Page 1 of 32
CM5.{1,14-15} | CM5.{1,14-15} | Nutrients, Requirements and Personal Nutrition — SDL Guide
Learning Objectives
- Describe the common sources of major macronutrients and micronutrients and their functions
- State the ICMR-NIN 2020 Recommended Dietary Allowances for key nutrients across life stages
- Explain how age, sex, physiological state, and activity level modify nutritional requirements
- Articulate the role of personal nutrition awareness and counselling in health promotion and disease prevention
INSTRUCTIONS
Nutrition sits at the foundation of all clinical medicine. A doctor who cannot translate nutrient requirements into practical dietary advice leaves a critical gap in preventive care. This module builds the vocabulary and reference values you will use throughout your career — from prescribing a diet for a pregnant woman to counselling a patient with metabolic disease.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 11 — Nutrition and Health (textbook)
- ICMR-NIN 2020 — Recommended Dietary Allowances and Estimated Average Requirements for Indians (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a Family Welfare Centre in rural Rajasthan, a 22-year-old primigravida in her third trimester is found pale and fatigued. Her haemoglobin is 8.2 g/dL. She reports eating only chapati, dal, and sometimes vegetables. 'I eat what the family eats,' she says. Her diet, though seemingly ordinary, is deficient in iron, folate, and calcium — nutrients with heightened demands in pregnancy that a standard adult diet often fails to meet. This encounter is not unusual. It is, in fact, representative of India's double burden of malnutrition: undernutrition (particularly micronutrient deficiencies) in rural women and children, coexisting with rising overnutrition (obesity, metabolic syndrome) in urban settings. As a doctor, knowing precisely which nutrients are needed, in what amounts, and for whom is not an academic exercise — it is the first clinical skill in nutrition.
WHY THIS MATTERS
Nutritional knowledge is directly actionable in clinical practice. Every patient interaction involving diet — antenatal counselling, growth monitoring in children, management of anaemia, or advice to a diabetic — requires you to translate nutrient science into food guidance. India's National Family Health Survey (NFHS-5, 2019-21) reports that 57% of women aged 15-49 are anaemic, 35.5% of children under 5 are stunted, yet 24% of adults are overweight or obese. These numbers make nutrition not just a public health statistic but a daily clinical reality. The ICMR-NIN 2020 Recommended Dietary Allowances (RDA) provide India-specific reference values — derived from Indian population data — that supersede older global estimates. This module gives you the framework and the numbers.
RECALL
Before proceeding, recall from your Biochemistry (BI) coursework: carbohydrates, proteins, and fats are metabolised to yield ATP via glycolysis, the TCA cycle, and beta-oxidation respectively. The digestive system (Physiology, PY) absorbs nutrients in specific segments — iron in the duodenum and jejunum, B12 in the terminal ileum, fat-soluble vitamins with dietary fat. Basal metabolic rate (BMR) — the energy expended at rest — is the foundation on which total daily energy requirements are built, modified by an activity factor. These biochemical and physiological concepts anchor the practical RDA values you will learn here.
The Scale of Nutritional Deficiency in India
India bears one of the world's highest burdens of nutritional deficiency, and understanding this magnitude is the first step toward meaningful public health action. The double burden of malnutrition — undernutrition and overnutrition coexisting in the same country and sometimes in the same household — defines India's nutritional landscape. NFHS-5 (2019-21) reports 35.5% stunting and 19.3% wasting in children under five, alongside 23.4% overweight or obesity in adult women. Among women aged 15-49, anaemia prevalence is 57%. These figures are not merely statistics; they translate into lost cognitive development in children, increased maternal and neonatal mortality, and rising non-communicable disease burden in adults.
The nutritional transition — a shift from traditional high-fibre diets to processed, high-energy-density foods — is accelerating among urban populations, even as rural populations struggle with micronutrient deficiencies. Vitamin A deficiency, iodine deficiency disorders, and iron deficiency anaemia together constitute the 'hidden hunger' — deficiencies that impair health without obvious hunger. Zinc deficiency, affecting an estimated 25% of Indians, contributes to impaired immune function and growth faltering. This epidemiological context explains why India's National Nutrition Policy, POSHAN Abhiyaan 2018-22, and flagship programmes such as ICDS and the Mid-Day Meal Scheme are designed precisely to address these gaps at scale.
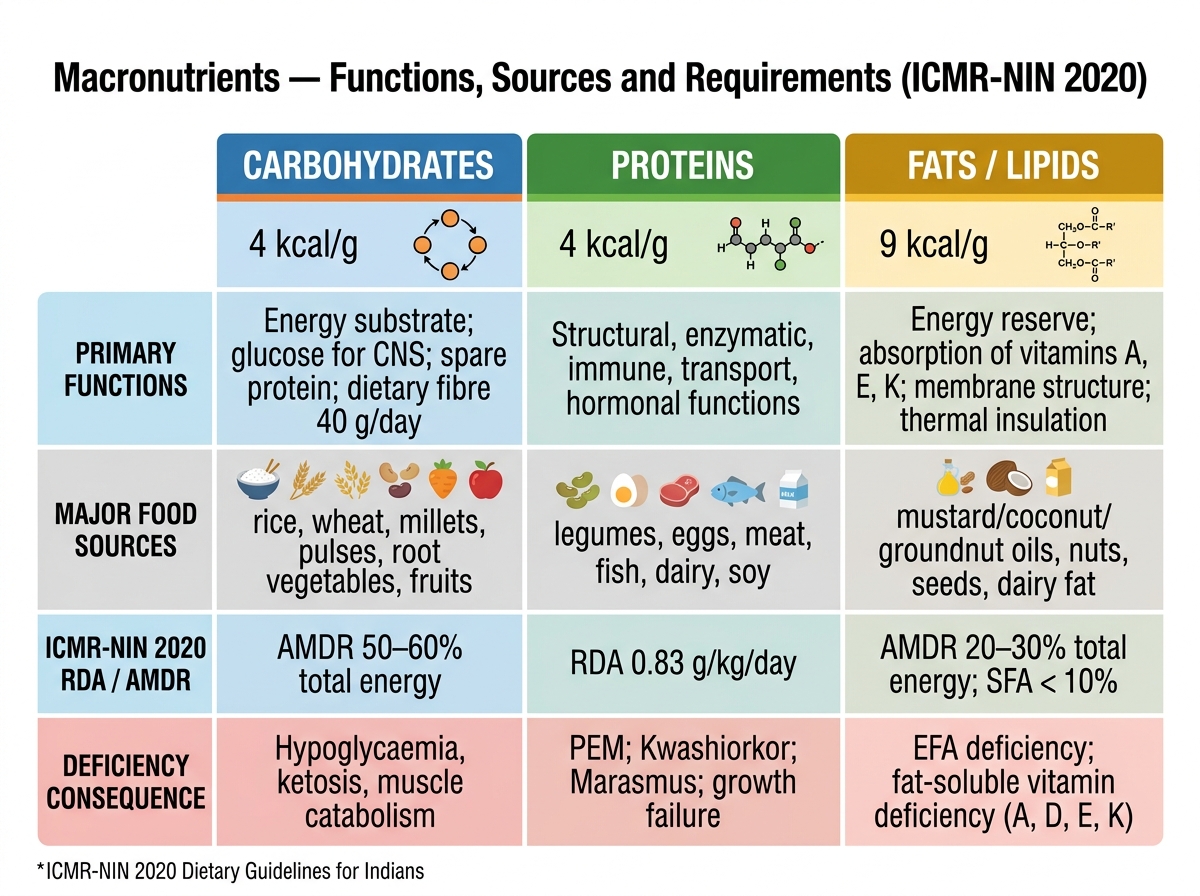
Macronutrients — Functions, Sources and Requirements (ICMR-NIN 2020)
Macronutrients — Functions, Sources and Requirements
Provided image
Macronutrients are the energy-yielding nutrients consumed in gram quantities daily. Understanding them requires knowing not just their functions but their caloric density, principal food sources, and the ICMR-NIN 2020 reference values that quantify how much is enough for an Indian adult.
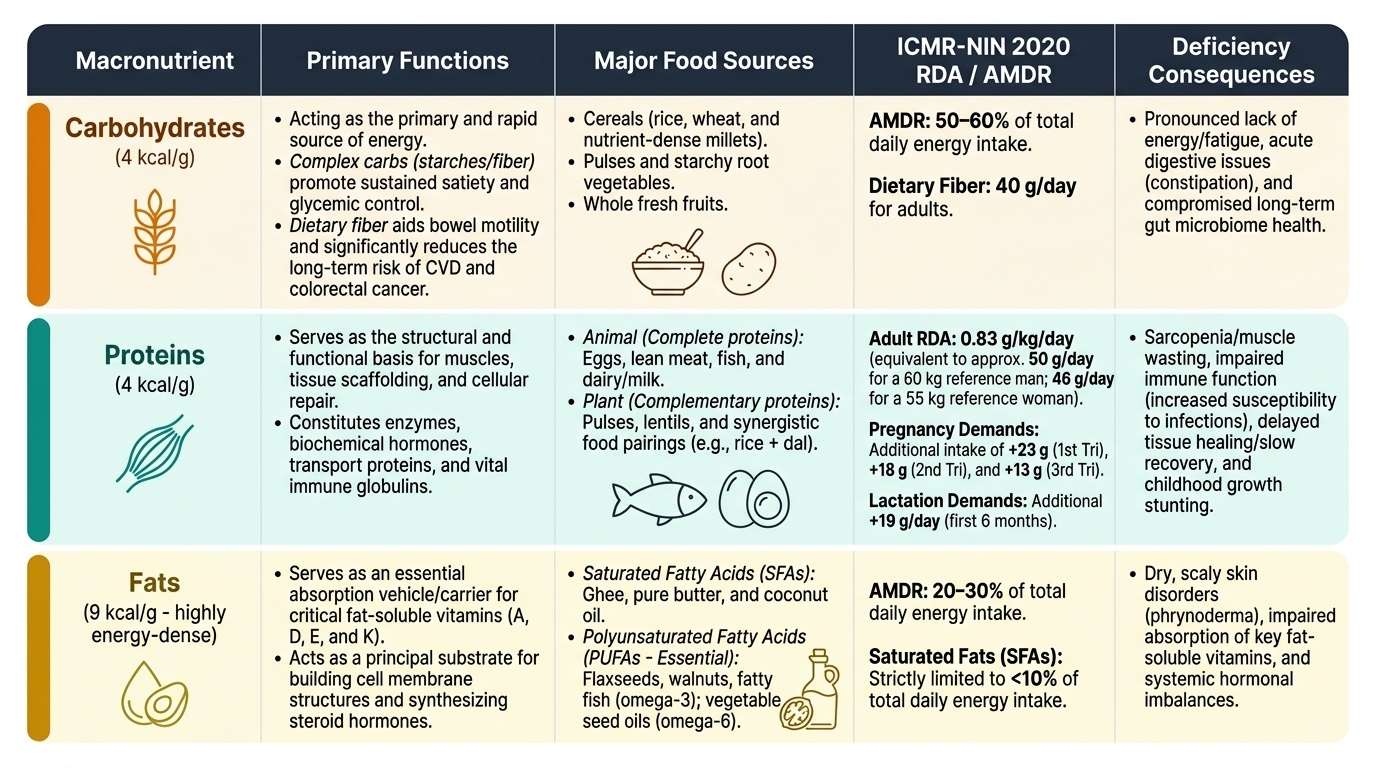
Carbohydrates provide 4 kcal per gram and should supply 50-60% of total daily energy (ICMR-NIN 2020 Acceptable Macronutrient Distribution Range, AMDR). Principal sources are cereals (rice, wheat, millets), pulses, root vegetables, and fruits. Simple carbohydrates (sugars) are rapidly absorbed and promote postprandial glycaemic spikes; complex carbohydrates (starches, dietary fibre) promote satiety and glycaemic control. Dietary fibre — the non-digestible polysaccharide fraction — has a recommended intake of 40 g/day for an adult Indian; it reduces constipation, colorectal cancer risk, and cardiovascular disease risk.
Proteins yield 4 kcal per gram and are the structural and functional molecules of the body — enzymes, hormones, immune globulins, transport proteins, and tissue scaffolding. The ICMR-NIN 2020 RDA for protein is 0.83 g/kg body weight/day for a sedentary adult (reference man 60 kg = 50 g/day; reference woman 55 kg = 46 g/day). Biological value of protein depends on its essential amino acid profile: animal proteins (eggs, meat, fish, milk) are complete; most plant proteins are limiting in one or more essential amino acids, but complementary combinations (e.g. rice + dal) achieve adequacy. During pregnancy, extra protein of 23 g/day (first trimester), 18 g/day (second trimester), and 13 g/day (third trimester) is recommended. Lactation requires an additional 19 g/day in the first six months.
Fats yield 9 kcal per gram — the most energy-dense macronutrient — and serve as carrier of fat-soluble vitamins (A, D, E, K), substrate for steroid hormone synthesis, and structural component of cell membranes. The ICMR-NIN AMDR for fat is 20-30% of total energy. Saturated fatty acids (SFAs) — present in ghee, butter, coconut oil — should be limited to <10% of energy; polyunsaturated fatty acids (PUFAs), including omega-3 (α-linolenic acid from flaxseed, walnuts, fatty fish) and omega-6 (linoleic acid from vegetable oils), are essential fatty acids that must be obtained from diet. Trans fatty acids, formed during partial hydrogenation of vegetable oils (present in vanaspati, bakery products), are strongly atherogenic and should be <1% of energy.
Energy requirements for the ICMR-NIN 2020 reference adult (sedentary): man ~2110 kcal/day; woman ~1660 kcal/day. These values increase with moderate activity (man ~2710 kcal; woman ~2130 kcal) and heavy activity (man ~3470 kcal; woman ~2720 kcal).
SELF-CHECK
An adult Indian woman (55 kg, sedentary) is planning a vegetarian diet. What is her recommended dietary protein intake per day according to ICMR-NIN 2020?
A. 35 g/day
B. 46 g/day
C. 60 g/day
D. 75 g/day
Reveal Answer
Answer: B. 46 g/day
ICMR-NIN 2020 protein RDA is 0.83 g/kg/day. For a 55 kg reference woman: 0.83 × 55 = 45.65 ≈ 46 g/day. Protein quality (biological value of plant proteins) is a separate consideration addressed by complementary food combinations.
Micronutrients — Vitamins and Minerals
Micronutrients are vitamins and minerals required in small quantities (milligrams or micrograms) but are indispensable for normal metabolism, immune function, and development. Deficiency produces specific clinical syndromes that are prevalent in India and directly testable in NMC examinations.
Fat-soluble vitamins (A, D, E, K) are absorbed with dietary fat and stored in the body, making both deficiency and toxicity possible:
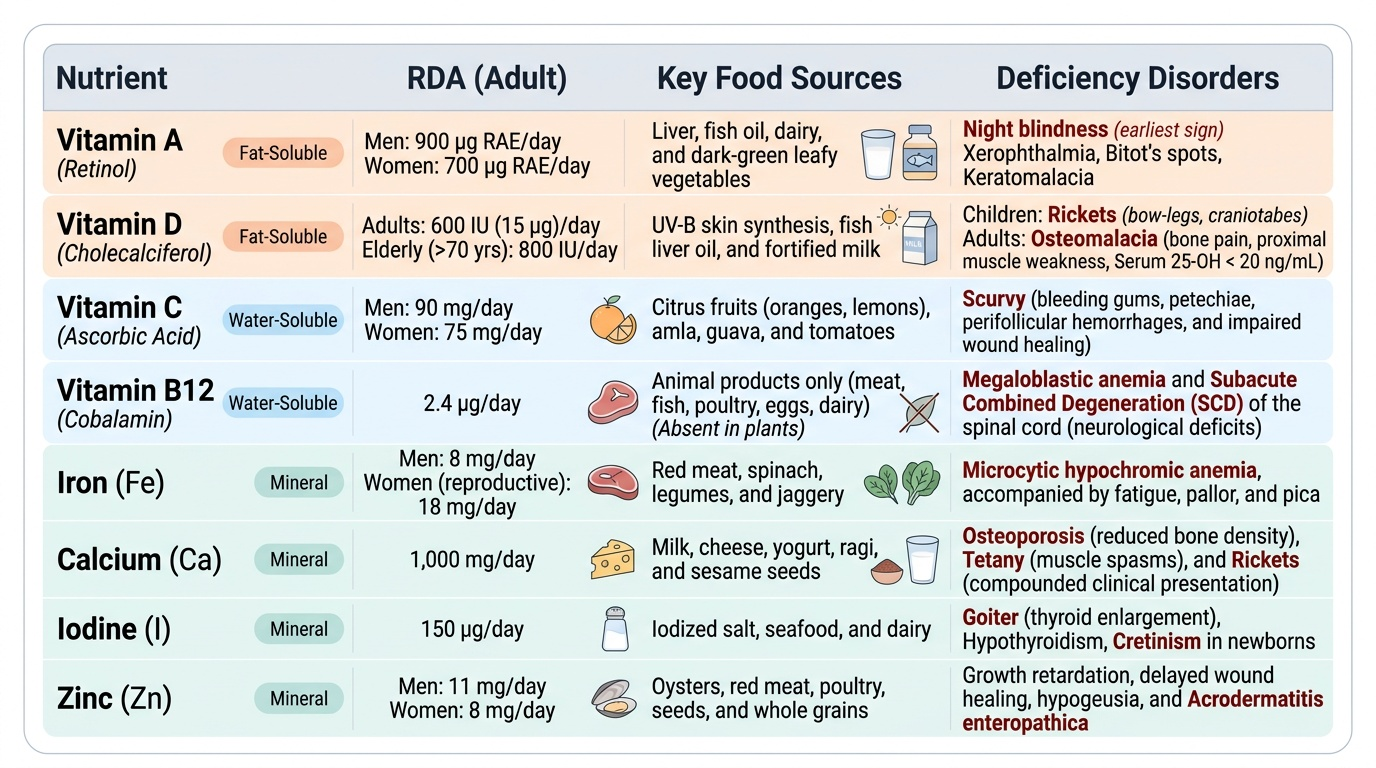
- Vitamin A (retinol): RDA adult man 900 µg Retinol Activity Equivalents (RAE)/day, adult woman 700 µg RAE/day. Sources: liver, fish oil, dairy, dark-green leafy vegetables (as β-carotene, converted at 1/12 efficiency). Deficiency → night blindness (earliest sign), xerophthalmia, Bitot's spots, keratomalacia, and increased susceptibility to infections. Vitamin A supplementation reduces under-5 mortality in deficient populations.
- Vitamin D (cholecalciferol): Synthesised in skin on UV-B exposure; dietary sources are fish liver oil, fortified milk. RDA adult 600 IU (15 µg)/day; elderly (>70 yrs) 800 IU/day. Deficiency → rickets in children (bow-legs, craniotabes), osteomalacia in adults (bone pain, proximal muscle weakness). Serum 25-OH vitamin D <20 ng/mL = deficiency. High prevalence in India despite sunny climate, due to low dietary intake and limited sun exposure in women.
- Vitamin K: Essential for synthesis of clotting factors II, VII, IX, X (the 'K-vitamin clotting factors'). RDA adult 55-65 µg/day. Deficiency → haemorrhagic disease of the newborn (breastfed neonates — breast milk low in Vitamin K).
Water-soluble vitamins (B-complex, Vitamin C) are not stored appreciably, so regular dietary intake is essential:
- Vitamin B12 (cobalamin): RDA adult 2.2 µg/day. Exclusively in animal foods; vegans are at high risk. Deficiency → megaloblastic anaemia + subacute combined degeneration of the spinal cord (demyelination of dorsal and lateral columns). Intrinsic factor (IF) required for ileal absorption — IF deficiency causes pernicious anaemia.
- Folate (Vitamin B9): RDA adult 220 µg/day; pregnancy 500 µg/day. Deficiency → megaloblastic anaemia; neural tube defects (NTDs) in early pregnancy — folate supplementation pre-conception and in first trimester prevents NTDs.
- Vitamin C (ascorbic acid): RDA adult 80 mg/day. Deficiency → scurvy (perifollicular haemorrhages, bleeding gums, corkscrew hairs, impaired wound healing). Enhances non-haem iron absorption — important in vegetarian diets.
Key minerals:
- Iron: RDA adult man 19 mg/day, adult woman 29 mg/day (non-pregnant); pregnancy 35 mg/day (ICMR-NIN 2020). Deficiency → iron deficiency anaemia — the most prevalent micronutrient deficiency in India; affects 57% of women aged 15-49 (NFHS-5). Haem iron (meat, fish) is absorbed at ~25%; non-haem iron (cereals, pulses) at ~5-10%; absorption enhanced by Vitamin C, inhibited by phytates and tannins.
- Calcium: RDA adult 1000 mg/day; pregnancy and lactation 1200 mg/day. Sources: milk and milk products, ragi (finger millet), sesame seeds, dark-green leafy vegetables. Deficiency → rickets (children), osteomalacia (adults), osteoporosis (long-term). Vitamin D is required for calcium absorption.
- Iodine: RDA adult 150 µg/day; pregnancy 220 µg/day; lactation 290 µg/day. Deficiency → iodine deficiency disorders (IDD): goitre, cretinism (hypothyroidism in infancy — intellectual disability, growth retardation). Universal salt iodisation (USI) is India's primary control strategy. Sources: iodised salt, seafood.
- Zinc: RDA adult man 17 mg/day, adult woman 12 mg/day. Deficiency → growth retardation, impaired immune function, hypogonadism, impaired wound healing, acrodermatitis enteropathica. Present in meat, legumes, whole grains (but phytates reduce bioavailability in plant sources).
Provided image
SELF-CHECK
A 2-year-old child in rural Odisha presents with bow-legs and widened wrist epiphyses on X-ray. Serum calcium is 8.0 mg/dL. Which nutrient deficiency best explains this presentation?
A. Iron deficiency
B. Vitamin A deficiency
C. Vitamin D deficiency
D. Iodine deficiency
Reveal Answer
Answer: C. Vitamin D deficiency
The triad of bow-legs, widened epiphyses (rachitic rosary, cupped metaphyses on X-ray), and low-normal calcium in a child is diagnostic of nutritional rickets due to Vitamin D deficiency. Vitamin D is required for intestinal calcium absorption and bone mineralisation. Note: Vitamin A deficiency causes night blindness and xerophthalmia, not rickets.