Page 1 of 8
CM15.1-4 | CM15.1-4 | Mental Health Recognition and Programme Response — SDL Guide
Learning Objectives
- Define mental health using the WHO framework and distinguish it from the mere absence of disease
- Describe the epidemiological burden of mental disorders in India using NMHS 2016 data
- Identify warning signals of mental health disorders across affective, psychotic, substance-use, and somatoform categories
- Explain the objectives, structure, and delivery of the National Mental Health Programme (NMHP) and the District Mental Health Programme (DMHP)
- Describe the key provisions of the Mental Healthcare Act 2017 and their implications for community practice
- Apply a structured recognition-and-referral approach for mental health problems at the individual, family, and community level
INSTRUCTIONS
Mental health is no longer a specialist-only domain — primary care doctors and community health workers are the first point of contact for the majority of people with mental disorders in India. Yet the treatment gap exceeds 80%, meaning most people who need help never receive it. This module equips you with the epidemiological lens to understand the burden, the clinical eye to recognise warning signals early, and the programme knowledge to activate the national response machinery (NMHP/DMHP/MHCA 2017) when you encounter mental health problems in community practice.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 27th ed., Ch. 22 — Mental Health (textbook)
- National Mental Health Survey of India 2015–16 (NIMHANS, Govt of India) (report)
- Mental Healthcare Act 2017 (Act No. 10 of 2017), Ministry of Law and Justice, Govt of India (legislation)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rupa is a 34-year-old schoolteacher in a small town in Rajasthan. Over the past three weeks her husband has noticed she barely speaks, refuses meals, and repeatedly says 'there is no point in living.' The local ASHA worker visits and is unsure whether this is grief — Rupa lost her mother two months ago — or something more serious. She calls the Primary Health Centre doctor for advice. The doctor asks: Is Rupa just sad, or is she in danger? How do I recognise the difference? What services exist in my district? And what are Rupa's rights under the law? This session answers all four questions — and by the end, you will know exactly what to do when you are in the doctor's position.
WHY THIS MATTERS
Mental health conditions are among the most prevalent, disabling, and undertreated health problems in India. Unlike infectious diseases, they leave no laboratory footprint and carry no fever — so they remain invisible until a crisis forces attention. As a community medicine doctor you will encounter depression, psychosis, alcohol dependence, and developmental disorders in outpatient queues, school health programmes, and antenatal clinics — often undiagnosed and untreated. The National Mental Health Programme specifically assigns primary care doctors a central role in detection and first-line management. Understanding the burden data, recognising warning signals, and knowing how to activate programme resources will make you directly effective in reducing the 80–85% treatment gap that Park calls 'the most glaring indicator of health system failure in this domain.'
RECALL
Before we begin, draw on what you already know. From your Physiology block, recall that emotional regulation involves the limbic system — the amygdala (threat appraisal), hippocampus (contextual memory), and prefrontal cortex (executive control). Disruption of monoamine neurotransmitters (serotonin, dopamine, noradrenaline) is central to most mood and psychotic disorders. From community medicine's social medicine unit, recall that poverty, domestic violence, migration, caste discrimination, and gender inequality are powerful social determinants of ill-health — including mental ill-health. These upstream determinants explain why mental disorders cluster in marginalised communities. Now layer on the Public Health Systems structure: the three-tier Primary-Community-District hospital network is the same infrastructure through which DMHP delivers mental health services. Keep this structural picture in mind as we build the mental health programme logic.
Magnitude of the Mental Health Burden
Understanding the scale of mental ill-health in India requires moving beyond clinical impressions to systematic epidemiology. The National Mental Health Survey (NMHS) 2016 — the largest nationally representative household survey of its kind, sampling 34,802 adults across 12 Indian states — remains the authoritative reference. Its headline finding: the lifetime prevalence of mental disorders among Indian adults is approximately 13.7%, with a current (past-year) prevalence of 10.6%. Breaking this down by category reveals the distribution: common mental disorders (depression, anxiety, somatoform disorders) account for the largest share at a combined current prevalence approaching 10.6%; alcohol and substance use disorders affect approximately 4.6% of adults in their lifetime; severe mental disorders including schizophrenia, bipolar disorder, and other psychoses have a lifetime prevalence of approximately 1.9%, placing some 15 million Indians in this category alone; and developmental disorders including autism spectrum conditions and intellectual disabilities contribute additional burden particularly in childhood. Two findings from NMHS are especially important for community medicine practice. First, the treatment gap — the proportion of people with a diagnosable mental disorder who receive no treatment — stands at 80–85% for most disorder categories in India. This means four in every five people with depression or schizophrenia in India receive no professional care. Second, the urban–rural distribution shows that rural populations are not protected: rural prevalence for common mental disorders is substantial, and access to specialist services is far more restricted. Globally, the WHO GBD data rank depression as the single largest cause of disability worldwide, contributing more years lived with disability than any physical condition.
The WHO definition of mental health — established in 2001 and affirmed in subsequent frameworks — defines mental health not as the absence of mental disorder but as 'a state of well-being in which every individual realises their own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to their community.' This definition has three clinical implications: (1) mental health is a positive attribute, not merely the absence of pathology; (2) it exists on a continuum — the same person can move between mental health and ill-health over time depending on life circumstances; and (3) it is both a right and a social responsibility, which is the philosophical foundation of the NMHP.
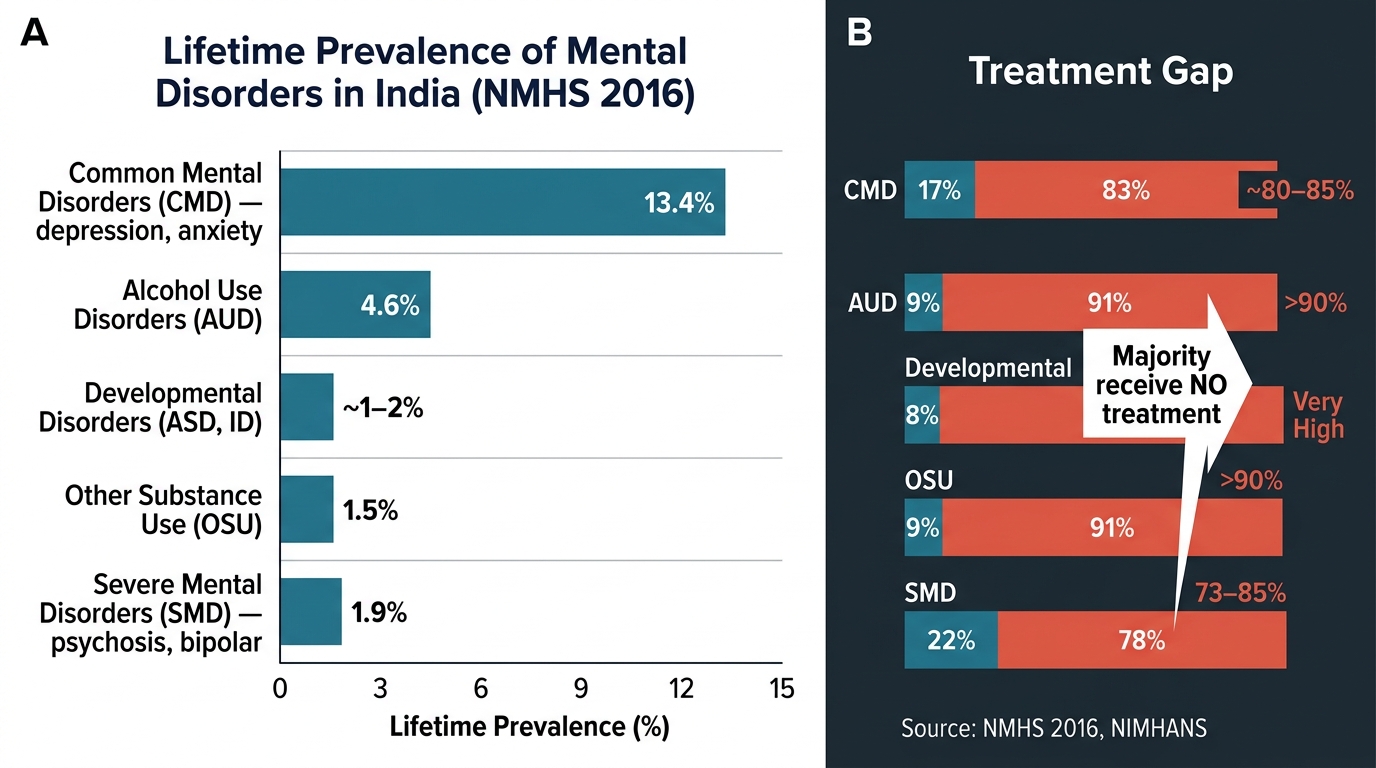
Burden and Treatment Gap for Mental Disorders in India — NMHS 2016
| Category | Lifetime Prevalence (NMHS 2016) | Treatment Gap |
|---|---|---|
| Common mental disorders (depression, anxiety) | ~13.4% | ~80–85% |
| Severe mental disorders (psychosis, bipolar) | ~1.9% | ~73–85% |
| Alcohol use disorders | ~4.6% | >90% |
| Other substance use | ~1.5% | >90% |
| Developmental disorders (ASD, ID) | 1–2% (est.) | Very high |
Determinants of Mental Health and Ill-health
Mental disorders do not arise from biology alone — they emerge from the intersection of biological vulnerability, psychological experience, and social context. The social determinants of mental health are the upstream conditions that explain why some populations carry disproportionate burden. Park's framework, aligned with the WHO Commission on Social Determinants of Health, identifies the following major categories.
Socioeconomic determinants are the most consistently documented. Poverty operates through material deprivation (poor nutrition, overcrowding), chronic stress (financial insecurity, debt cycles), and reduced help-seeking (cost of treatment, lack of insurance). In India, studies consistently show that households below the poverty line have two to three times the prevalence of depression compared with higher-income groups. Gender is a pervasive determinant: women in India have higher rates of common mental disorders (depression, anxiety) and are disproportionately affected by intimate partner violence, which independently predicts poor mental health outcomes. Men, conversely, have higher rates of alcohol dependence and suicide completion. Migration and displacement — whether internal (rural-to-urban labour migration) or forced (natural disasters, conflict) — disrupt social support networks, expose migrants to discrimination and precarious housing, and are associated with elevated psychosis and depression rates. Caste discrimination and social exclusion add further risk, operating via chronic psychological stress, restricted livelihood options, and internalized stigma.
Biological determinants include genetic predisposition (heritability of schizophrenia is approximately 80%, bipolar disorder approximately 70%), prenatal infections and nutritional deficiencies, birth complications (perinatal hypoxia as a risk for schizophrenia), and chronic physical illness (diabetes, hypothyroidism, HIV and antiretroviral drugs can cause mood syndromes). Psychological determinants include adverse childhood experiences (ACEs — abuse, neglect, parental mental illness), attachment disruption, and maladaptive coping styles.
Protective factors are equally important for programme design: strong social support networks, social cohesion, employment, education, access to green space, religious/spiritual community, and early access to appropriate care all buffer against mental disorder. NMHP's community-based approach is explicitly designed to leverage these protective factors — strengthening community capacity rather than medicalising distress.
Warning Signals of Mental Health Disorders
Recognising a mental health problem early is a critical clinical skill that can be exercised without specialist training. Warning signals are early, recognisable changes in behaviour, emotion, thought, or function that suggest the onset of a mental disorder — they are not diagnostic criteria, but they prompt further assessment and timely referral. The community doctor's role is to recognise these signals and act, not to make a DSM or ICD diagnosis.
For affective disorders (depression, anxiety, bipolar disorder) — by far the most common category — the key warning signals are: persistent sadness or emptiness lasting more than two weeks that does not respond to reassurance; loss of interest or pleasure in previously enjoyed activities (anhedonia); significant changes in sleep (insomnia or hypersomnia), appetite, and psychomotor activity (observed slowing or agitation); recurrent thoughts of death or suicide ('I feel there is no point,' talk of self-harm); and unexplained physical complaints (fatigue, headache, body pain without organic cause) that recur across multiple visits. In children and adolescents, depression may present atypically as irritability, school refusal, and somatic complaints rather than sadness.
For psychotic disorders (schizophrenia, brief psychotic disorder) the signals are more dramatically abnormal but are often missed because families rationalise them: hallucinations (most commonly auditory — 'hearing voices' that others cannot hear, especially derogatory or commanding voices); delusions (fixed, false, culturally incongruent beliefs — beliefs of persecution, reference, or grandeur); marked social withdrawal from family and peer groups; disorganised speech (incoherent, tangential answers) or behaviour (bizarre acts, self-neglect); and negative symptoms (flat affect, poverty of speech, loss of motivation) that families often mislabel as laziness.
For alcohol and substance use disorders: frequent intoxication, tolerance (needing more to achieve the same effect), withdrawal symptoms (tremors, sweating, seizures on stopping), neglect of responsibilities, and continued use despite obvious harm. In rural settings, country liquor consumption and solvent inhalation in adolescents may be under-reported.
For somatoform and medically unexplained disorders: recurrent, multi-system physical complaints that are fully investigated and unexplained; doctor-shopping behaviour; and marked disability disproportionate to objective findings. These patients consume disproportionate primary care resources and are rarely recognised as having a treatable mental health problem.
For developmental disorders (autism spectrum, intellectual disability, ADHD): parental concern about delayed speech, poor eye contact, repetitive behaviours, or academic difficulty are the sentinel signals. School teachers and ANMs are often the first to notice.
IMPORTANT: The community level recognition framework operationalises these signals for non-specialist workers (ASHAs, ANMs, community health volunteers) using validated, simplified tools. In India, the MHCP (Mental Health Care Package) under DMHP includes a two-question depression screen ('During the past month, have you often been bothered by feeling down, depressed, or hopeless?' and 'Have you had little interest or pleasure in doing things?') that can be administered by any trained health worker.
| Disorder Category | Key Warning Signals | At-risk Population | Action at Community Level |
|---|---|---|---|
| Depression/Anxiety | Persistent sadness >2 weeks, anhedonia, sleep/appetite change, suicidal ideation | Women of reproductive age, elderly, post-disaster survivors | Two-question screen; refer if positive |
| Psychosis | Auditory hallucinations, delusions, social withdrawal, self-neglect | Young adults (peak onset 18–35), post-partum women | Immediate referral to DMHP team; involve family |
| Alcohol use disorder | Frequent intoxication, tolerance, withdrawal, role neglect | Men 20–50, daily labourers | Brief intervention at PHC; de-addiction referral |
| Somatoform | Recurrent unexplained physical symptoms, doctor-shopping | Women 30–50, low literacy | Explain mind-body link; avoid over-investigation |
| Developmental | Delayed milestones, poor eye contact, academic difficulty | Children <10 years | Developmental screening; early intervention referral |
SELF-CHECK
A 28-year-old man is brought by his family because over the past month he has stopped going to work, spends hours alone, and has been seen 'talking to himself' in his room. He denies being unwell. Which warning signal most strongly suggests a psychotic disorder?
A. Persistent sadness lasting more than two weeks
B. Social withdrawal combined with self-referential talking (likely auditory hallucinations)
C. Refusal to see a doctor
D. Sleep disturbance
Reveal Answer
Answer: B. Social withdrawal combined with self-referential talking (likely auditory hallucinations)
Social withdrawal accompanied by apparent auditory hallucinations (talking to an unseen presence) is the hallmark warning signal for a psychotic disorder such as schizophrenia. Option A suggests depression; option C and D are non-specific. A DMHP referral is indicated.