Page 12 of 20
DR12.5 | Cutaneous Adverse Drug Reaction Primary Care — SDL Guide
Learning Objectives
- Provide appropriate primary care for patients with cutaneous adverse drug reactions across the severity spectrum.
- Apply the single most important step — immediate cessation of the culprit drug — to every adverse drug reaction.
- Manage mild to moderate reactions (maculopapular rash, fixed drug eruption, urticaria) at primary-care level.
- Deliver burns-model stabilisation for SJS/TEN — fluids, skin/wound care, analgesia, mucosal care — and arrange emergency transfer.
- Recognise which interventions are NOT the primary-care doctor's role and document the reaction for pharmacovigilance.
INSTRUCTIONS
Once you can recognise a cutaneous adverse drug reaction, the next responsibility is to act correctly — and the right action ranges from simple reassurance to life-saving emergency care. This module builds on the recognition skills of the companion module and teaches what the primary-care doctor actually does (competency DR12.5): the universal first step of stopping the culprit drug, the graded management of mild to severe reactions, and the burns-model stabilisation and urgent transfer that a patient with Stevens-Johnson syndrome or toxic epidermal necrolysis needs. Equally important is knowing the limits of primary care — which treatments to begin and which to leave for the specialist.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Cutaneous Adverse Drug Reactions — Management (textbook)
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Section: Management of Severe Cutaneous Adverse Drug Reactions (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 40-year-old man walks into a primary health centre with a rash. Over the consultation you notice his lips are raw and crusted, his eyes are red and weeping, and the skin on his chest, when you press it lightly, slides and peels. He started a sulfa antibiotic ten days ago. This is toxic epidermal necrolysis beginning to unfold — and the nearest burns unit is three hours away. What you do in this room over the next half hour, with only the resources of a basic health centre, will shape whether this man survives the journey. The single most important thing is something you can do immediately and for free: stop the drug. This module is about everything that follows — the primary care that keeps such a patient alive until specialist help is reached.
WHY THIS MATTERS
Recognising a severe drug reaction is only half the job; the patient's survival often depends on what the first doctor does before any specialist is involved. For mild reactions, correct primary care — stopping the drug, simple symptomatic treatment, and clear advice — resolves the problem and prevents a dangerous re-challenge. For severe reactions like DRESS and SJS/TEN, the primary-care doctor's stabilisation and timely referral are genuinely life-saving, and errors — failing to stop the drug, attempting unproven treatments, or delaying transfer — cost lives. Competency DR12.5 asks you to provide this primary care competently and to know its limits, which is one of the most directly life-saving skills a generalist can possess.
RECALL
Recall three things that make sense of the management that follows. First, from the companion module: the severe cutaneous reactions are fixed drug eruption (benign, same-site recurrence), DRESS (long latency, eosinophilia, organ involvement) and the SJS/TEN spectrum (epidermal detachment graded by body surface area — SJS less than 10%, overlap 10–30%, TEN more than 30%). Second, from surgery and physiology: a major burn loses fluid, heat and protein through the lost skin barrier and is at high risk of infection — exactly the physiology of TEN, which is why TEN is managed like a burn. Third, the principle of pharmacovigilance: every adverse drug reaction should be documented and reported so future harm is prevented. These ideas frame primary-care management.
The Doctor's First Duty: Recognise Severity and Act
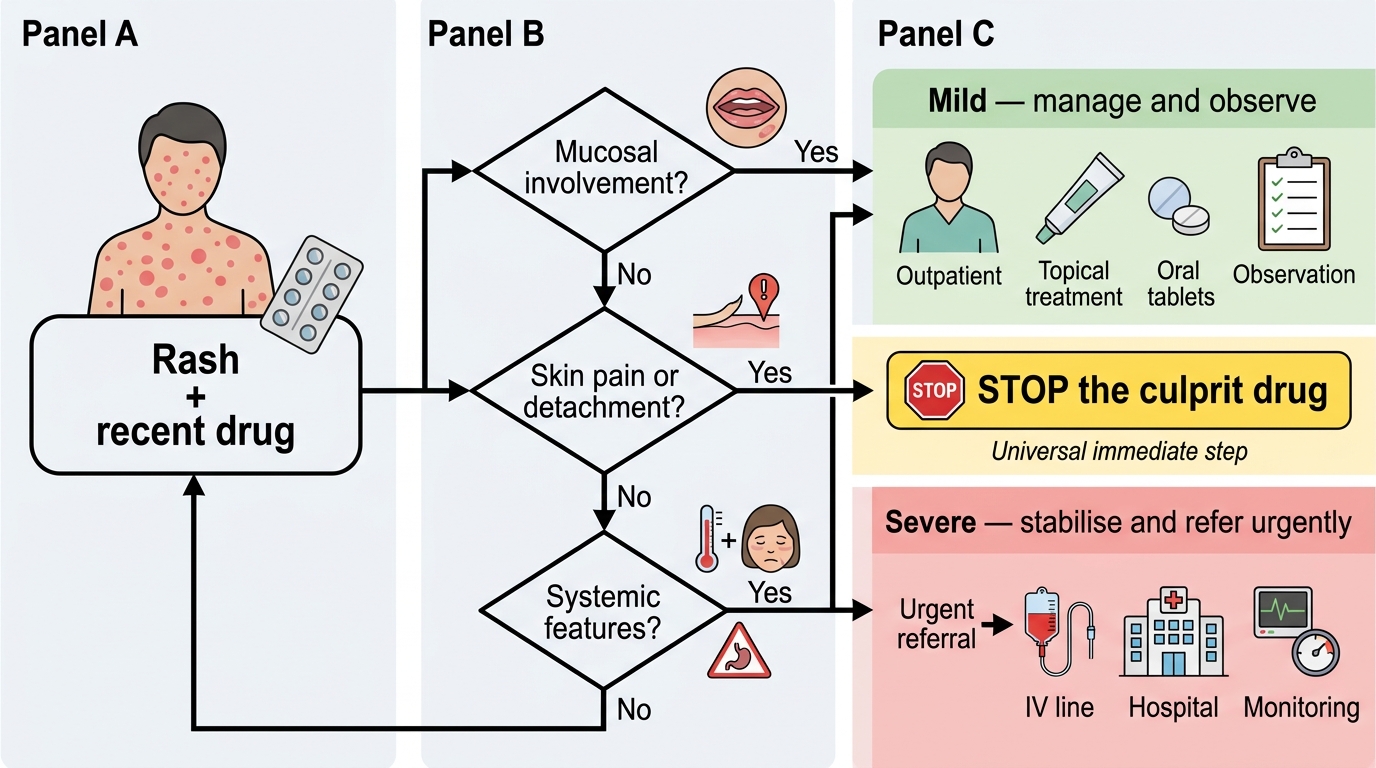
When a patient presents to a primary-care setting with a possible drug reaction, the doctor's first duty is a rapid severity triage that determines everything that follows. Within the first minutes you must decide whether this is a mild reaction that can be managed and observed, or a severe reaction that demands stabilisation and urgent referral. The triage rests on a few quick observations: are the mucous membranes (eyes, mouth, genitals) involved; is the skin painful or detaching rather than merely itchy; is the patient systemically unwell with fever, facial swelling or signs of organ dysfunction? Any of these moves the patient instantly into the severe category.
Whatever the severity, one action is universal and immediate: identify and stop the culprit drug. This is the single most important step in managing any adverse drug reaction, it can be done anywhere with no resources, and in SJS/TEN every hour of delay in stopping the drug worsens the outcome. The first duty, then, is simple to state and decisive in effect — recognise how severe the reaction is, and stop the offending drug at once — and the rest of this module elaborates the graded care that follows from that triage.
Drug Reaction Triage: Mild versus Severe
- First duty: rapid severity triage — mild versus severe.
- Severity flags: mucosal involvement, skin pain/detachment, systemic features (fever, facial oedema, organ dysfunction).
- Universal immediate step: identify and stop the culprit drug — the single most important action, free and possible anywhere.
Why Stopping the Drug Is Not Enough: Pathogenesis After Exposure
Why Drug Withdrawal Alone Is Not Enough
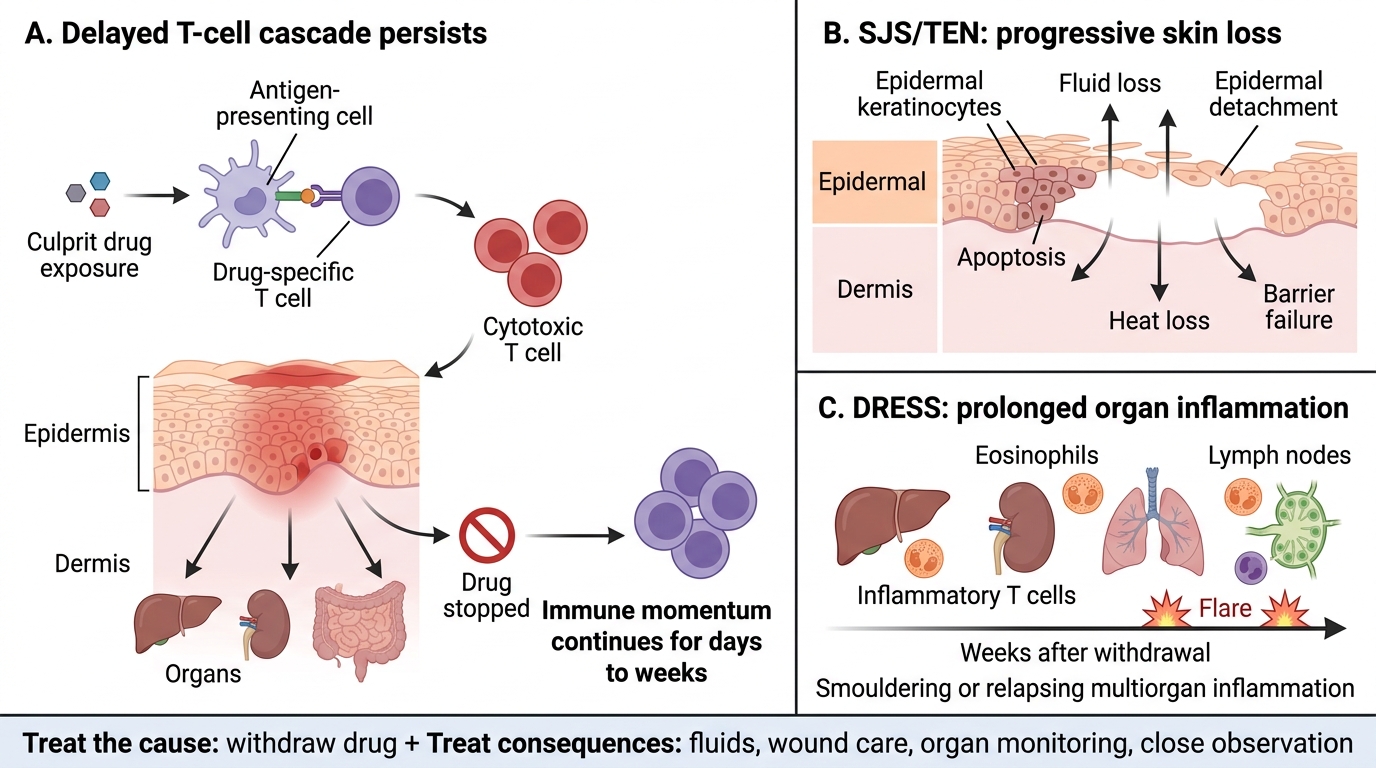
Stopping the culprit drug is essential, but understanding why it is not by itself sufficient explains the supportive care that severe reactions demand. These are delayed, T-cell-mediated reactions, and the immune process they set in motion has its own momentum: once activated, the drug-specific and cytotoxic T cells continue to drive tissue damage for days even after the triggering drug has been cleared. In SJS/TEN, the cascade of keratinocyte apoptosis and epidermal detachment progresses for several days after drug withdrawal, so the skin loss — and the consequent fluid, heat and barrier failure — continues and must be actively managed. In DRESS, the multiorgan inflammation and eosinophilic injury can smoulder or even flare for weeks, which is why organ function must be monitored well after the drug is stopped.
This ongoing pathology is the rationale for everything beyond drug cessation: the fluid replacement and wound care of TEN, the organ monitoring of DRESS, and the close observation of any patient whose reaction has not yet declared its full extent. Stopping the drug halts further immune provocation, but it does not reverse the damage already initiated. The primary-care doctor must therefore treat both the cause (withdraw the drug) and the consequences (support the failing skin and organs) — and recognise that a patient may deteriorate over the hours after presentation even though the drug has been stopped.
- Severe reactions are delayed, T-cell-mediated and have self-sustaining momentum.
- SJS/TEN: epidermal detachment progresses for days after the drug is stopped — barrier failure must be managed actively.
- DRESS: organ inflammation can persist or flare for weeks — monitor organ function after withdrawal.
- Implication: treat the cause (stop drug) AND the consequences (support skin/organs); expect possible deterioration after presentation.
SELF-CHECK
Which single action is the most important first step in managing ANY cutaneous adverse drug reaction, from a mild rash to toxic epidermal necrolysis?
A. Start a systemic corticosteroid
B. Identify and immediately stop the culprit drug
C. Apply a potent topical steroid to the whole body
D. Re-challenge with a smaller dose to confirm the culprit
Reveal Answer
Answer: B. Identify and immediately stop the culprit drug
Identifying and immediately stopping the culprit drug is the single most important step in every adverse drug reaction. It halts further immune provocation, requires no special resources, and in SJS/TEN delay in stopping the drug directly worsens outcome. Re-challenge is dangerous and contraindicated.
Managing Mild to Moderate cADRs at Primary Care Level
Primary Care Management of Mild to Moderate cADRs
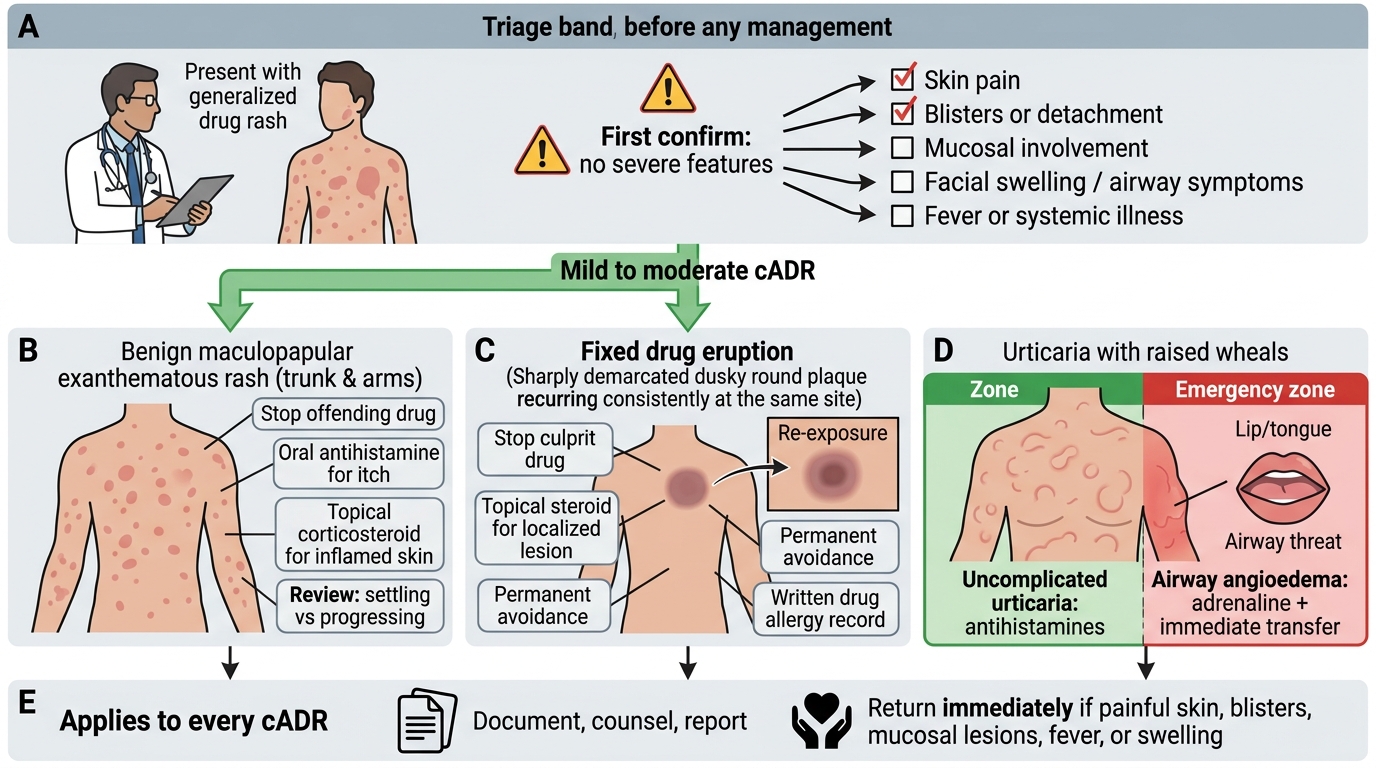
The great majority of drug reactions are mild to moderate and are fully within the scope of primary care, provided the doctor first confirms there are no severe features. For a benign maculopapular (exanthematous) rash, stopping the offending drug, prescribing an oral antihistamine for itch and a topical corticosteroid for the inflamed skin, and reviewing the patient to ensure the rash settles rather than progresses, is sufficient. For a fixed drug eruption, the management is to stop the culprit drug, treat the localised lesion with a topical steroid (or systemic steroid only if it is the rare generalised bullous variant), and — critically — counsel the patient to permanently avoid that drug, since re-exposure reliably reproduces the lesion. For urticaria, antihistamines are the mainstay, with the important exception that angioedema threatening the airway is an emergency requiring adrenaline and immediate transfer.
Two responsibilities apply to every reaction, however mild. The first is documentation and counselling: record the reaction clearly in the patient's notes, tell the patient (and ideally provide a written record) the name of the drug to avoid in future, and report the reaction through the pharmacovigilance system so the information is captured. The second is vigilance for progression: a rash that looked mild can evolve, so safety-net advice — return immediately if the skin becomes painful, blisters, the mucous membranes are involved, or fever develops — must be given to every patient sent home.
| Reaction | Primary-care management | Key responsibility |
|---|---|---|
| Maculopapular rash | Stop drug; antihistamine; topical steroid; review | Safety-net advice; document |
| Fixed drug eruption | Stop drug; topical steroid (systemic if generalised bullous) | Counsel lifelong avoidance |
| Urticaria | Antihistamine; adrenaline + transfer if airway angioedema | Watch for anaphylaxis |
| Any reaction | Stop culprit drug | Document + report (pharmacovigilance) |