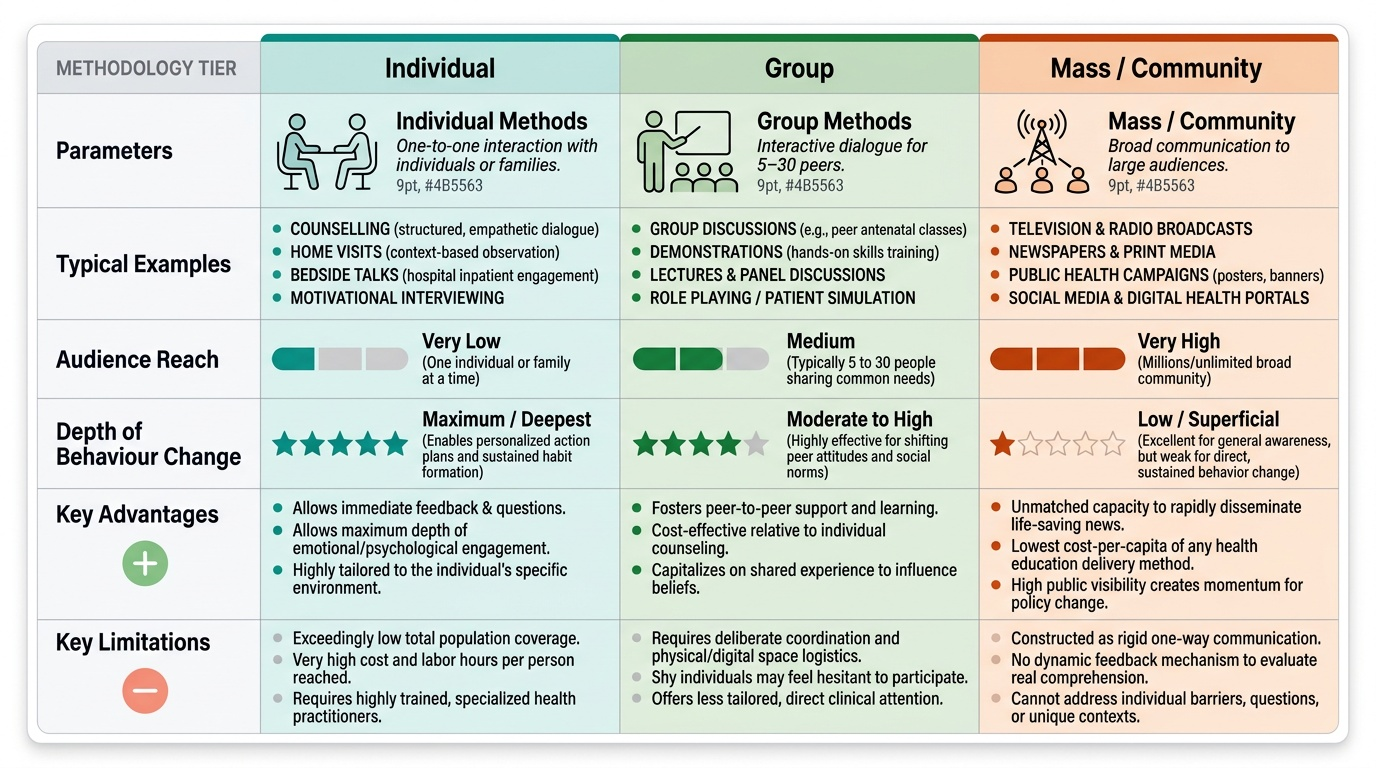
Health education methods are best classified by the size and directness of the audience they reach. Park's Textbook organises them into three tiers: individual, group, and mass (or community-level) methods. This is the classification that NMC examinations follow, and it directly maps onto the strengths and limitations of each approach.
Individual methods are one-to-one interactions between a health worker (doctor, nurse, ANM, ASHA, or counsellor) and a single person or family. The cardinal individual methods are: (a) counselling — a structured, empathetic, two-way communication process aimed at helping a person understand their health situation and make an informed decision; (b) home visits — allowing the health worker to assess the environment, observe practices, and address barriers in the person's own context; (c) bedside talks — used during hospital admission when the patient and family are captive and often highly motivated; and (d) motivational interviewing — a patient-centred counselling style that elicits and strengthens the person's own motivation to change. Advantages: maximum depth of engagement, feedback and questions possible, behaviour change often sustained. Limitations: very low reach (one person at a time), high resource cost per capita, requires trained personnel.
Group methods reach five to thirty people who share a common characteristic or health need. The principal group methods are: (a) group discussion — a facilitated dialogue among peers, effective for attitude change (antenatal groups discussing breastfeeding); (b) lecture with discussion — didactic but more scalable than individual; (c) demonstration — showing how to perform a skill (ORS preparation, hand-washing technique, contraceptive use), followed by re-demonstration by participants (return demonstration); (d) role play and drama — used in schools and communities to simulate health scenarios and rehearse responses; (e) symposium and panel discussion — expert-led, for educated audiences; (f) workshop and training — intensive skill-building over multiple sessions; (g) peer education — trained community members educate their peers (highly effective for adolescent reproductive health). Advantages: social reinforcement of norms, peer influence, moderate depth of learning, scalable to cluster level. Limitations: limited reach, requires organisation and a venue, group dynamics can be challenging.
Mass/community methods communicate with thousands or millions simultaneously. These include: (a) mass media — television (health shows, public service announcements), radio (community FM, AIR health spots), print (newspapers, magazines); (b) printed materials — posters (designed for public display at health facilities, schools, anganwadis), pamphlets and leaflets (take-home), flip charts (used by health workers during home visits); (c) social media and digital platforms — WhatsApp health messages, YouTube videos, government apps (Aarogya Setu, Poshan Tracker); (d) folk media — puppet shows, street plays (nukkad nataks), folk songs, magic shows with health messages, which are culturally resonant in rural India; (e) exhibitions and health fairs — at melas, community events. Advantages: very high reach, cost-effective per person, raises awareness rapidly. Limitations: shallow engagement, no individual feedback possible, literacy-dependent for print, cannot address complex skills, prone to misinterpretation.
Provided image