Page 2 of 32
CM5.{1,14-15} | CM5.{1,14-15} | Nutrients, Requirements and Personal Nutrition — SDL Guide (Part 2)
Special Nutritional Requirements Across the Life Cycle
Nutritional requirements are not fixed — they change substantially across the life cycle and with physiological state. Understanding these variations is essential for counselling individual patients and for designing population-level nutrition programmes. The ICMR-NIN 2020 provides group-specific RDA values that replace one-size-fits-all guidance.
Infancy (0-6 months): Exclusive breastfeeding (EBF) meets all nutritional requirements for the first 6 months. Breast milk provides ~70 kcal/100 mL, adequate protein (~1.1 g/100 mL), essential fatty acids (DHA/ARA), immunoglobulins (especially secretory IgA), and bioavailable iron and zinc. After 6 months, complementary foods are introduced (see CM5.13 module). Vitamin D supplementation (400 IU/day) is recommended for exclusively breastfed infants in settings with limited sun exposure.
Childhood (1-10 years): Rapid growth demands high protein intake relative to body weight (~1.0-1.2 g/kg/day for children vs 0.83 g/kg for adults). Iron, calcium, and zinc requirements per kg body weight are higher than in adults. School-age children benefit from midday meals for both nutrition and attendance (National Mid-Day Meal Scheme/PM POSHAN).
Adolescence: The adolescent growth spurt increases energy, protein, iron (especially in girls with onset of menstruation), and calcium requirements substantially. Girls: iron RDA 27 mg/day during adolescence. Peak bone mass is acquired primarily during adolescence — adequate calcium and Vitamin D at this stage reduces osteoporosis risk decades later. Weekly Iron and Folic Acid Supplementation (WIFS) under NIPI/RBSK targets adolescent girls to address this.
Pregnancy: Energy requirement increases by approximately 350 kcal/day in the second trimester and 450 kcal/day in the third trimester. Extra protein: 23 g/day (T1), 18 g/day (T2), 13 g/day (T3) above baseline RDA. Iron requirement rises to 35 mg/day, folate to 500 µg/day, iodine to 220 µg/day, calcium to 1200 mg/day. The government IFA (Iron-Folic Acid) supplementation programme targets all pregnant women to meet iron and folate needs.
Lactation: Energy demand increases by ~530 kcal/day in the first 6 months (some met from gestational fat stores). Extra protein 19 g/day (months 0-6), 13 g/day (months 7-12). Calcium requirement remains elevated at 1200 mg/day to support milk calcium content without maternal bone demineralisation. Iodine requirement peaks at 290 µg/day.
Elderly: BMR declines with age (~2% per decade after 40), reducing total energy needs, but protein requirements remain at 0.83 g/kg/day or higher to prevent sarcopenia. Calcium requirement rises to 1200 mg/day (age >50) due to reduced absorption efficiency. Vitamin D requirement increases to 800 IU/day (age >70). Micronutrient-dense foods and fortified products are preferred over energy-dense but nutrient-poor foods.
Activity level modifies energy requirements linearly via the Physical Activity Ratio (PAR). A man doing heavy physical labour (PAR ~4.0) may require 3470 kcal/day vs 2110 kcal/day for a sedentary man — a 65% increase.
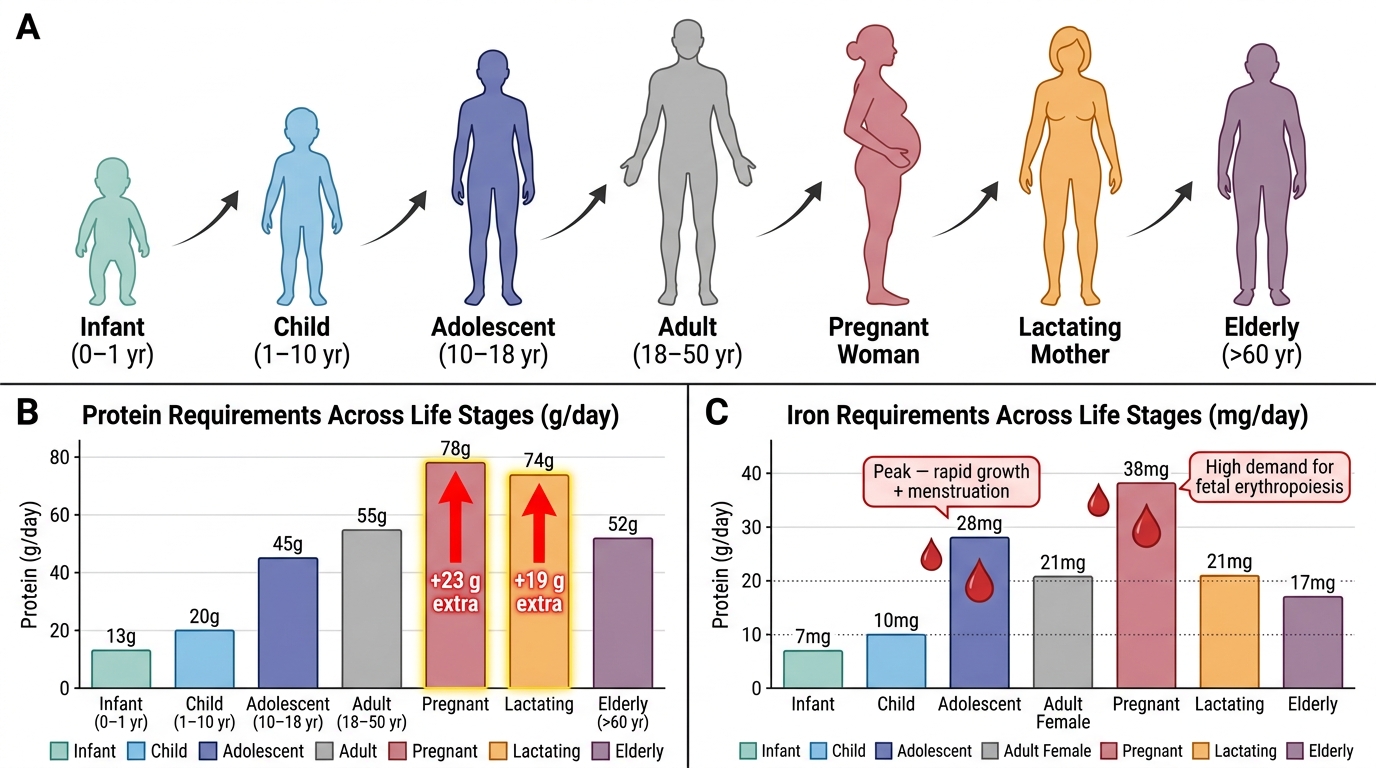
Nutrient Requirement Variations Across the Life Cycle: Protein and Iron
Nutrition Programmes and Policies as Intervention
India has developed a comprehensive framework of national programmes to address the nutritional needs identified above. These programmes are the organised societal response to the burden of malnutrition — they convert knowledge of nutritional requirements into population-level interventions. As a community medicine physician, you will work within and refer patients to these programmes.
The Integrated Child Development Services (ICDS) scheme, launched in 1975, is the world's largest nutrition programme. It delivers a supplementary nutrition package (providing 500 kcal and 12-15 g protein/day for children 6 months-6 years, and 600 kcal + 18-20 g protein for pregnant/lactating women) through Anganwadi Centres (AWCs). The scheme also integrates immunisation, health check-ups, referral services, and pre-school education — making it a convergent platform for the first 1000 days of a child's life.
The National Mid-Day Meal Scheme (now PM POSHAN) targets children in government schools. It provides a cooked meal delivering 450 kcal and 12 g protein (primary classes) or 700 kcal and 20 g protein (upper primary classes), addressing both nutritional needs and school attendance in one intervention.
POSHAN Abhiyaan (National Nutrition Mission, 2018-2022) set ambitious targets: reduce stunting, wasting, anaemia, and low birth weight by 2% per year. It uses a convergence approach across ICDS, health, WASH (water, sanitation, hygiene), and agriculture sectors, supported by a real-time monitoring app (POSHAN Tracker/Annapoorna).
National Iodine Deficiency Disorders Control Programme (NIDDCP) implements Universal Salt Iodisation (USI) — mandating that all edible salt sold in India be iodised to 15 ppm iodine at the consumer level. This has substantially reduced goitre prevalence from 54% (1980s) to <5% currently in most districts.
Understanding these programmes is not merely academic: you will be asked in OSCE settings to counsel a mother about where to access supplementary nutrition, or to explain why an adolescent girl should take WIFS tablets.
Evaluating Dietary Adequacy — Practical Tools
Before advising patients on diet, a clinician needs to evaluate the current dietary pattern. Several practical tools exist for this purpose, each with specific use cases in both clinical and community settings.
The 24-hour dietary recall is the most commonly used method in both clinical practice and nutrition surveys. The patient recalls all food and drink consumed in the previous 24 hours, with portion sizes estimated using standard measures (cups, katoris, tablespoons) or food models. Multiple recalls (2-3 non-consecutive days including one weekend day) improve accuracy and capture day-to-day variation. It is quick, requires no literacy, and can be administered by a trained health worker. Limitation: relies on memory and may underestimate portion sizes.
The dietary diversity score uses the number of distinct food groups consumed in the past 24 hours as a proxy for micronutrient adequacy. WHO's Minimum Dietary Diversity for Women (MDD-W) uses 10 food groups; a score ≥5 groups predicts micronutrient adequacy in women of reproductive age. For infant and young child feeding (IYCF), the indicator uses 8 food groups (minimum dietary diversity = 5 or more groups). This is used in NFHS surveys and by Anganwadi workers in community monitoring.
The food frequency questionnaire (FFQ) captures habitual food intake over weeks to months, quantifying how often specific foods are eaten. It is more suitable for epidemiological research than individual clinical assessment.
Food groups model: The ICMR-NIN 'My Plate for the Day' (based on 15 food groups) visualises a balanced diet. Five major food groups — cereals and millets, pulses and legumes, dairy, fruits and vegetables, and oils/fats — form the framework for dietary guidance. Each group contributes specific nutrients; diversity within and across groups ensures micronutrient adequacy.
For a clinician in a primary care setting, a simple three-question dietary screen ('Do you eat cereals + dal daily? Do you eat vegetables daily? Do you eat meat/egg/milk weekly?') combined with a focused physical examination (pallor for anaemia, thyroid size for iodine status, growth parameters for children) provides an efficient nutritional surveillance approach.