Page 1 of 8
CM18.1-3 | CM18.1-3 | International Health Agencies and Pandemic Prevention — SDL Guide
Learning Objectives
- Define international health and explain why health problems require multilateral responses
- Describe the mandate, headquarters, and key programmes of the major international health agencies (WHO, UNICEF, World Bank, USAID, GAVI, Global Fund)
- Explain the IHR 2005 framework, the PHEIC declaration process, and WHO's role in pandemic prevention
- Describe India's position within the international health architecture and its obligations under IHR 2005
INSTRUCTIONS
Infectious diseases, nutritional crises, and environmental hazards do not respect national borders. The COVID-19 pandemic, the 2014 Ebola epidemic, and resurgent polio all demonstrated that a health event anywhere can become a health emergency everywhere. This module maps the international architecture that coordinates the global response — the agencies, legal frameworks, and surveillance systems that India is embedded in and that shape how you will practise public health.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 19 — International Health (textbook)
- WHO. International Health Regulations (2005), 3rd ed. Geneva: World Health Organization; 2016 (document)
- WHO. World Health Statistics 2023. Geneva: WHO; 2023 (document)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is January 2020. A cluster of pneumonia cases of unknown aetiology has been reported from Wuhan, China. Within days, cases appear in Thailand and Japan. On 30 January 2020, the WHO Director-General convenes an Emergency Committee and declares a Public Health Emergency of International Concern (PHEIC) — only the sixth in the history of the IHR 2005 framework. Forty days later, on 11 March 2020, WHO upgrades the declaration to a pandemic. The speed of this cascade — from local cluster to PHEIC in under a month — reflects both the pace of modern spread and the machinery of international health that exists to detect and respond to it. As a community medicine physician, you will need to understand who does what in this architecture, and how India is plugged into it.
WHY THIS MATTERS
Understanding international health agencies is not an academic exercise. These organisations directly shape the vaccines in India's immunisation schedule (GAVI co-finances EPI vaccines), the disease surveillance protocols your district office follows (IHR 2005 mandates), the essential medicines on your PHC formulary (WHO EML influences NLEM), and the outbreak protocols activated during any public health emergency. As a medical officer, you will interact with the outputs of these agencies every working day even if you never attend an international meeting.
RECALL
Before proceeding, activate what you already know. From your studies of primary health care (CM cluster: Healthcare of the Community), recall the Alma-Ata Declaration and its emphasis on primary health care as the foundation of health for all. Recall from your disease surveillance module that India operates the Integrated Disease Surveillance Programme (IDSP), which interfaces with the WHO surveillance network. Recall from your health planning module the concept of Universal Health Coverage (UHC) — now a global SDG target co-monitored by WHO and World Bank. These national systems are nodes in a global network; this module explains the network itself.
Global Disease Burden and the Need for International Cooperation
International health is defined as the branch of public health that addresses health issues and determinants that transcend national boundaries, requiring cooperative multilateral action. Park (2021) defines it as 'the application of the principles and practice of public health to the special problems arising from the international movements of people, products and vectors of diseases, and to the problems of health in different countries.' The rationale for international cooperation is anchored in a fundamental epidemiological reality: pathogens do not respect geopolitical borders.
The global burden of communicable and non-communicable diseases is strikingly unequal. Low- and middle-income countries (LMICs) bear approximately 80% of the global communicable disease burden while possessing fewer than 20% of global health resources. Malaria kills over 600,000 people annually — almost all in sub-Saharan Africa — yet the pathogen circulates wherever competent Anopheles vectors and susceptible hosts coexist, including India's northeastern states. Influenza pandemics originating in animal reservoirs in East Asia have historically reached every inhabited continent within weeks of emergence. Drug-resistant tuberculosis strains evolving in one country travel with mobile populations. Zoonotic spillover events — where pathogens jump from animal reservoirs to humans — are increasingly frequent as habitat encroachment and live-animal trade expand.
Beyond communicable diseases, climate change, industrial pollution, and trade in food and pharmaceuticals create shared health threats that no single nation can address in isolation. The post-World War II consensus that recognised these realities led to the creation of a multilateral health architecture, beginning with the WHO in 1948. Every subsequent international health crisis — SARS 2003, H1N1 2009, Ebola 2014, COVID-19 2020 — has refined and stress-tested that architecture.
For India specifically, international cooperation is not optional. India is part of the WHO South-East Asia Regional Office (SEARO) and is legally bound by IHR 2005. India's pharmaceutical sector supplies approximately 20% of global generic medicines by volume, making Indian drug quality a matter of international health security. India's eradication of polio in 2014 was a achievement of coordinated international surveillance and vaccination campaigns. Understanding the architecture that made these outcomes possible is a clinical and public health competency.
Determinants of International Health Inequity
The determinants that drive differential disease burden between nations operate across biological, social, economic, political, and environmental domains. Understanding these determinants is essential to appreciating why international agencies exist and what they must address beyond simple disease control.
Socio-economic determinants are the most powerful. Per capita income, education, and access to safe water and sanitation explain more variance in life expectancy across countries than any single disease-specific intervention. The World Bank's Human Capital Index quantifies how much of a child's potential productivity is lost to poor health and inadequate education — a composite determinant that international agencies use to prioritise investment. Countries in the lowest income quintile have under-five mortality rates 15–20 times those of high-income countries, predominantly from preventable and treatable conditions.
Political determinants include governance quality, health system financing, and the prioritisation of health in national budgets. Fragile and conflict-affected states bear a disproportionate burden of communicable diseases because their health systems collapse during conflict and rebuild slowly. The social determinants of health — income inequality, gender inequity, racial discrimination, and urban-rural disparities — shape who gets sick and who recovers. WHO's Commission on Social Determinants of Health (2008) documented that these upstream factors are responsible for the bulk of avoidable health inequity between and within countries.
Environmental determinants include climate-driven changes to vector habitats, air and water pollution from industrial activity, and occupational exposures that differ vastly between high-income and low-income country workforces. The emergence and re-emergence of zoonotic diseases is a direct determinant shaped by deforestation, land-use change, and live-animal markets — all of which concentrate in specific geographies with weak regulatory environments.
For international agencies, these determinants demand interventions far beyond medical care — encompassing trade policy, debt relief, technology transfer, and diplomatic engagement. The Sustainable Development Goals (SDGs), adopted in 2015, operationalise this multi-determinant framework by embedding health (SDG 3) within a matrix of goals addressing poverty, hunger, gender, climate, and governance. The SDG framework is jointly monitored by WHO, UNICEF, World Bank, UNDP, and UNFPA — each agency tracking the determinants within its mandate.
SELF-CHECK
Which international legal framework obligates all WHO member states — including India — to report potential Public Health Emergencies of International Concern within 24 hours of risk assessment?
A. The Alma-Ata Declaration (1978)
B. The International Health Regulations 2005 (IHR 2005)
C. The Ottawa Charter for Health Promotion (1986)
D. The Doha Declaration on TRIPS and Public Health (2001)
Reveal Answer
Answer: B. The International Health Regulations 2005 (IHR 2005)
The International Health Regulations 2005 (IHR 2005) is the legally binding framework under which 196 states parties — essentially all WHO member states — are obligated to report events that may constitute a PHEIC. The Alma-Ata Declaration and Ottawa Charter are non-binding policy documents; the Doha Declaration concerns pharmaceutical patents and access to medicines, not disease notification.
Architecture of International Health Agencies
The international health architecture comprises four broad tiers of organisations, each with distinct mandates, governance structures, and modes of operation. Familiarity with this architecture prevents confusion about who is accountable for what during a health emergency.
Tier 1 — UN-affiliated multilateral bodies: The World Health Organization (WHO), established 7 April 1948 (celebrated as World Health Day), is the directing and coordinating authority on international health within the UN system, headquartered in Geneva, Switzerland. WHO is governed by the World Health Assembly (WHA), comprising representatives of all 194 member states, which meets annually. WHO's core functions include norm-setting (guidelines, standard-setting), surveillance (Global Outbreak Alert and Response Network, GOARN), technical assistance, and the IHR 2005 framework. UNICEF (United Nations Children's Fund), headquartered in New York, focuses on child and maternal health, nutrition, and education. UNICEF co-leads GOBI-FFF (Growth monitoring, Oral rehydration, Breastfeeding, Immunisation — Female education, Family spacing, Food supplementation) and is a major partner in global immunisation through GAVI. UNFPA (United Nations Population Fund), headquartered in New York, addresses reproductive health, family planning, and safe motherhood. UNDP (United Nations Development Programme), headquartered in New York, leads the human development index and the SDG monitoring framework, acting at the development-health interface. The World Bank, headquartered in Washington DC, is the world's largest single financier of health programmes in LMICs — providing loans, grants, and technical assistance — and co-leads UHC tracking with WHO.
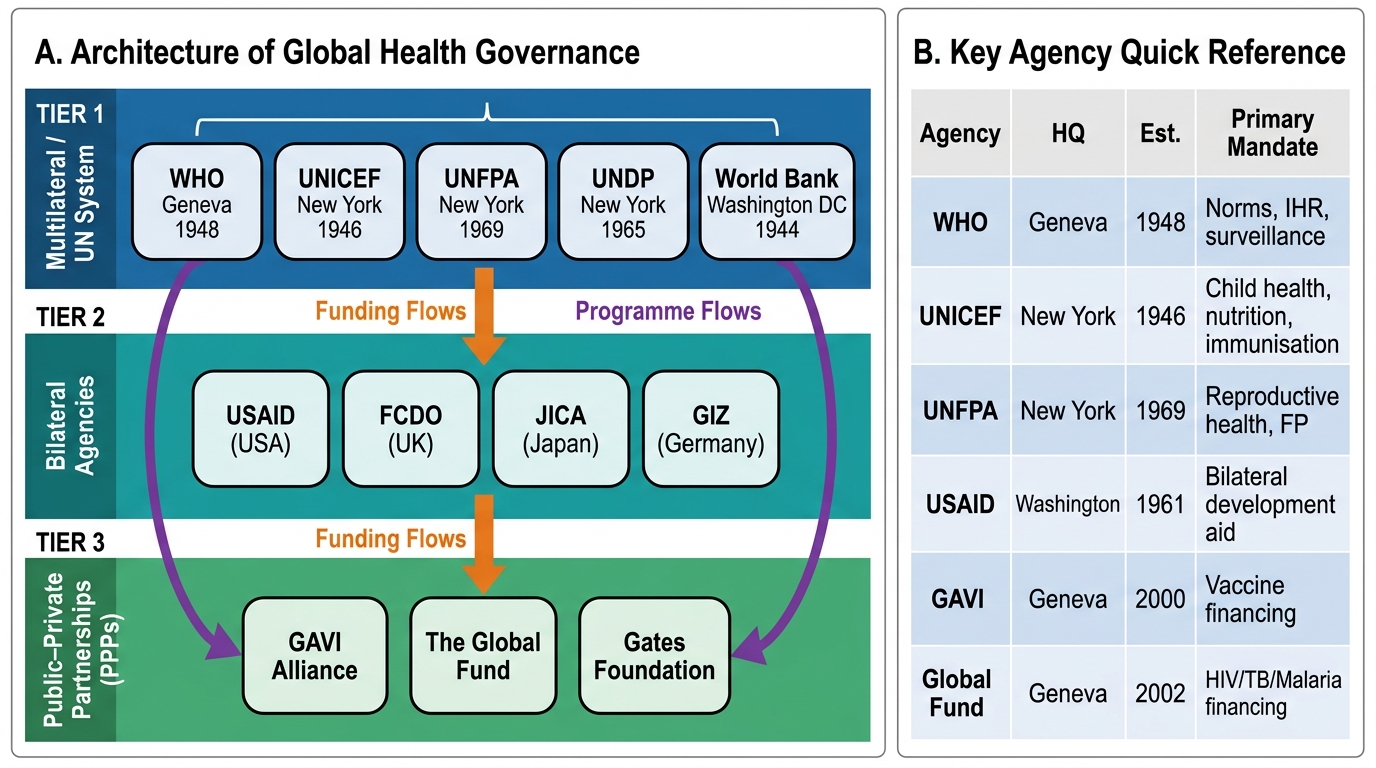
Fig. 1 — Architecture of International Health Governance: Three-Tier Organisational Framework and Funding Flows
| Agency | HQ City | Est. Year | Primary Health Mandate | India Programme Example |
|---|---|---|---|---|
| WHO | Geneva | 1948 | International health norm-setting, IHR, disease surveillance | Technical support for IDSP, NTEP, NPPCF; SEARO regional office in New Delhi |
| UNICEF | New York | 1946 | Child and maternal health, nutrition, immunisation | Universal Immunisation Programme support, nutrition surveillance, WASH |
| UNFPA | New York | 1969 | Reproductive health, family planning | Family planning under NHM, maternal health, obstetric care |
| UNDP | New York | 1965 | Development-health nexus, SDG monitoring | Human Development Index reporting for India, SDG 3 tracking |
| World Bank | Washington DC | 1944 | Health financing, loans, technical assistance | PMGSY, National Health Mission components, loan-funded health projects |
Tier 2 — Bilateral agencies: USAID (United States Agency for International Development) funds major disease programmes including the President's Emergency Plan for AIDS Relief (PEPFAR) and the President's Malaria Initiative (PMI). The UK's FCDO (Foreign, Commonwealth and Development Office, formerly DFID) provides bilateral health assistance. Germany's GIZ (Deutsche Gesellschaft für Internationale Zusammenarbeit) supports health systems strengthening. Japan's JICA supports health through technical cooperation.
Tier 3 — Public-private partnerships (PPPs): GAVI, the Vaccine Alliance (established 2000, Geneva) is a PPP that increases access to new vaccines for LMICs — co-financed by donor governments, vaccine manufacturers, WHO, UNICEF, World Bank, and the Bill & Melinda Gates Foundation. GAVI co-finances pentavalent and pneumococcal vaccines in many LMICs. The Global Fund to Fight AIDS, Tuberculosis and Malaria (established 2002, Geneva) is a financing mechanism that channels grants to country-led programmes — India has received Global Fund support for TB and HIV programmes. The Bill & Melinda Gates Foundation is the world's largest private philanthropic health funder.
Tier 4 — WHO Regional and Country Offices: WHO is organised into 6 regional offices. India falls under SEARO — WHO South-East Asia Regional Office, headquartered in New Delhi. SEARO comprises 11 member states and coordinates regional surveillance, technical support, and response.