Page 13 of 20
DR12.5 | Cutaneous Adverse Drug Reaction Primary Care — SDL Guide (Part 2)
Primary Care Response to DRESS
Primary Care Response to DRESS
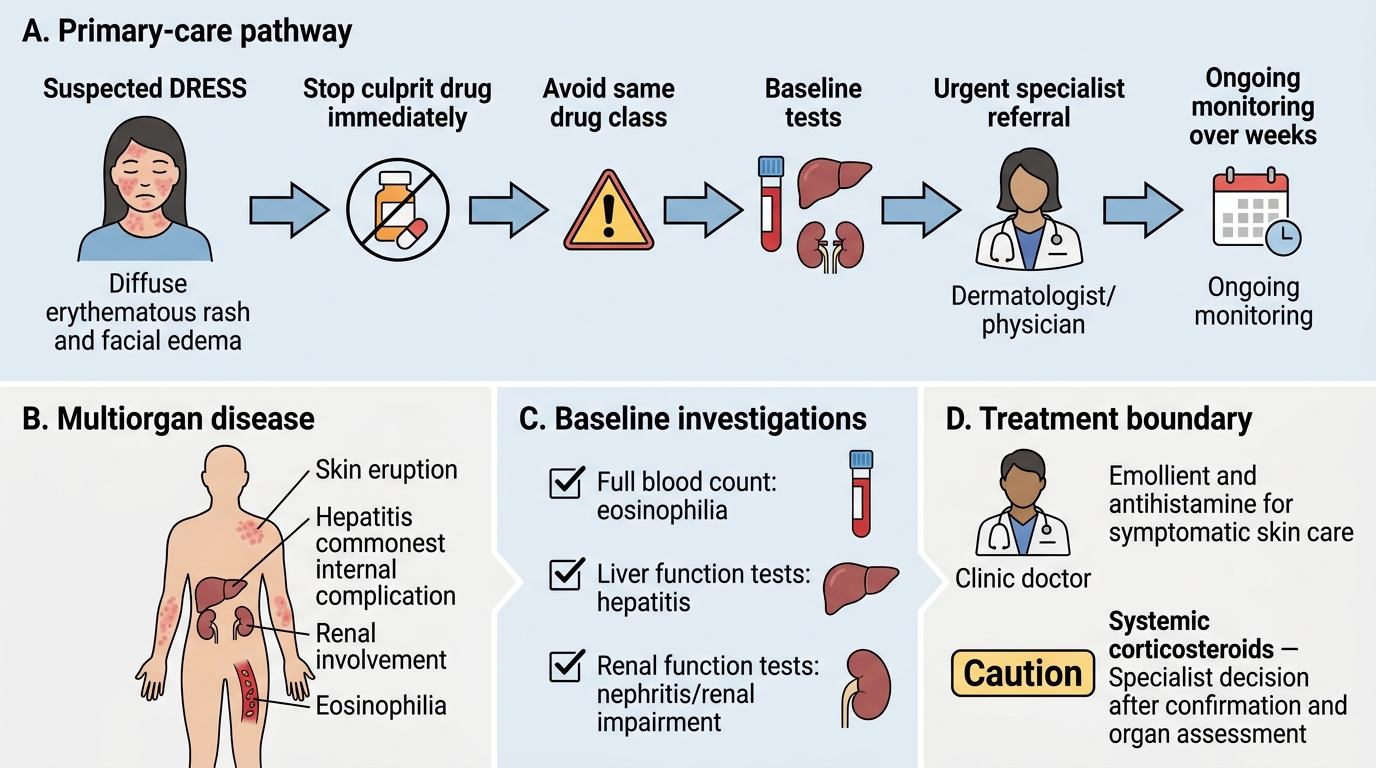
DRESS sits at the severe end of the spectrum, and the primary-care response is shaped by the fact that it is a multiorgan disease with a tendency to persist. The immediate steps are to stop the culprit drug at once — and, importantly, to avoid restarting any drug of the same class, because cross-reactivity within a class (notably the aromatic anticonvulsants) is common — and to obtain baseline investigations that reveal the extent of organ involvement: a full blood count for eosinophilia, and liver and renal function tests, since hepatitis is the commonest internal complication. The patient should be kept under observation and the affected skin treated symptomatically with emollients and antihistamines while these results guide the urgency of referral.
The key boundary for the primary-care doctor is that the definitive treatment of DRESS — systemic corticosteroids — is a specialist decision made after the diagnosis is confirmed and organ involvement assessed; it is not something to be started reflexively at first contact. The correct primary-care pathway is therefore: stop the drug, establish baseline organ function, treat the skin symptomatically, refer urgently to a dermatologist or physician, and arrange continued monitoring of liver and renal function because organ inflammation can flare over the following weeks. Recognising that DRESS needs specialist-led systemic therapy, not a quick course of steroids from the clinic, is part of competent primary care.
- Stop the culprit drug immediately; avoid the whole drug class (cross-reactivity, e.g. aromatic anticonvulsants).
- Baseline investigations: full blood count (eosinophilia), liver and renal function (organ involvement).
- Symptomatic skin care: emollients, antihistamines.
- Refer urgently: systemic corticosteroids for DRESS are a specialist decision after diagnosis is confirmed.
- Continued monitoring: organ function over the following weeks, as DRESS can flare.
SJS/TEN: Burns-Model Stabilisation and Emergency Transfer
SJS/TEN: Burns-Model Stabilisation and Emergency Transfer
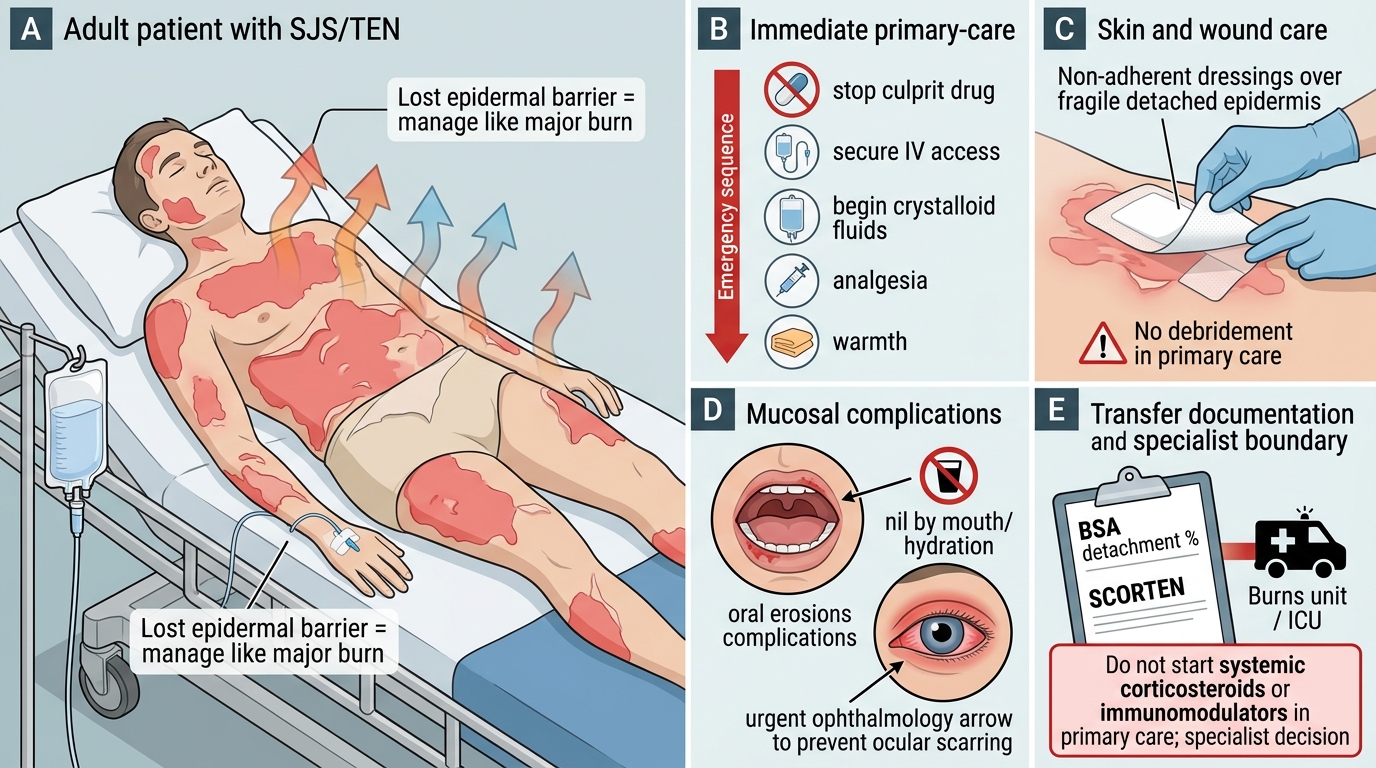
SJS/TEN is a dermatological emergency, and the primary-care response is built on a single analogy: because the patient has lost the epidermal barrier, manage it like a major burn while arranging urgent transfer to a burns unit or intensive care. The sequence begins, as always, with stopping the culprit drug immediately. Then secure intravenous access and begin fluid resuscitation with crystalloid, because fluid loss through the denuded skin is the immediate threat, just as in a burn. Provide skin and wound care with non-adherent dressings, handling the fragile skin gently and avoiding any debridement at primary-care level. Maintain warmth and temperature control, because the lost barrier cannot regulate heat, and give adequate analgesia, as the raw skin is extremely painful.
The mucosal complications need specific attention: if there is oral mucosal involvement the patient may need to be kept nil by mouth with attention to hydration, and eye involvement demands urgent ophthalmology input because ocular scarring can cause permanent blindness. Throughout, document the estimated body surface area of detachment and, where possible, the SCORTEN severity, which guide the receiving unit. The decisive boundary is that the primary-care doctor does not start systemic corticosteroids or other immunomodulatory therapy — their use in TEN is debated and potentially harmful, and is a specialist decision; the primary-care role is to stabilise, support and transfer. Arrange emergency transfer without delay, continuing fluids and supportive care en route.
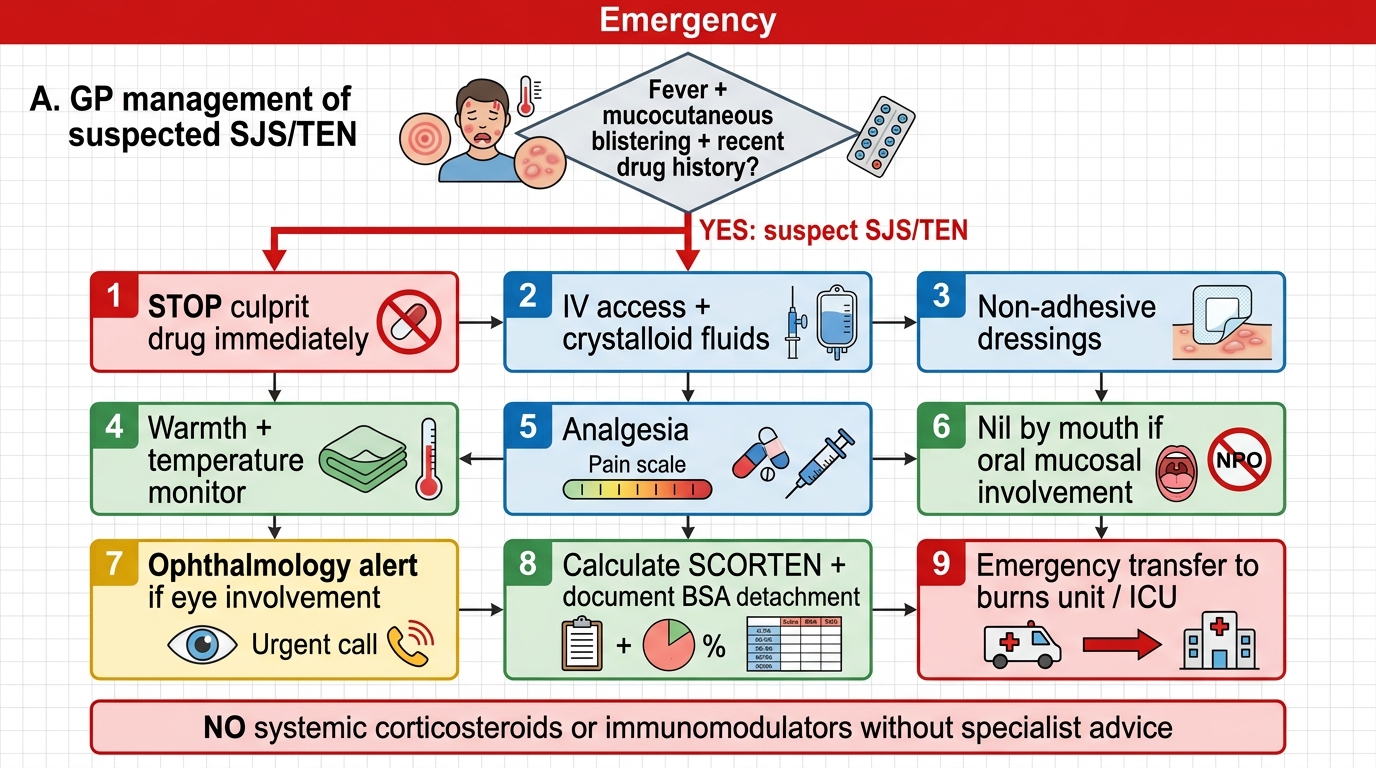
GP Emergency Management of Suspected SJS/TEN
- Stop the culprit drug immediately.
- Burns-model care: IV fluids (crystalloid) for skin losses; non-adherent dressings, gentle handling, no debridement; warmth and temperature control; analgesia.
- Mucosal care: nil by mouth if oral involvement; urgent ophthalmology for eye involvement.
- Assess and document: BSA of detachment and SCORTEN.
- Do NOT start systemic corticosteroids/immunomodulators in primary care — specialist decision.
- Arrange emergency transfer to a burns unit/ICU, continuing care en route.
SELF-CHECK
A patient with toxic epidermal necrolysis (about 35% BSA detachment) presents to a primary health centre. Which action is NOT appropriate at the primary-care level?
A. Stop the culprit drug immediately
B. Begin intravenous fluid resuscitation and gentle wound care
C. Start high-dose systemic corticosteroids before transfer
D. Arrange urgent ophthalmology input and emergency transfer to a burns unit
Reveal Answer
Answer: C. Start high-dose systemic corticosteroids before transfer
Starting systemic corticosteroids in TEN is a specialist decision — their benefit is debated and they may be harmful — and is NOT the primary-care doctor's role. The correct primary-care actions are to stop the drug, give burns-model supportive care (fluids, wound and mucosal care, analgesia, warmth), and arrange urgent transfer.
Differential and Investigations in Primary Care
Primary-Care Differentiation of Severe Drug Reactions
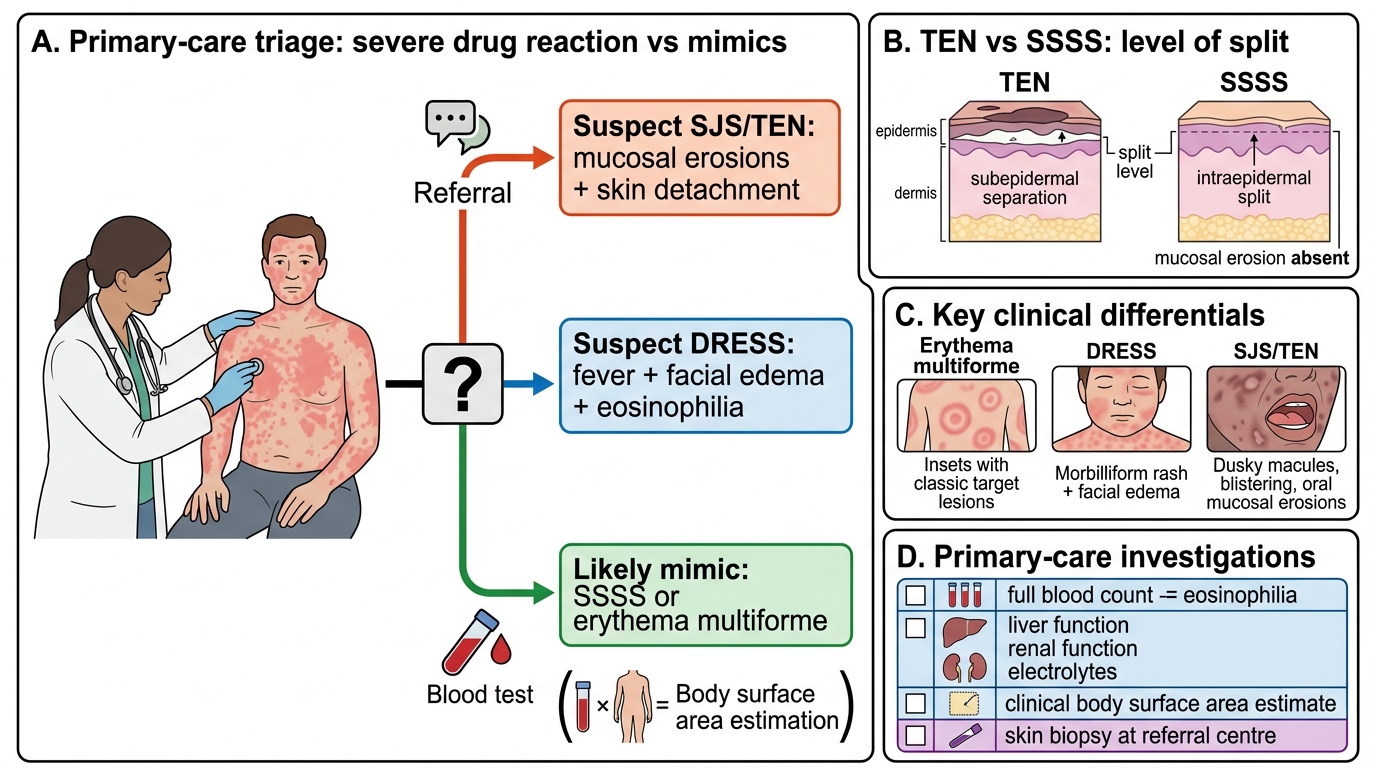
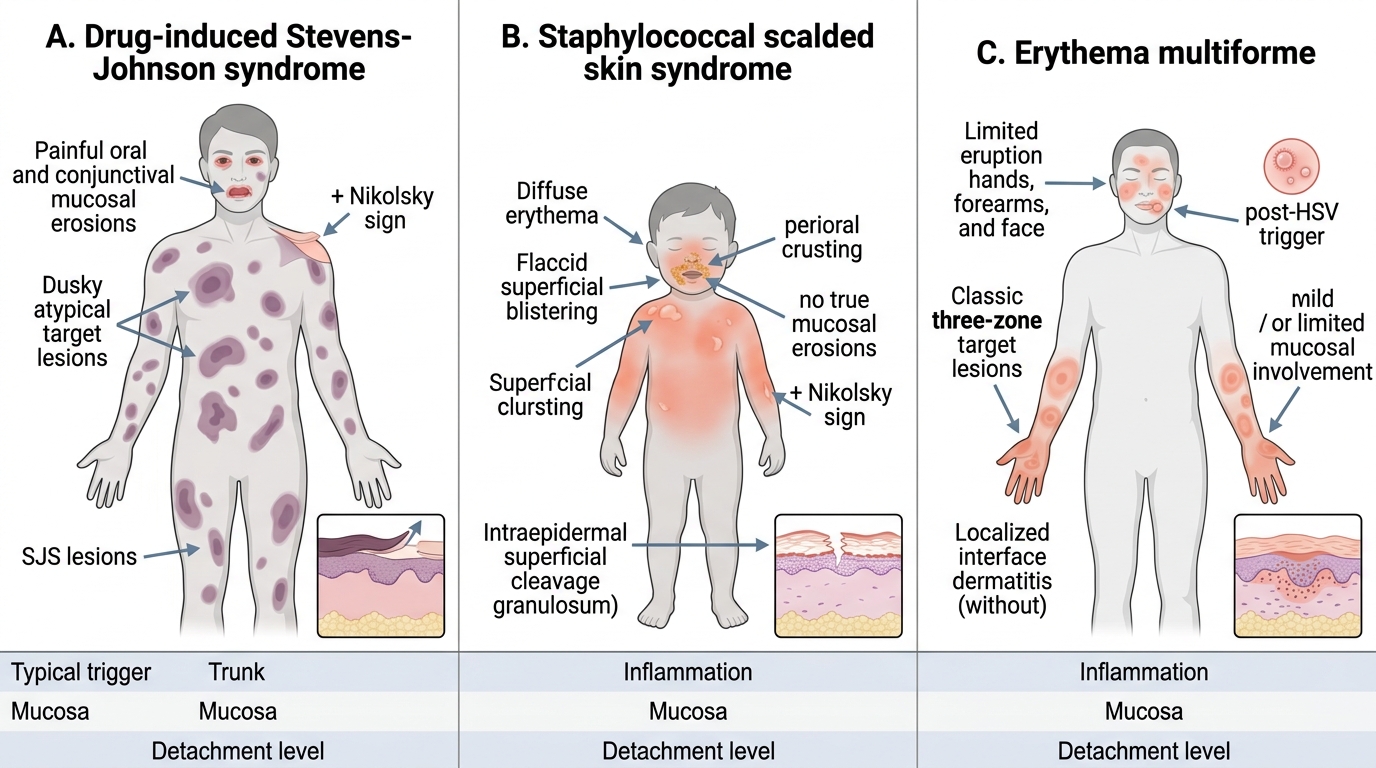
Correct primary-care management depends on not confusing a severe drug reaction with its mimics, since the treatment paths diverge sharply. The most important differential of TEN is staphylococcal scalded skin syndrome (SSSS), a toxin-mediated condition that mainly affects young children, produces a more superficial split with perioral crusting, and — crucially — does not cause the true mucosal erosions of SJS/TEN; SSSS needs antistaphylococcal antibiotics, not burns-type care for an immune reaction. Erythema multiforme, with its classic target lesions and frequent association with herpes simplex, is usually a milder, more limited condition that should not be over-treated as TEN. A widespread morbilliform drug rash with fever and a swollen face should prompt thought of DRESS rather than a simple exanthem.
The investigations available at primary-care level are modest but useful. A full blood count can reveal the eosinophilia of DRESS; basic biochemistry (liver and renal function, electrolytes) detects organ involvement and the metabolic disturbance of extensive skin loss; and clinical estimation of body surface area grades SJS/TEN. Definitive tests such as skin biopsy (to confirm the level of the epidermal split and distinguish TEN from SSSS) are usually performed at the referral centre. The primary-care doctor's task is to use simple clinical discrimination and the available bedside and basic laboratory clues to reach a working diagnosis, treat accordingly, and refer — not to await a tissue diagnosis before acting.
Distinguishing SJS, SSSS, and Erythema Multiforme
- SSSS: young children, superficial split, perioral crusting, no true mucosal erosions — needs antibiotics, not burns care.
- Erythema multiforme: target lesions, often post-herpes, usually limited — do not over-treat as TEN.
- DRESS: morbilliform rash + fever + facial oedema — think DRESS, not simple exanthem.
- Primary-care tests: FBC (eosinophilia), biochemistry (organ/metabolic), BSA estimation; biopsy at referral centre.