Page 2 of 8
CM15.1-4 | CM15.1-4 | Mental Health Recognition and Programme Response — SDL Guide (Part 2)
National Mental Health Programme and Mental Healthcare Act
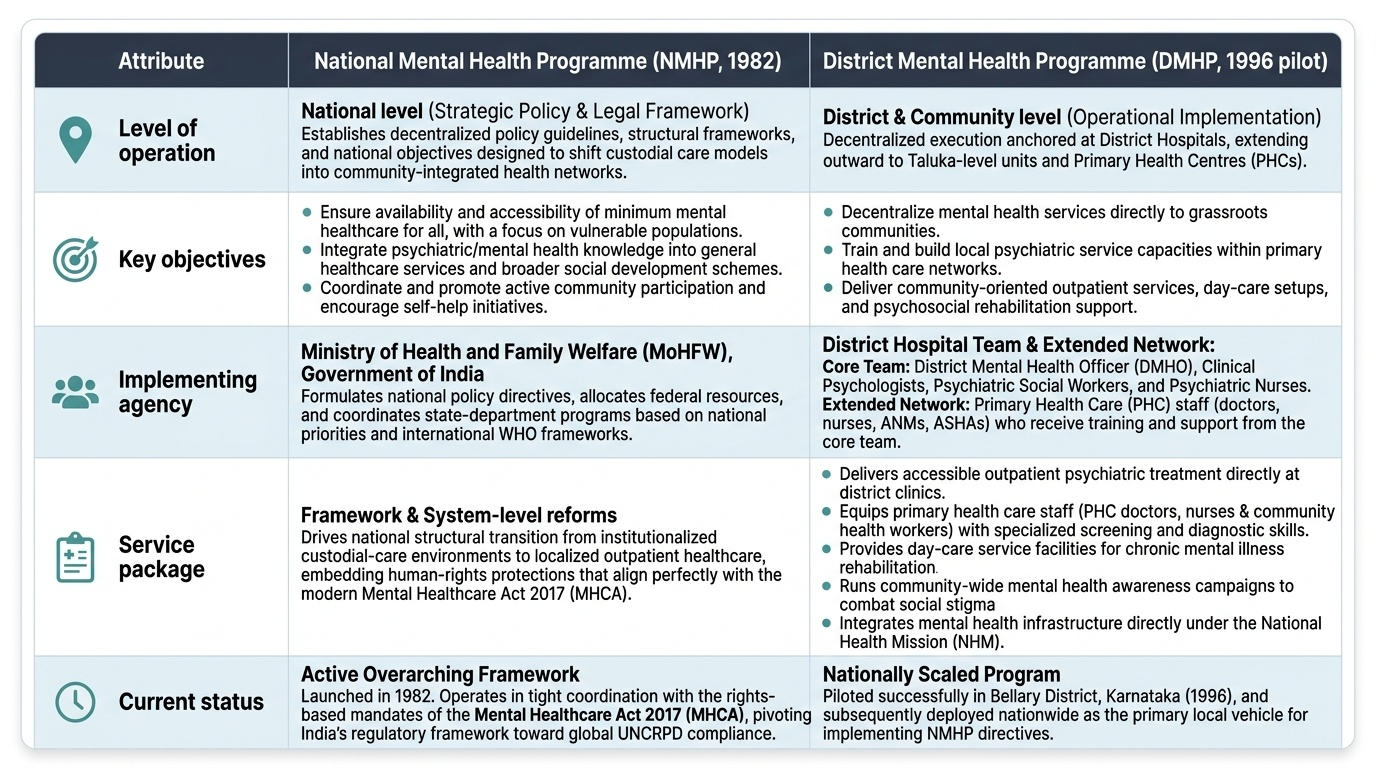
India's public mental health architecture rests on two pillars: the National Mental Health Programme (NMHP) — which provides the delivery framework — and the Mental Healthcare Act 2017 — which provides the legal framework of rights and protections.
The National Mental Health Programme (NMHP), 1982 was launched by the Government of India following the recommendations of the Ratnasabapathy Report and in alignment with WHO's Declaration of Alma-Ata (1978), which called for the integration of mental health into primary care. NMHP's four founding objectives are: (1) to ensure availability and accessibility of minimum mental healthcare for all, particularly the most vulnerable; (2) to encourage the application of mental health knowledge in general healthcare and social development; (3) to promote community participation in mental health service development; and (4) to stimulate efforts towards self-help in the community. The programme's strategic approach shifted the locus of care from large psychiatric hospitals to the community — a fundamental conceptual break with the custodial-care tradition of pre-independence psychiatry.
The District Mental Health Programme (DMHP) is the operational arm of NMHP at district level. It was piloted in Bellary district, Karnataka in 1996 and subsequently scaled nationally. Each DMHP unit is based at the District Hospital and operates outreach services to taluka and primary health centres. The DMHP service package includes: outpatient psychiatric services at district level; training of PHC doctors, nurses, ANMs, and ASHAs in basic mental health recognition and management; day-care centres for chronic mental illness; psychosocial rehabilitation; community awareness campaigns; and integration with National Health Mission (NHM) platforms. The DMHP team structure typically comprises a District Mental Health Officer (DMHO), a clinical psychologist, psychiatric social workers, and psychiatric nurses.
The Mental Healthcare Act 2017 (MHCA 2017) — which replaced the Mental Health Act 1987 — represents a landmark shift from a custody-oriented legal framework to a rights-based framework aligned with the UN Convention on the Rights of Persons with Disabilities (UNCRPD). Its key provisions for community medicine practice include:
- Right to access mental healthcare: every person has the right to affordable, high-quality mental healthcare — including at government-funded facilities.
- Right to make an advance directive: a person with mental illness can document in advance how they wish to be treated during a future episode of illness.
- Right to nominate a representative: a trusted person who can make decisions on their behalf during incapacity.
- Right to equality and non-discrimination: mental illness cannot be grounds for discrimination in employment, housing, or healthcare.
- Right to confidentiality: information about a person's mental illness cannot be disclosed without consent.
- Decriminalisation of attempted suicide (Section 115): a person who attempts suicide is presumed to be under severe stress — not criminal. They must be provided care, not prosecution. This provision has major public health significance for suicide prevention programmes.
- Prohibition of inhuman treatment: the Act explicitly prohibits electroconvulsive therapy without anaesthesia, and treatment without informed consent in non-emergency settings.
IMPORTANT: The shift from the 1987 to 2017 Act is frequently examined. The 1987 Act was modelled on the British Mental Health Act 1959 and focused on detention and management of those deemed 'dangerous'; the 2017 Act is modelled on UNCRPD and focuses on rights, autonomy, and community integration.
Provided image
SELF-CHECK
Under the Mental Healthcare Act 2017, which provision directly supports suicide prevention by changing how a person who has attempted suicide is treated by law?
A. Right to nominate a representative
B. Right to an advance directive
C. Section 115 — decriminalisation of attempted suicide
D. Right to equality and non-discrimination
Reveal Answer
Answer: C. Section 115 — decriminalisation of attempted suicide
Section 115 of MHCA 2017 decriminalises attempted suicide. It presumes the person was under severe stress and mandates that they receive care — not prosecution under the IPC. This provision is directly relevant to suicide prevention in community settings.
Monitoring and Evaluation of Mental Health Programmes
A programme without monitoring is a policy without accountability. The evaluation of NMHP/DMHP employs both process (coverage, service delivery) and outcome (morbidity, disability, suicide) indicators — all nested within India's broader national health data systems.
Key process indicators used to monitor NMHP/DMHP performance include: treatment coverage rate (proportion of identified mental disorder cases receiving appropriate treatment — the 80–85% treatment gap is both the baseline and the programme target to close); DMHP facility reach (number of districts where operational DMHP units function — as of recent NHM reports, coverage remains incomplete with significant inter-state variation); PHC doctor training coverage (proportion of PHC medical officers trained in MHCP protocols under DMHP); awareness campaign reach (communities covered by anti-stigma activities); and referral linkage rates (proportion of PHC-detected cases successfully referred to DMHP).
Key outcome indicators include: suicide rate (National Crime Records Bureau annual data — India's age-standardised suicide rate is approximately 12–14 per 100,000; states like Chhattisgarh, Telangana, Kerala show higher rates); disability-adjusted life years (DALYs) attributed to mental disorders (from GBD study data updated periodically); and quality of life measures among programme beneficiaries. The NMHS 2016 itself serves as the major baseline outcome survey — India does not yet have a real-time national mental health registry.
Programme challenges and bottlenecks that monitoring consistently reveals include: (1) Stigma — the single largest demand-side barrier; families conceal mental illness, patients refuse care, and community workers face social resistance; (2) Workforce shortage — India has approximately 0.3 psychiatrists per 100,000 population against a WHO-recommended minimum of 1–2; the DMHP task-shifting model is essential precisely because specialist numbers will not scale quickly; (3) Geographic access — one-third of districts in tribal and hilly areas lack functional DMHP units; (4) Treatment discontinuation — most NMHP beneficiaries stop treatment within 3 months due to perceived recovery, cost of transport, or medication side-effects; (5) Data quality — HMIS mental health indicators are incompletely filled in most states, making real-time programme monitoring difficult.
The Eleventh and Twelfth Five-Year Plans substantially increased NMHP allocation, and recent NHM annual implementation plans have integrated mental health as a non-communicable disease priority — signalling a policy-level commitment to scale. Evaluation frameworks now align with WHO's Comprehensive Mental Health Action Plan 2013–2030 indicators, which set global benchmarks for treatment coverage, human rights protection, and community integration.
CLINICAL PEARL
The 'two-question depression screen' validated for low-resource primary care settings — 'Over the past two weeks, have you felt down, depressed, or hopeless?' and 'Have you had little interest or pleasure in doing things?' — has a sensitivity of approximately 83% and specificity of 92% for major depression when both questions are positive (Whooley et al.). This screen can be administered by a trained ANM in under one minute and does not require a psychiatric specialist. Under DMHP protocol, a single positive response to either question is sufficient to trigger a brief structured assessment. In Rupa's case (our opening scenario), both questions would be answered affirmatively — making her a clear referral candidate regardless of the grief context.
SELF-CHECK
The NMHS 2016 reported a treatment gap of approximately 80–85% for most mental disorders in India. Which combination of factors BEST explains this gap?
A. Low prevalence of mental disorders and limited awareness among patients
B. Stigma, workforce shortage, geographic access barriers, and high out-of-pocket cost
C. Absence of a national mental health programme before 2017
D. Over-reliance on AYUSH practitioners and self-medication with traditional remedies
Reveal Answer
Answer: B. Stigma, workforce shortage, geographic access barriers, and high out-of-pocket cost
The treatment gap is multi-causal: stigma prevents help-seeking, a specialist workforce of only ~0.3 psychiatrists/100,000 limits supply, geographic inaccessibility excludes rural populations, and high out-of-pocket expenditure deters follow-up. NMHP was launched in 1982 (not 2017), so option C is factually incorrect.
Application: Recognition and Referral in Community Practice
The preceding sections provide the epidemiological, clinical, and programme knowledge required for community mental health practice. This section synthesises them into a practical recognition-and-referral framework for doctors working at PHC and Community Health Centre level — the frontline of NMHP delivery.
Step 1 — Opportunistic and systematic screening. At every PHC consultation, routine screening for mental health problems should be embedded as part of the clinical encounter. The two-question depression screen (described in the Clinical Pearl) takes under 60 seconds. For patients with chronic physical illness (diabetes, hypertension, epilepsy) the screening should be systematic because comorbid mental disorders in this population are common and dramatically worsen physical health outcomes. ASHA workers and ANMs conducting home visits should be trained to identify the warning signals described earlier and to report them during routine supervisory contacts.
Step 2 — Risk stratification. Once a warning signal is identified, rapid severity triage guides the urgency and pathway of the response:
- Mild: common mental disorder symptoms present but the person is functional, no suicidal ideation, insight preserved → brief counselling and psychoeducation at PHC level, review in two weeks.
- Moderate: significant functional impairment, possible substance use, some safety concern → DMHP outreach team involvement, PHC doctor initiates first-line pharmacotherapy (e.g. antidepressant for moderate depression) per NMHP protocol.
- Severe: active psychosis, suicidal intent with plan, severe self-neglect, or agitation endangering self or others → immediate referral to District Hospital psychiatry unit; family or nominated representative engaged; MHCA 2017 rights explained.
Step 3 — Communication that reduces stigma. How the doctor communicates about a mental health diagnosis determines whether the patient accepts referral and treatment. Evidence-based stigma-reduction principles in community settings include: using non-pejorative language ('you are experiencing a medical condition affecting your mood/thoughts' rather than 'you are pagal'); normalising the experience ('this is very common — one in ten people experience depression at some point'); engaging the family as partners rather than adversaries; and explicitly addressing the MHCA 2017 rights to confidentiality and dignity.
Step 4 — Referral and follow-up. A referral without follow-up is a referral lost. Community health workers should be tasked with follow-up visits within 2–4 weeks to check adherence to treatment, transportation barriers, and family support. This task-shifting model is central to DMHP's theory of change — the specialist psychiatrist at the district hospital manages complex cases and trains the PHC team; the PHC team manages common cases and monitors referred cases in the community.
Worked scenario: Returning to Rupa. The PHC doctor applies the two-question screen (both positive). She identifies: warning signals (persistent sadness >3 weeks, refusal to eat, suicidal ideation implied by 'no point in living', possible auditory hallucinations to be assessed). She categorises severity as MODERATE-SEVERE (functional impairment + safety concern). She contacts the district DMHP team, initiates psychoeducation with Rupa's husband, explains the MHCA 2017 right to confidentiality, and arranges transport to the DMHP outreach clinic the following morning. The ASHA worker is asked to visit daily and report back. Rupa's case demonstrates that appropriate care begins at the village level — not at the psychiatry ward.
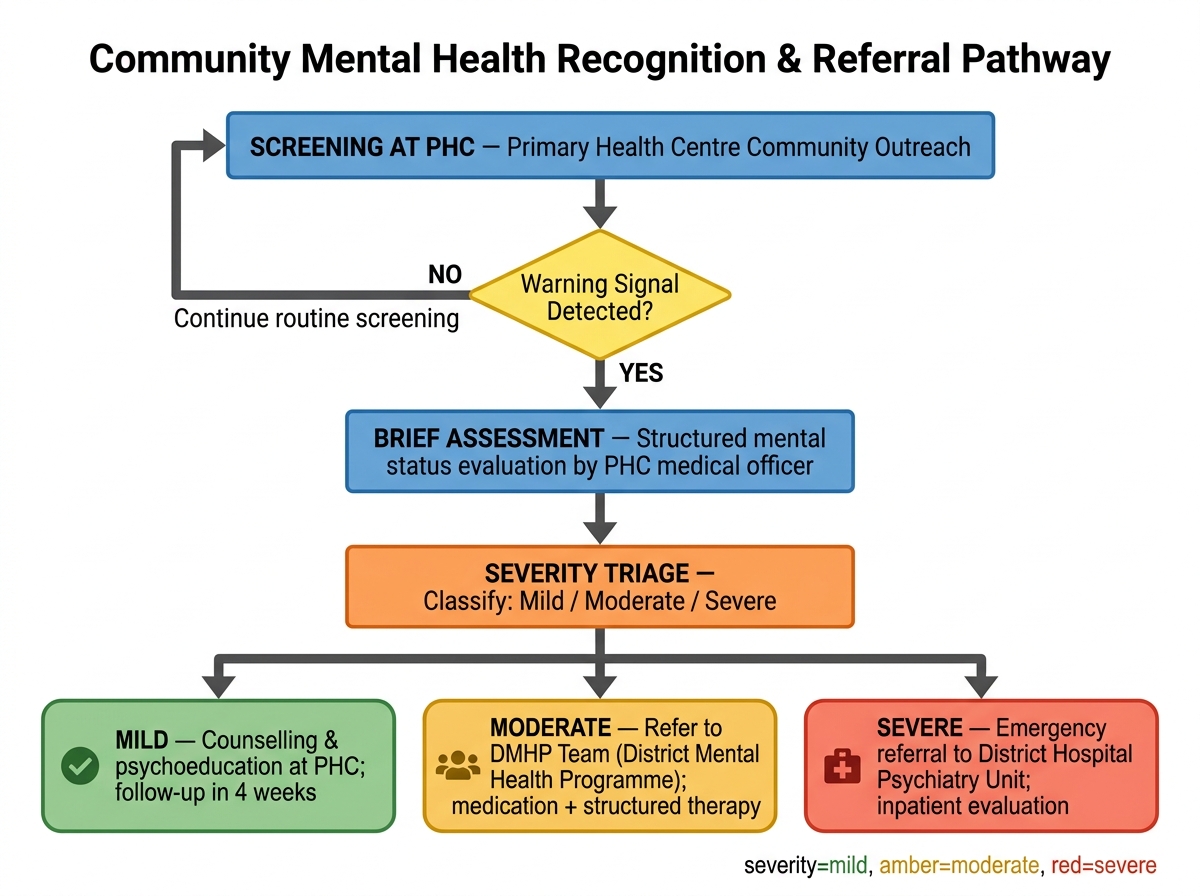
Community Mental Health Recognition and Referral Pathway (NMHP/DMHP Framework)