Page 16 of 27
CM10.6-7 | CM10.6-7 | Family Planning and Family Welfare Programme — SDL Guide
Learning Objectives
- Enumerate and describe various family planning methods, their mechanisms, advantages, and shortcomings
- Describe the basis, principles, and organisation of the Family Welfare Programme including technical and operational aspects
INSTRUCTIONS
India's family welfare programme has achieved a historic milestone: for the first time, the national Total Fertility Rate has reached 2.0 (NFHS-5, 2019-21), at or below the replacement level of 2.1. Yet this national average masks extreme intra-state variation — in Uttar Pradesh and Bihar TFR remains above 3, while 9.4% of currently married Indian women have an unmet need for family planning. As a community medicine practitioner and PHC medical officer, you will counsel couples on contraceptive choice, insert PPIUCDs, manage injectable contraception programmes, and track programme indicators — this module prepares you for every aspect of that responsibility.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch 12 (Population and Family Welfare) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman with two children (the younger one 4 months old, exclusively breastfed) attends the PHC asking for contraception. Her husband prefers that she does not use any 'hormonal method.' She is amenorrhoeic. She wants to space her next pregnancy by at least 3 years. The ANM knows that PPIUCD is available and that the Antara injectable programme is running. But the woman's older IUCD was expelled once, so she is hesitant about an IUD. As the PHC doctor, how do you counsel her — and which method would you recommend given her specific situation, considering effectiveness, her husband's preference, her breastfeeding status, and her previous IUCD experience?
WHY THIS MATTERS
Family planning is simultaneously an individual clinical act (counselling a couple, inserting an IUCD, prescribing emergency contraception) and a population-level public health programme (tracking mCPR, analysing unmet need, managing method mix, implementing Antara and Mission Parivar Vikas). As a community medicine physician you inhabit both roles. The clinical skills are inseparable from the programme logic — knowing why India's mCPR is 56.5% and what unmet need means is not trivia; it explains who is not coming to your counselling sessions and why.
RECALL
From your demography module, recall that Total Fertility Rate (TFR) is the average number of children a woman would have if she lived through her reproductive life and experienced the current age-specific fertility rates; the replacement level TFR of 2.1 accounts for mortality and slight male excess at birth. Recall the demographic transition model: as mortality falls first and fertility falls later, populations experience a phase of rapid growth. Recall from the RMNCH module (CM10.4) that PPIUCD is inserted within 48 hours of delivery, and from the pharmacology module that levonorgestrel is a synthetic progestogen used in emergency contraception and the LNG-IUS. The concept of WHO Medical Eligibility Criteria (WHO MEC) — classifying contraindications to each method as Category 1 (no restriction), 2 (advantages outweigh risks), 3 (risks generally outweigh advantages), 4 (absolute contraindication) — is the framework for contraindication counselling.
Population and Fertility Burden: Why Family Planning Matters
India's population policy has undergone a fundamental shift: the goal is no longer reducing fertility by targets (the coercive target-based approach was officially abandoned in 1996) but by ensuring universal access to voluntary, high-quality family planning services so that every couple can achieve their desired family size. The demographic rationale rests on two observations. First, India's TFR has reached 2.0 nationally (NFHS-5, 2019-21) — just at or below the replacement level of 2.1 — but this national average conceals extreme regional variation: Kerala (1.8) and Tamil Nadu (1.8) are already below replacement, while Uttar Pradesh (2.35) and Bihar (2.98) remain well above it. This variation drives the geographic concentration of India's unmet need. Second, unmet need — defined as the proportion of currently married women who want no more children or wish to space their next child but are not using any contraceptive method — stands at 9.4% nationally (NFHS-5), representing tens of millions of women whose reproductive intentions are not being met by the health system. The public health burden of this unmet need is measured in unwanted pregnancies, unsafe abortions (India's Abortion Assessment Report estimates 15 million abortions annually, of which a substantial proportion are clandestine), and maternal deaths from complications of unsafe abortion. The Total Fertility Rate is the composite programme outcome indicator — a falling TFR indicates that the programme is successfully helping couples achieve their intended family size. However, TFR should always be disaggregated by state and socioeconomic group to identify which populations are still not being reached.
Determinants of Contraceptive Use and Unmet Need
High unmet need persists despite programmatic availability for reasons that sit squarely at the intersection of individual, household, and community determinants. The NFHS-5 data on reasons for non-use of contraception reveal that the leading reasons are not lack of access but fear of side effects (cited by 17.3% of women with unmet need), infrequent sex (16.1%), and opposition from husband (5.1%). This reframes the programme challenge: the barrier is not primarily availability of methods but awareness of options, trust in provider counselling, and gender dynamics within households. Son preference drives demand for more children even when a couple has reached their stated desired family size, because they have not yet had a son — India's sex ratio at birth (NFHS-5: 929 girls per 1,000 boys) reflects sex-selective practices embedded in this preference. Side effect experiences (particularly with hormonal methods and IUCDs) are frequently amplified by community rumour without accurate clinical context — a woman who develops menstrual irregularity after starting Depo-Provera (an expected pharmacological effect) may discontinue and spread negative reports, dropping a method that is otherwise highly effective. Method choice: the overwhelming dominance of female sterilization in India's method mix (37.9% mCPR, NFHS-5) compared to reversible methods (condom 9.5%, OCP 4.5%, IUCD 2.1%) reflects a historical programme emphasis on sterilization acceptance that shaped client expectations — many women only know sterilization as 'the family planning option.' Reversing this method-mix distortion requires genuine counselling that presents the full basket of choices without implicit sterilization pressure.
SELF-CHECK
A 24-year-old woman exclusively breastfeeds her 4-month-old infant and has remained amenorrhoeic since delivery. She does not want another pregnancy for 2 years. She is currently using no contraceptive. What is her contraceptive status?
A. No contraception needed — exclusive breastfeeding alone prevents pregnancy indefinitely
B. She is protected by LAM for now (all three conditions met), but should be counselled to start a reliable method within 2 months when LAM conditions will expire
C. She has unmet need because breastfeeding does not provide contraceptive protection
D. She should immediately start the combined oral contraceptive pill to ensure reliable protection
Reveal Answer
Answer: B. She is protected by LAM for now (all three conditions met), but should be counselled to start a reliable method within 2 months when LAM conditions will expire
LAM (Lactational Amenorrhoea Method) is 98% effective when ALL three conditions are met simultaneously: (1) exclusive breastfeeding, (2) amenorrhoea, and (3) infant under 6 months. She currently satisfies all three, so she has effective contraceptive protection right now and is NOT counted as having unmet need. However, LAM expires when ANY condition changes — the infant will be 6 months old in 2 months, after which LAM is no longer reliable. She should be counselled NOW to choose a long-acting method to begin at 6 months. COC (Option D) is WHO MEC category 3 while she is exclusively breastfeeding an infant under 6 months, because estrogen suppresses milk production.
Temporary Contraceptive Methods: Mechanism, Advantages, Limitations
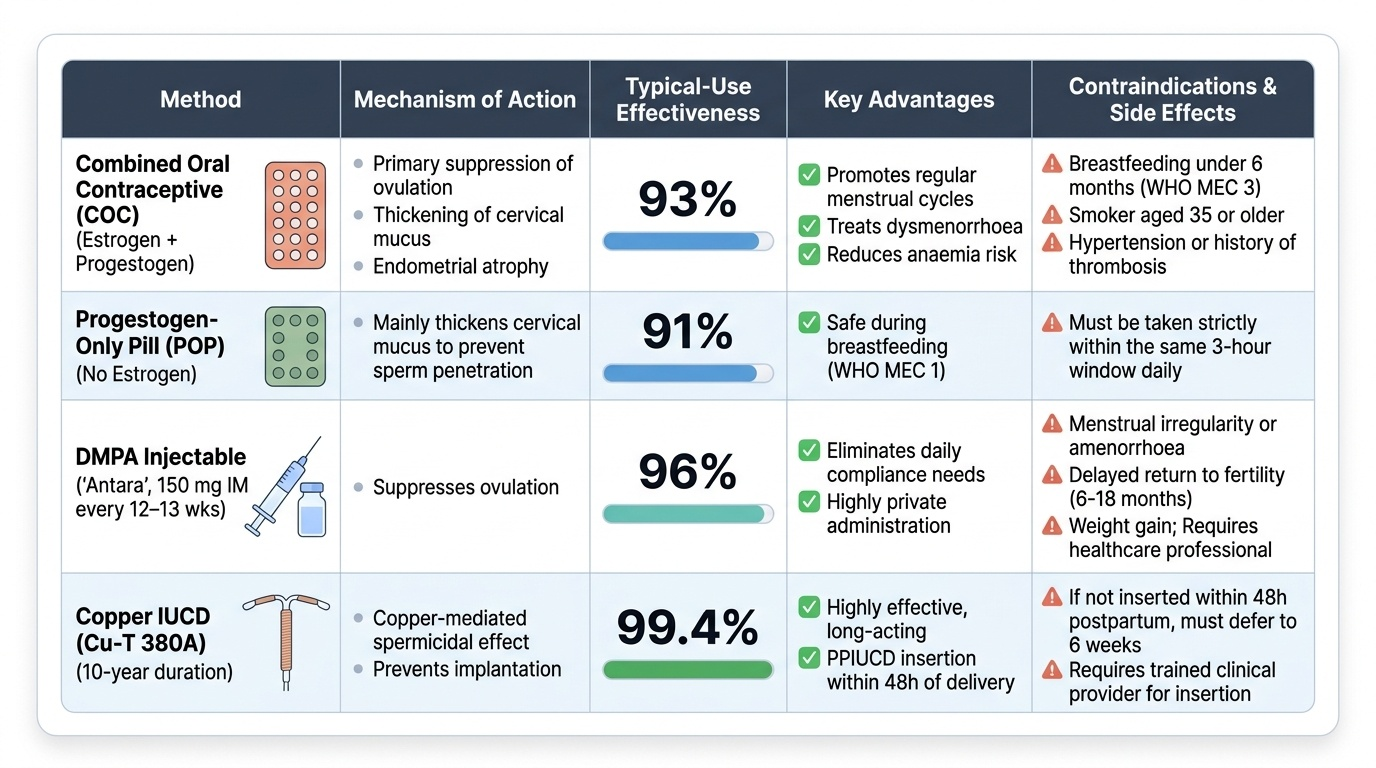
Temporary (reversible) contraceptive methods allow a return to fertility after discontinuation and are appropriate for birth spacing as well as for limiting — they are the programme's tool for meeting the needs of the 9.4% with unmet need who do not want permanent sterilization. Combined oral contraceptive pill (COC): estrogen + progestogen combination; mechanism — ovulation suppression (primary), cervical mucus thickening, endometrial atrophy; typical-use effectiveness 93%; advantages — regular cycles, treatment for dysmenorrhoea, reduced anaemia; contraindications include breastfeeding under 6 months (WHO MEC 3 — estrogen suppresses lactation), smoking plus age >35, hypertension, history of thrombosis. Progestogen-only pill (POP): no estrogen; mechanism — mainly cervical mucus effect; safe during breastfeeding (WHO MEC 1); must be taken within the same 3-hour window daily for maximal effectiveness; typical-use 91%. DMPA injectable (Depot Medroxyprogesterone Acetate): 150 mg IM every 12-13 weeks; marketed under the Antara programme in India (ASHAs supply from PHC, given by ANM at sub-centre); mechanism — ovulation suppression; typical-use 96%; advantage — non-daily compliance, privacy; limitations — menstrual irregularity/amenorrhoea, delayed return to fertility (6-18 months), weight gain, not self-administered. Intrauterine Contraceptive Device (IUCD): Cu-T 380A (copper-bearing, 10-year duration, 99.4% effectiveness) works via copper-mediated spermicidal and anti-implantation effect; PPIUCD (postpartum IUCD) must be inserted within 48 hours of delivery before uterine involution, during which the os is sufficiently open and the uterus well-demarcated; after 48 hours, insertion is deferred to 6 weeks postpartum (interval IUCD). Advantage: highly effective long-acting reversible contraception (LARC) requiring no daily compliance. Limitations: menstrual irregularity (heavier periods with copper IUCDs), expulsion rate 3-5% in first year, not protective against STIs. Emergency Contraception Pill (ECP): levonorgestrel 1.5 mg as a single dose taken within 72 hours of unprotected intercourse; efficacy is approximately 85% when taken within 72 hours and approximately 58% between 72-120 hours; mechanism — delays or inhibits ovulation, does not terminate an established pregnancy. Condom (male): typical-use 87%; sole method that provides dual protection (contraception + STI prevention including HIV); promoted under the Social Marketing Programme. LAM: effective only when all three conditions are simultaneously met — exclusive breastfeeding, amenorrhoea, and infant under 6 months; efficacy drops sharply when any condition is absent.
Provided image