Page 2 of 8
CM18.1-3 | CM18.1-3 | International Health Agencies and Pandemic Prevention — SDL Guide (Part 2)
WHO, IHR 2005 and Pandemic Prevention
The legal cornerstone of international pandemic prevention is the International Health Regulations 2005 (IHR 2005), which entered into force on 15 June 2007 and is legally binding on 196 states parties — a larger number than WHO's 194 member states, which is unique. IHR 2005 replaced the previous International Sanitary Regulations, expanding the scope from three specific diseases (cholera, plague, yellow fever) to any event that may constitute a Public Health Emergency of International Concern (PHEIC).
A PHEIC is defined as 'an extraordinary event which is determined to constitute a public health risk to other States through the international spread of disease and to potentially require a coordinated international response.' The PHEIC decision is made by the WHO Director-General, based on information from state parties and advice from an Emergency Committee (experts convened under IHR Article 48). Four criteria must be met: (1) the event is serious, unusual or unexpected; (2) there are implications for public health beyond the affected state; (3) immediate international action may be required; (4) the event may require a coordinated international response. Since IHR 2005 entered into force, PHEICs have been declared for: H1N1 influenza (April 2009), polio (May 2014), Ebola West Africa (August 2014), Zika virus (February 2016), Kivu Ebola (July 2019), COVID-19 (January 2020), mpox (July 2022, re-declared August 2024).
Under IHR 2005, state parties have core capacity obligations: surveillance, risk assessment, notification, verification, response, and communication. India must notify WHO within 24 hours of assessing that an event may constitute a PHEIC. The national focal point for IHR in India is the National Centre for Disease Control (NCDC) under the Directorate General of Health Services (DGHS), and the IDSP serves as the primary surveillance platform.
WHO's operational pandemic response is coordinated through GOARN — the Global Outbreak Alert and Response Network — a collaboration of over 250 technical institutions worldwide that can rapidly deploy outbreak response teams. GOARN provided surge capacity during Ebola (2014), COVID-19 (2020), and other emergencies.
Pandemic prevention — not just response — requires sustained investment in: (a) animal-human interface surveillance (One Health approach: WHO, FAO, WOAH/OIE working together); (b) genomic sequencing capacity to detect novel variants; (c) IHR core capacity building in countries that lack robust surveillance; (d) vaccine development platforms (WHO's R&D Blueprint, CEPI). The re-emergence of diseases like mpox and Marburg demonstrates that the pandemic prevention architecture is continuously tested.
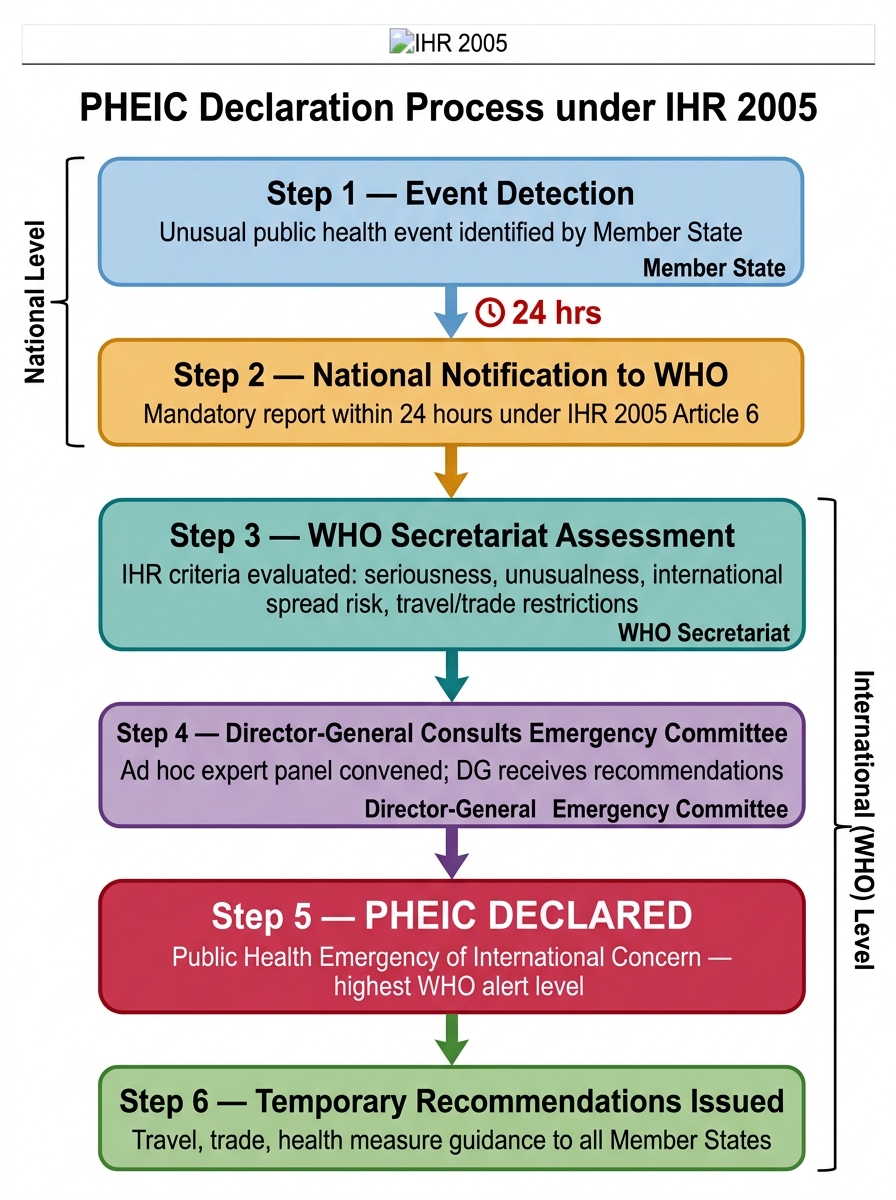
PHEIC Declaration Process under IHR 2005
SELF-CHECK
India belongs to which WHO Regional Office, and where is that office headquartered?
A. EMRO — Cairo, Egypt
B. SEARO — New Delhi, India
C. WPRO — Manila, Philippines
D. AFRO — Brazzaville, Republic of Congo
Reveal Answer
Answer: B. SEARO — New Delhi, India
India is part of the WHO South-East Asia Regional Office (SEARO), which is headquartered in New Delhi, India. SEARO covers 11 member states including India, Bangladesh, Bhutan, Sri Lanka, Nepal, Myanmar, Maldives, Indonesia, Thailand, Timor-Leste, and the Democratic People's Republic of Korea.
Evaluating Agency Effectiveness and Accountability
International health agencies are accountable to their member states, donors, and the populations they serve — but the mechanisms of accountability differ considerably across agency types. Understanding how effectiveness is evaluated is important for a community medicine physician who will read agency reports and apply their guidelines.
WHO's accountability framework operates through the World Health Assembly, which receives the biennial budget, the Director-General's report, and evaluation reports from the independent Joint Inspection Unit and the WHO Programme Budget Web Portal. WHO's performance is monitored against the Thirteenth General Programme of Work (GPW13) targets: triple billion goals — 1 billion more people benefiting from universal health coverage, 1 billion more better protected from health emergencies, 1 billion more enjoying better health and well-being. Progress is measured through the WHO Health Statistics annual report and the SDG 3 monitoring framework.
UHC tracking is conducted jointly by WHO and the World Bank using the UHC Service Coverage Index (SCI) — a composite of 14 tracer interventions covering reproductive health, child health, infectious diseases, and non-communicable diseases. India's SCI was 61 in 2021 (global average 68), reflecting significant but incomplete coverage.
SDG monitoring provides a cross-agency accountability structure. SDG 3 (Good Health and Well-being) has 13 targets and 28 indicators, monitored by WHO as custodian. Progress is reported to the UN High-Level Political Forum annually, providing a platform for public accountability.
The Independent Panel for Pandemic Preparedness and Response (IPPPR), convened after COVID-19, evaluated the IHR framework and found critical gaps: delayed PHEIC declaration, under-investment in core capacities, and fragmented global response. Its 2021 report recommended a Pandemic Treaty (now being negotiated as the WHO Pandemic Accord) and strengthened IHR amendments (agreed May 2024). This iterative process of evaluation → reform → implementation → re-evaluation is how the international health architecture evolves.
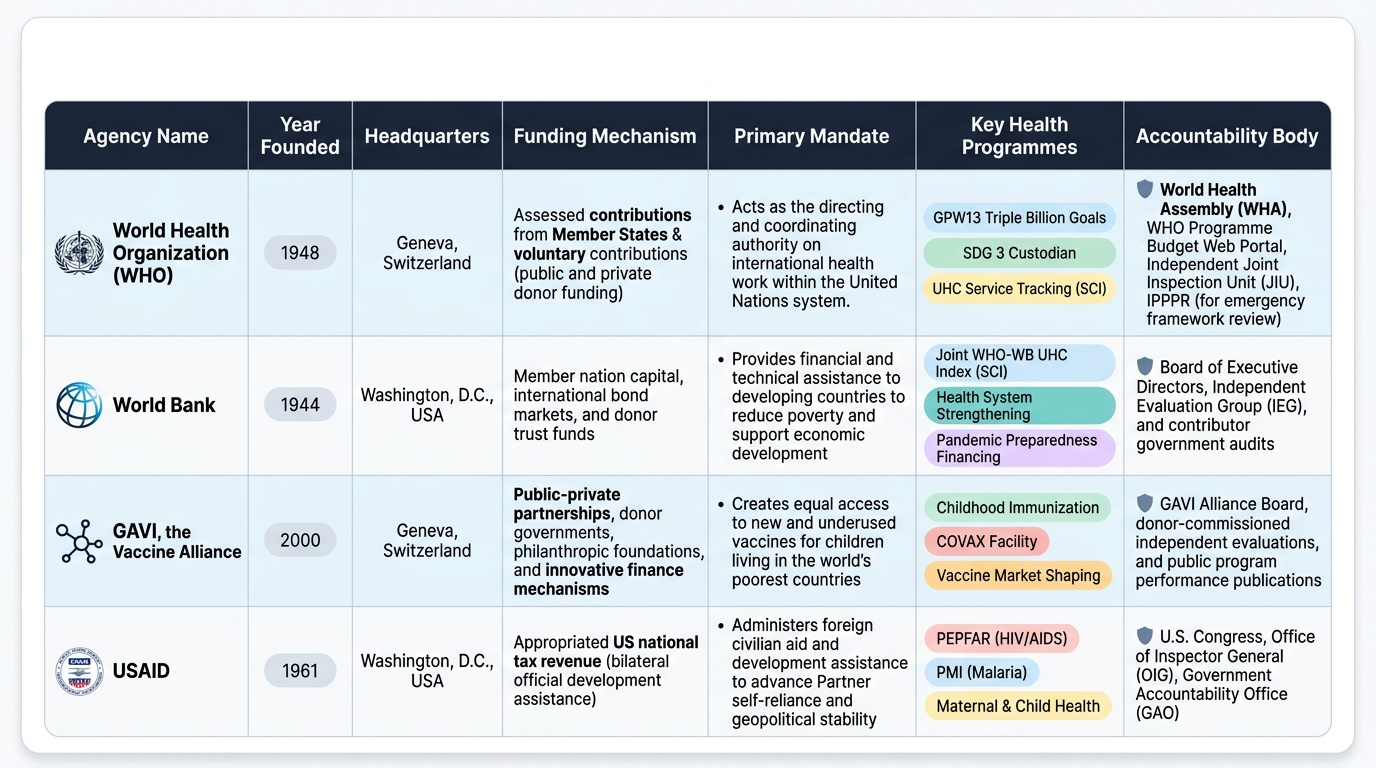
For bilateral agencies and PPPs, effectiveness is evaluated through independent evaluations commissioned by boards and donor governments. GAVI publishes programme evaluations measuring vaccine coverage and equity; the Global Fund uses a performance-based funding model where grants are disbursed based on results verification.
Provided image
CLINICAL PEARL
The WHO's PHEIC declaration is sometimes described as 'the highest level of alarm' in global health — but it carries no enforcement power. WHO can issue Temporary Recommendations (e.g., 'do not implement travel bans') under IHR Article 15, but compliance is voluntary. The COVID-19 pandemic exposed this gap: many countries imposed travel bans contrary to WHO recommendations within days of the PHEIC declaration. This is why community medicine physicians must understand that international frameworks are coordination tools, not command-and-control systems — effective implementation depends on national political will and health system capacity. India's IDSP-to-NCDC-to-DGHS-to-WHO reporting chain is the operational interface between the international obligation and the field.
India in the International Health Architecture
India's engagement with the international health architecture is both as a recipient of technical and financial assistance and as an increasingly significant contributor to global health.
As a SEARO member state, India benefits from WHO's regional technical support across disease programmes. SEARO's priority diseases — dengue, tuberculosis, antimicrobial resistance, vaccine-preventable diseases — are also India's priority diseases. India's National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases, and Stroke (NPCDCS) has received WHO technical input; the National TB Elimination Programme (NTEP) operates with WHO/Global Fund technical and financial support.
Under IHR 2005, India has developed its core capacities through IDSP — which serves as the primary alert system — and the National Centre for Disease Control (NCDC), which is designated as the national IHR focal point. India conducts IHR Joint External Evaluations (JEEs) — voluntary multisectoral assessments of IHR core capacity — and has committed to annual reporting on the SPAR (State Party Annual Report) tool.
India's pharmaceutical contribution to international health is substantial: approximately 20% of global generic medicine exports by volume originate in India, making WHO Good Manufacturing Practice (GMP) compliance and CDSCO regulatory capacity matters of international consequence. India is a major supplier to the UNICEF Supply Division and the Global Fund medicine procurement programmes.
India has also emerged as a vaccine manufacturing hub of global significance. The Serum Institute of India (SII) in Pune is the world's largest vaccine manufacturer by number of doses — producing vaccines for GAVI-eligible countries including OPV, pentavalent, and COVID-19 vaccines (Covishield). During COVID-19, India's 'Vaccine Maitri' initiative exported over 65 million doses to 95 countries before domestic supply pressures required a pause — a demonstration of both India's capacity and the tension between national and global health priorities.
For the graduating community medicine physician, the practical application is this: every district has an IDSP unit that reports to the state and national level, which ultimately flows to WHO. Knowing the chain — disease event in field → IDSP reporting unit → state surveillance unit → NCDC → DGHS (national IHR focal point) → WHO SEARO → WHO Geneva — allows you to understand where your local reports land in the global architecture.
SELF-CHECK
GAVI, the Vaccine Alliance is a public-private partnership that co-finances vaccines for low- and middle-income countries. Which of the following is NOT among GAVI's founding partners?
A. Bill & Melinda Gates Foundation
B. UNICEF
C. International Monetary Fund (IMF)
D. World Bank
Reveal Answer
Answer: C. International Monetary Fund (IMF)
GAVI was co-founded in 2000 by the Bill & Melinda Gates Foundation, WHO, UNICEF, and the World Bank, along with vaccine manufacturers and donor governments. The International Monetary Fund (IMF) is a financial institution focused on macroeconomic stability and does not participate in health programming or vaccine procurement — it is not a GAVI founding partner.