Page 14 of 20
DR12.5 | Cutaneous Adverse Drug Reaction Primary Care — SDL Guide (Part 3)
Tier-by-Tier Management Summary
Tier-by-Tier Management of Drug Reactions
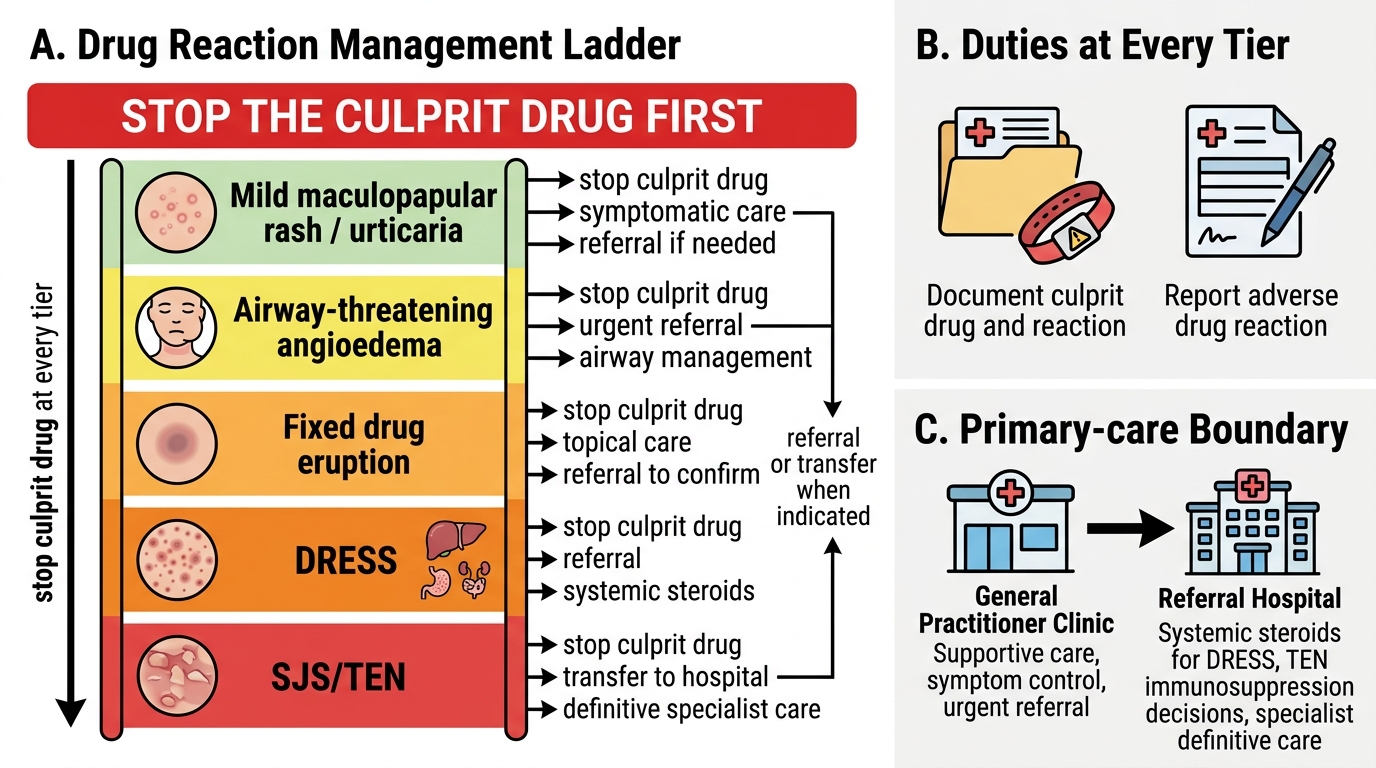
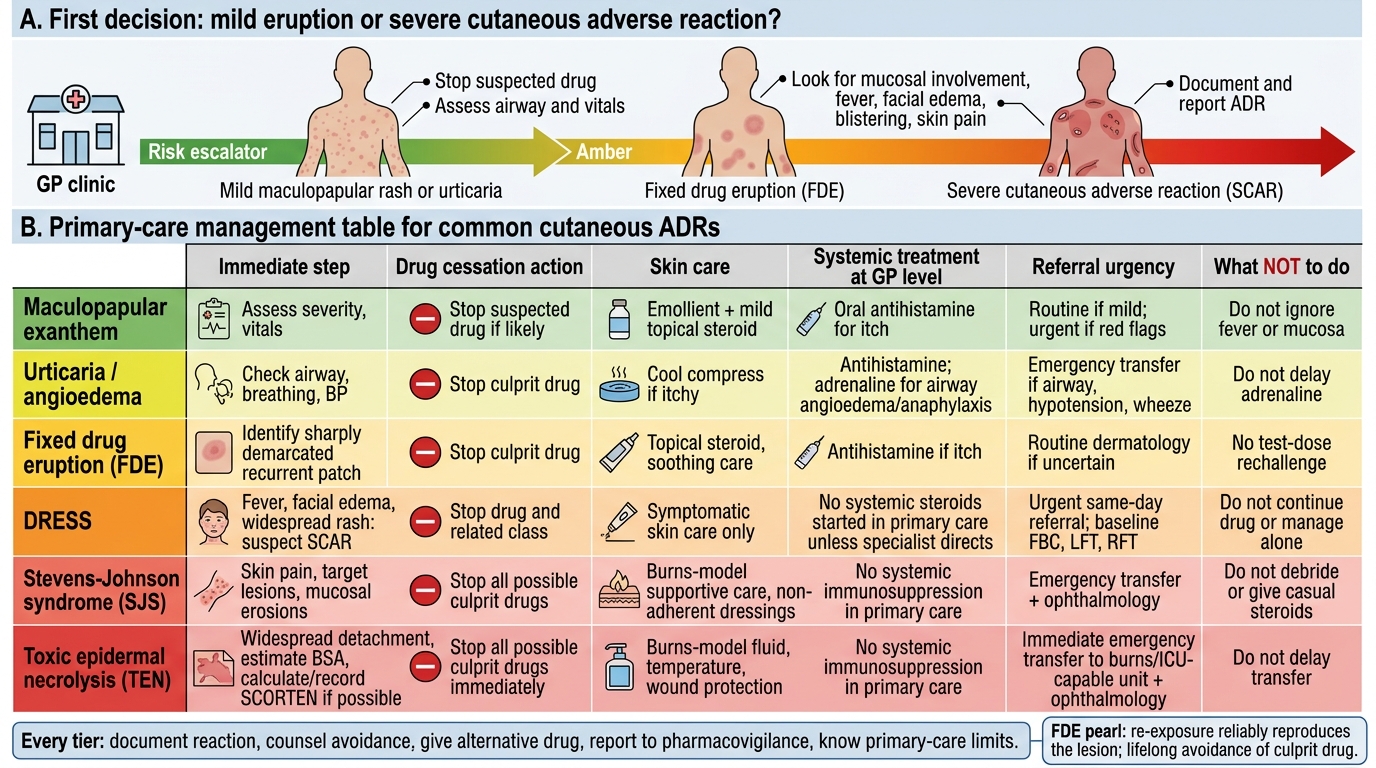
Bringing the management together as a single ladder makes the primary-care response easy to apply under pressure, with the constant rule that drug cessation is the first step at every tier. For a mild maculopapular rash or urticaria: stop the drug, give antihistamines and a topical steroid, provide safety-net advice, and treat airway-threatening angioedema with adrenaline and transfer. For a fixed drug eruption: stop the drug, topical steroid for the lesion, and counsel lifelong avoidance. For DRESS: stop the drug and its whole class, take baseline blood count and liver/renal function, treat the skin symptomatically, refer urgently, and leave systemic steroids to the specialist. For SJS/TEN: stop the drug, give burns-model care (fluids, wound and mucosal care, analgesia, warmth), arrange urgent ophthalmology and emergency transfer, document BSA/SCORTEN, and do not start systemic immunosuppression.
Across every tier, two duties never change. Pharmacovigilance: document the reaction and the culprit drug and report it, and ensure the patient knows what to avoid permanently. And knowing the limits of primary care: the generalist initiates supportive and symptomatic treatment and refers, but does not start the disputed or specialist-only therapies (systemic steroids in TEN, immunomodulators, definitive DRESS treatment) that belong to the referral centre. This combination — confident graded primary care plus clear boundaries — is exactly what competency DR12.5 requires.
Primary-Care Management of Cutaneous Adverse Drug Reactions
- Mild rash / urticaria: stop drug; antihistamine + topical steroid; adrenaline + transfer for airway angioedema.
- Fixed drug eruption: stop drug; topical steroid; counsel lifelong avoidance.
- DRESS: stop drug + class; baseline FBC/LFT/RFT; symptomatic skin care; refer urgently; systemic steroids = specialist.
- SJS/TEN: stop drug; burns-model care; urgent ophthalmology + emergency transfer; document BSA/SCORTEN; no systemic immunosuppression in primary care.
- Every tier: document + report (pharmacovigilance); know the limits of primary care.
SELF-CHECK
A patient had a fixed drug eruption to co-trimoxazole. He now needs an antibiotic again and asks if he can take co-trimoxazole at a lower dose to 'test' whether it still affects him. What is the correct advice?
A. Yes — a low-dose re-challenge safely confirms the diagnosis
B. No — re-exposure reliably reproduces the reaction; he must permanently avoid the culprit drug and be given an alternative
C. Yes — provided an antihistamine is taken alongside
D. It does not matter, as fixed drug eruption never recurs
Reveal Answer
Answer: B. No — re-exposure reliably reproduces the reaction; he must permanently avoid the culprit drug and be given an alternative
Re-exposure to the culprit drug reliably reproduces a fixed drug eruption at the same site (and may worsen or generalise it). Deliberate re-challenge is unsafe; the patient must be counselled to avoid that drug permanently and given a documented alternative — a core pharmacovigilance and primary-care responsibility.
Applying the Primary Care Response
Primary Care Response to Severe Drug Reactions
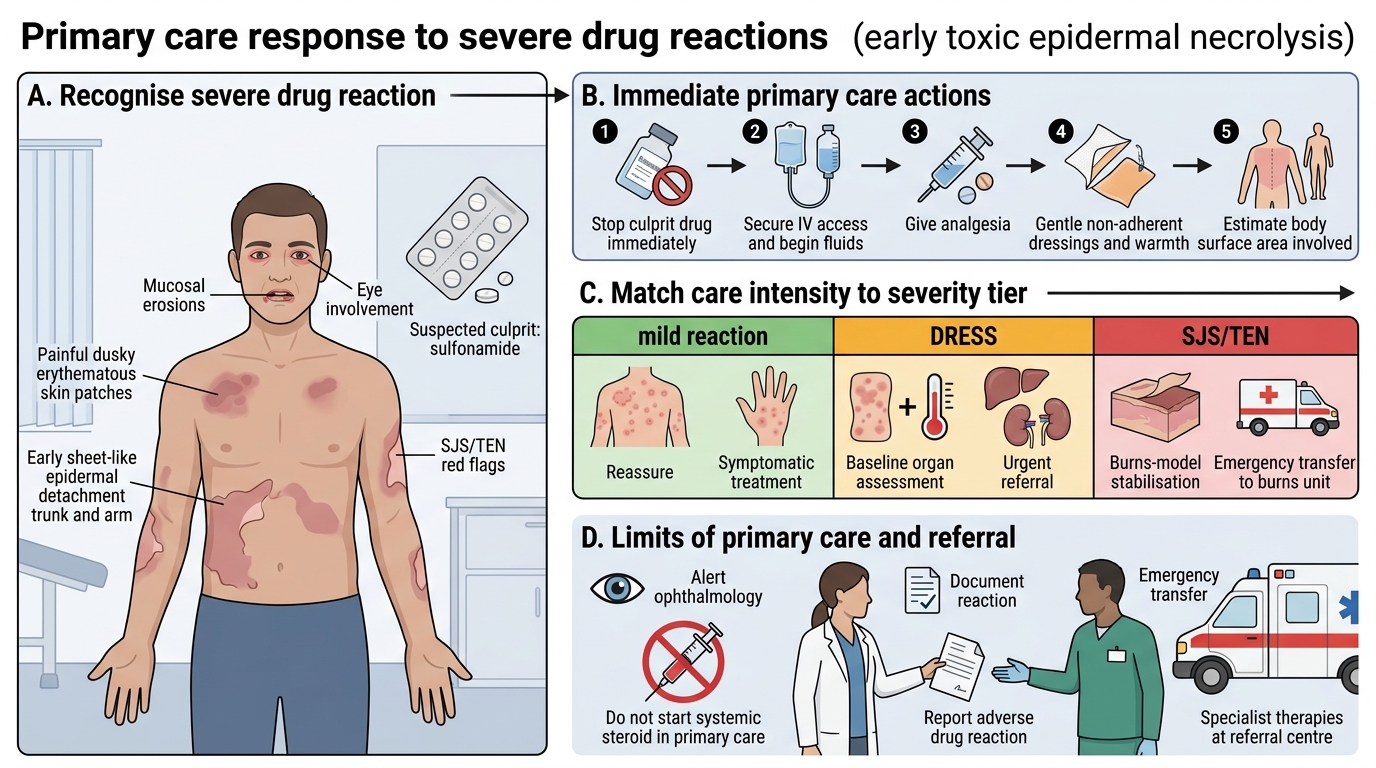
The final skill is to deploy this graded response fluently when a real patient with a drug reaction arrives. Return to the man with early toxic epidermal necrolysis from the opening: the correct sequence is to recognise the severe features (mucosal erosions, painful detaching skin), stop the sulfonamide immediately, secure intravenous access and begin fluids, provide gentle non-adherent wound care and warmth, give analgesia, alert ophthalmology for his eye involvement, estimate the body surface area involved, document the reaction, and arrange emergency transfer to a burns unit — all the while not reaching for a systemic steroid, which is not his to start. That ordered response, executed in a basic health centre, is what gives the patient the best chance.
Three principles should now be automatic. First, stop the culprit drug in every reaction, whatever its severity — it is always the most important step. Second, match the intensity of care to the tier: reassurance and symptomatic treatment for the mild, baseline organ assessment and urgent referral for DRESS, and burns-model stabilisation with emergency transfer for SJS/TEN. Third, know and respect the limits of primary care — initiate supportive treatment and refer, but leave specialist and disputed therapies to the referral centre, and always document and report the reaction so the patient is protected in future.
- Apply the sequence: recognise severity → stop the drug → tier-appropriate care → document → refer.
- For SJS/TEN: stop drug, fluids, wound/mucosal care, analgesia, ophthalmology, BSA/SCORTEN, emergency transfer — no systemic steroid in primary care.
- Three principles: always stop the culprit drug; match care to tier; respect the limits of primary care and document/report.
CLINICAL PEARL
When a severe drug reaction lands in front of you, anchor on two things you can always do regardless of resources: stop the culprit drug, and — for SJS/TEN — treat the patient like a burns case (fluids, gentle wound care, warmth, analgesia) while you arrange transfer. Resist the urge to 'do more' by starting systemic steroids in TEN: their benefit is unproven and they may cause harm, so that decision belongs to the specialist. Doing the simple, correct things well, and not the disputed things, is what saves these patients.