Page 9 of 20
DR12.4 | Cutaneous Adverse Drug Reaction Recognition — SDL Guide (Part 2)
DRESS: The Long-Latency Drug Reaction with Organ Involvement
DRESS: Delayed Drug Reaction with Systemic Organ Involvement
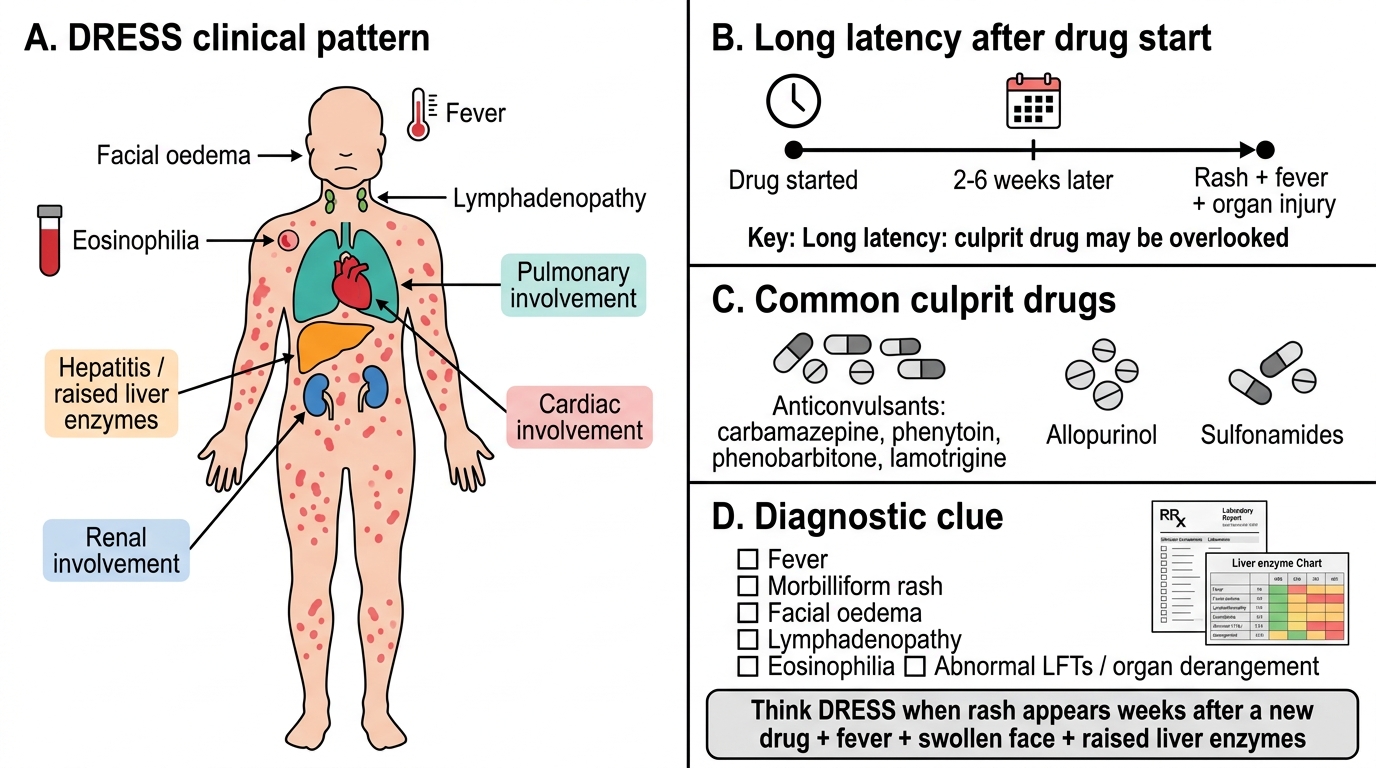
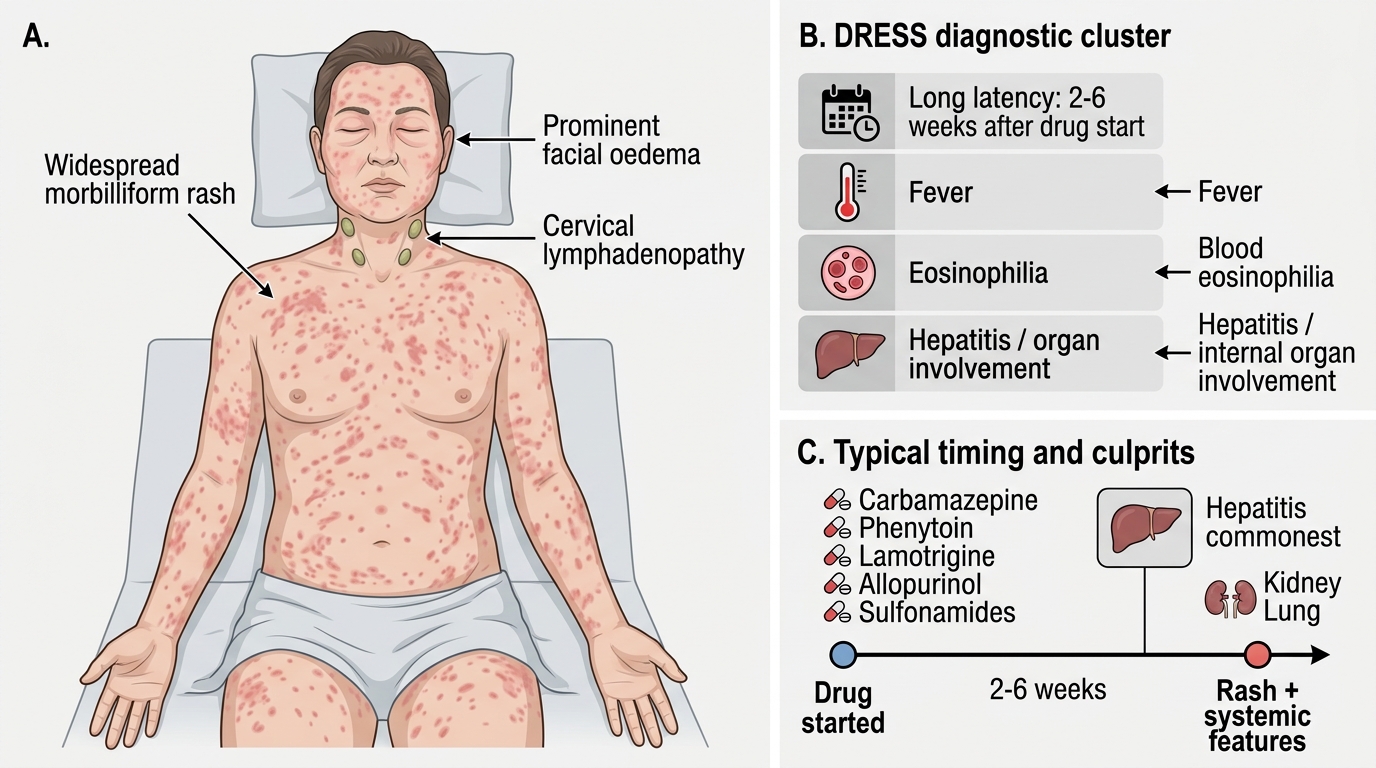
DRESS — Drug Reaction with Eosinophilia and Systemic Symptoms — is the great mimic, a severe hypersensitivity reaction that is dangerous precisely because it is more than skin-deep. Its cardinal distinguishing feature is long latency: unlike most drug rashes, DRESS typically begins two to six weeks after starting the culprit drug, so the offending agent may have been taken for weeks and is easily overlooked. The clinical picture combines a widespread morbilliform rash with a characteristically swollen face (facial oedema), fever, lymphadenopathy, and the two findings that name and define it: a blood eosinophilia and internal organ involvement, most commonly hepatitis (raised liver enzymes), but also the kidneys, lungs and heart. It is this internal organ injury that makes DRESS potentially fatal.
The culprit drugs are a recognisable group: anticonvulsants (carbamazepine, phenytoin, phenobarbitone, lamotrigine), allopurinol, and sulfonamides. Diagnosis is clinical, supported by the constellation of fever, rash, eosinophilia, lymphadenopathy and organ derangement (formalised in scoring systems such as RegiSCAR), and the key differentials are other drug rashes and an infectious illness such as infectious mononucleosis. The practical lesson is to think of DRESS in any patient who, weeks after starting a drug, develops a rash with fever, a swollen face and abnormal liver enzymes — and to check an eosinophil count and liver function as part of that suspicion.
DRESS: Rash, Facial Oedema and Systemic Involvement
- Long latency: onset typically 2–6 weeks after starting the drug (distinguishing feature).
- Skin & systemic: widespread rash, prominent facial oedema, fever, lymphadenopathy.
- Defining laboratory/organ features: blood eosinophilia + internal organ involvement (hepatitis commonest; also kidney, lung).
- Common culprits: anticonvulsants (carbamazepine, phenytoin, lamotrigine), allopurinol, sulfonamides.
- Differential: other drug rashes; infectious mononucleosis.
SELF-CHECK
A patient develops a rash, fever, swollen face and high eosinophil count with deranged liver enzymes four weeks after starting carbamazepine. Which reaction is this, and what feature is most characteristic?
A. Urticaria; immediate onset within minutes
B. DRESS; long latency (2–6 weeks) with eosinophilia and internal organ (liver) involvement
C. Fixed drug eruption; recurrence at the same site
D. Irritant contact dermatitis; exposure-dependent
Reveal Answer
Answer: B. DRESS; long latency (2–6 weeks) with eosinophilia and internal organ (liver) involvement
This is DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms). Its characteristic features are the LONG latency of 2–6 weeks after the drug, eosinophilia, facial oedema, lymphadenopathy and internal organ involvement (most often hepatitis) — distinguishing it from immediate or same-site reactions.
SJS and TEN: Epidermal Detachment by Body Surface Area
SJS-TEN Spectrum by Epidermal Detachment
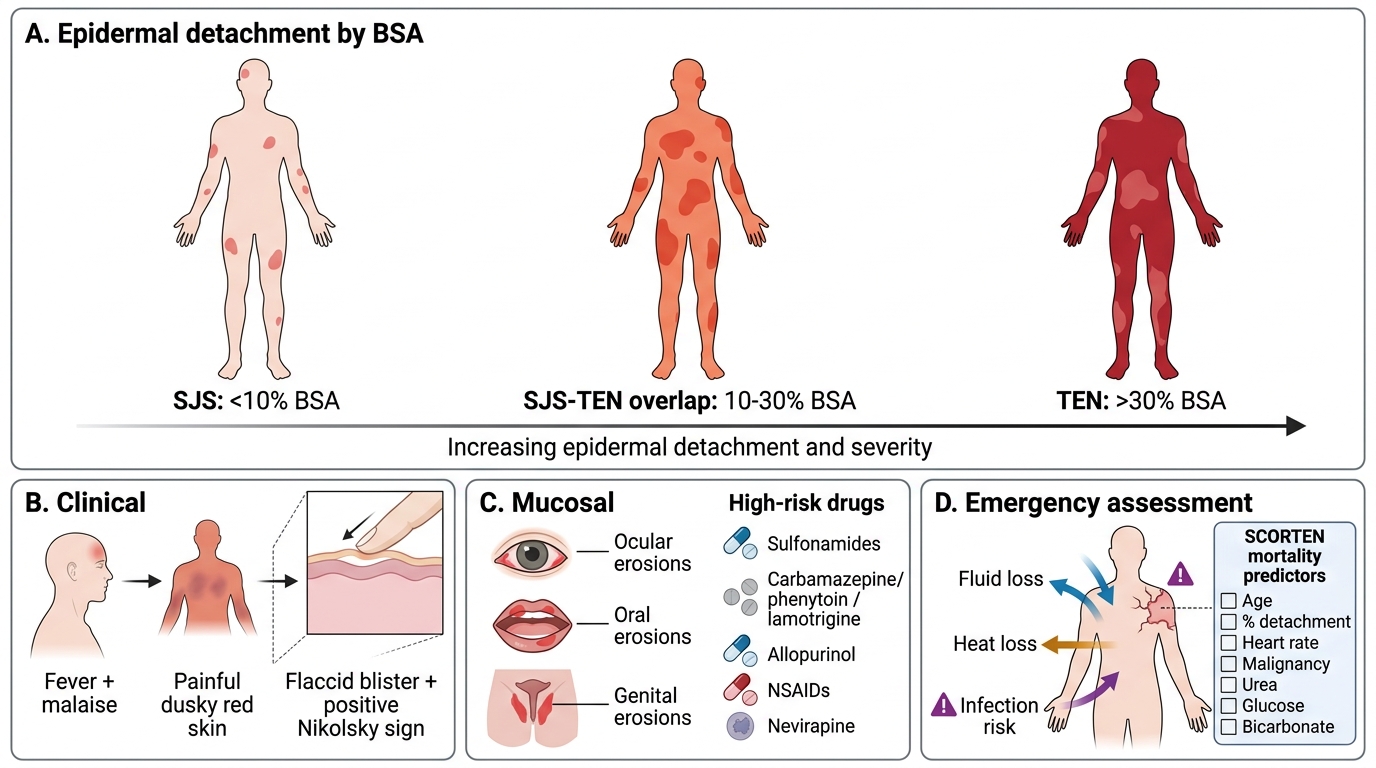
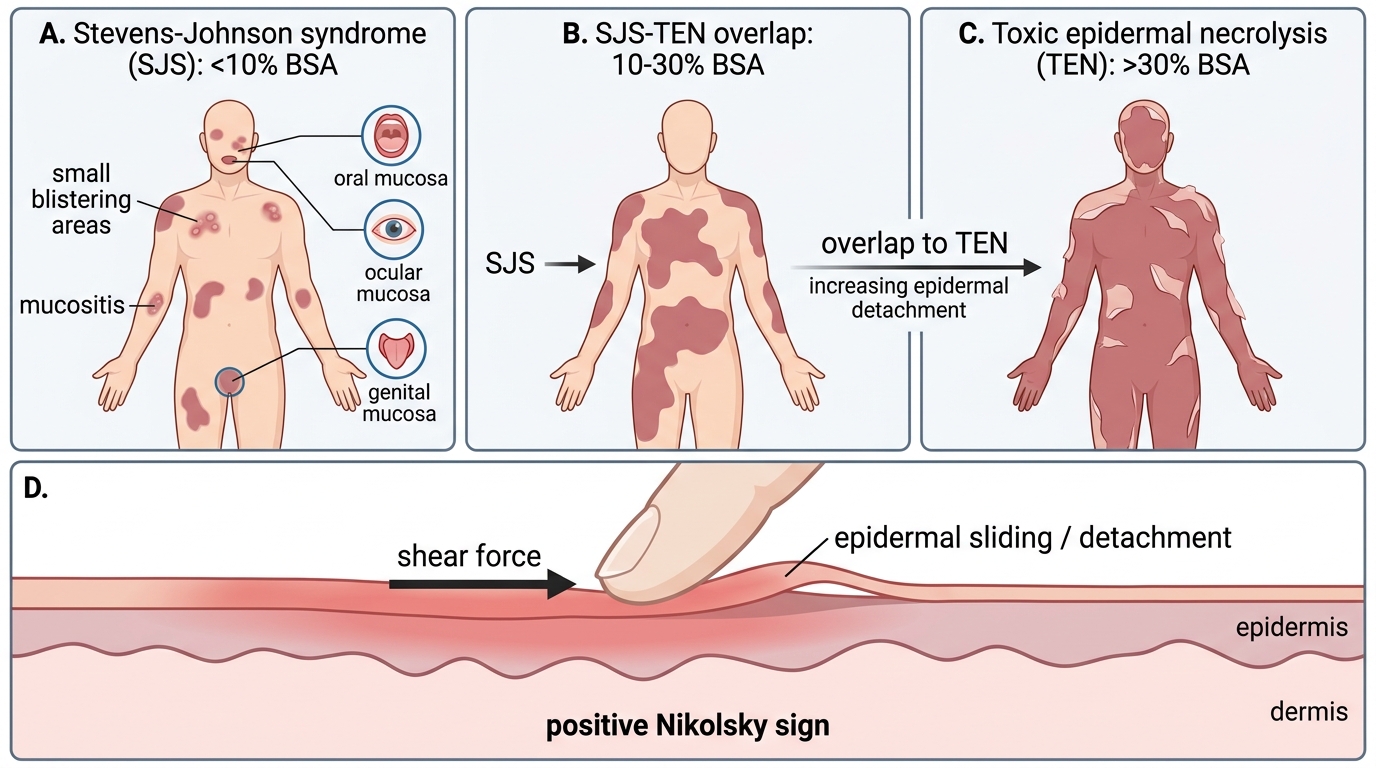
Stevens-Johnson syndrome and toxic epidermal necrolysis are the most feared cutaneous drug reactions, two ends of a single spectrum of epidermal death graded entirely by the percentage of body surface area that detaches. The defining cut-offs must be memorised exactly: Stevens-Johnson syndrome (SJS) is epidermal detachment of less than 10% BSA; SJS-TEN overlap is 10–30% BSA; and toxic epidermal necrolysis (TEN) is more than 30% BSA. Clinically the reaction begins with a prodrome of fever and malaise, followed by painful, dusky red skin and the development of flaccid blisters that slough to leave raw, denuded areas — the skin shears off with light pressure, a positive Nikolsky sign. Painful erosions of the mucous membranes — the eyes, mouth and genitals — are characteristic and often precede the skin detachment.
The culprit drugs are a well-defined list every clinician should know: sulfonamides, anticonvulsants (carbamazepine, phenytoin, lamotrigine), allopurinol, NSAIDs, and nevirapine. Severity and prognosis are formally assessed using the SCORTEN score, which combines age, the extent of detachment, heart rate, malignancy, and serum urea, glucose and bicarbonate to predict mortality. The reaction is an emergency because the loss of the epidermal barrier causes exactly the fluid, thermoregulatory and infective failures of a major burn — which is why TEN is managed like a burn. Recognising painful skin with mucosal erosions in a patient on one of these drugs, and grading it by BSA, is the critical recognition skill.
SJS-TEN Spectrum and Positive Nikolsky Sign
- BSA cut-offs: SJS <10%, SJS-TEN overlap 10–30%, TEN >30% epidermal detachment.
- Features: fever prodrome, painful dusky skin, flaccid blisters, sloughing, positive Nikolsky sign, painful ocular/oral/genital mucosal erosions.
- Culprit drugs: sulfonamides, anticonvulsants (carbamazepine, phenytoin, lamotrigine), allopurinol, NSAIDs, nevirapine.
- Severity score: SCORTEN predicts mortality.
- Why it is an emergency: epidermal loss = burns-like fluid, heat and infection failure.
Distinguishing These Reactions: Differential and Investigations
Differentiating Severe Drug Reactions and Mimics
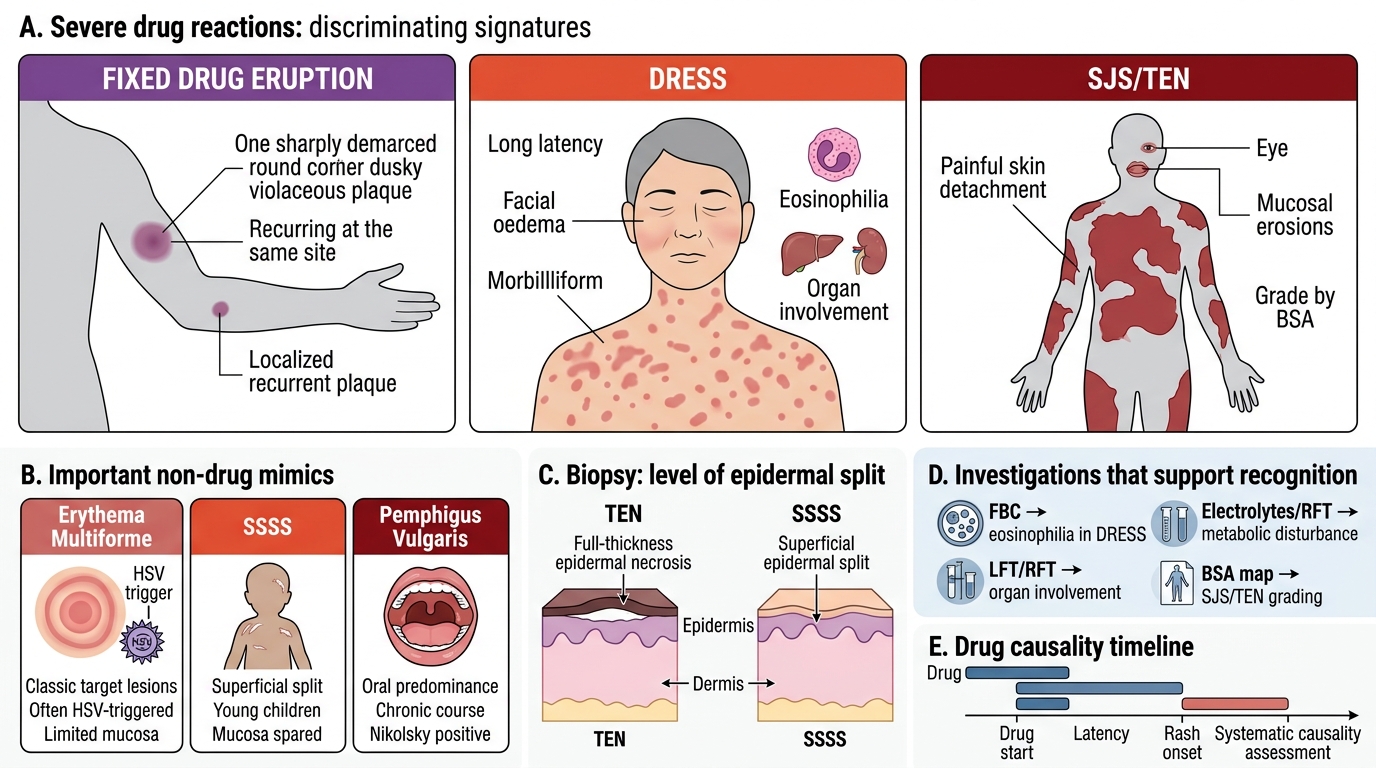
Putting the three severe reactions side by side, and distinguishing them from non-drug mimics, is the clinical reasoning at the heart of DR12.4. Each has a discriminating signature: a fixed drug eruption is localised and recurs at the same site; DRESS is defined by its long latency, facial oedema, eosinophilia and organ involvement; and SJS/TEN is defined by painful skin detachment with mucosal erosions, graded by BSA. The key non-drug mimics to keep in mind are erythema multiforme (classic target lesions, often triggered by herpes simplex rather than drugs, with limited mucosal involvement), staphylococcal scalded skin syndrome (a more superficial split, typically in young children, without true mucosal erosions), and pemphigus vulgaris (autoimmune blistering with a positive Nikolsky sign but a chronic course and oral predominance).
Investigations support but rarely replace clinical recognition. A skin biopsy distinguishes the level of the split — full-thickness epidermal necrosis confirms TEN, while a more superficial split suggests staphylococcal scalded skin syndrome. A full blood count reveals the eosinophilia of DRESS; liver and renal function tests detect the organ involvement of DRESS and the metabolic disturbance of TEN; and accurate BSA assessment grades the SJS/TEN spectrum. Drug causality is assessed systematically, noting the timing of each drug relative to onset. The combination of pattern recognition and these targeted tests reliably separates the reactions.
| Feature | Fixed drug eruption | DRESS | SJS/TEN |
|---|---|---|---|
| Onset/latency | Hours after re-exposure | 2–6 weeks | 1–3 weeks |
| Morphology | Few well-defined dusky plaques | Widespread rash + facial oedema | Painful skin, blisters, detachment |
| BSA / extent | Localised | Variable rash | Graded: SJS <10%, overlap 10–30%, TEN >30% |
| Mucosal involvement | Occasional (lips, genitals) | Uncommon | Prominent (eyes, mouth, genitals) |
| Systemic/organ | None usually | Fever, eosinophilia, hepatitis | Fever, fluid/electrolyte loss |
| Nikolsky sign | Negative (except bullous variant) | Negative | Positive |
| Key culprits | Sulfonamides, NSAIDs, tetracyclines, paracetamol | Anticonvulsants, allopurinol, sulfonamides | Sulfonamides, anticonvulsants, allopurinol, NSAIDs, nevirapine |
SELF-CHECK
A patient on a sulfonamide develops painful skin with flaccid blisters and sheet-like detachment affecting an estimated 18% of body surface area, with oral and ocular erosions. How is this classified?
A. Stevens-Johnson syndrome (SJS), because detachment is less than 10% BSA
B. SJS-TEN overlap, because detachment is between 10% and 30% BSA
C. Toxic epidermal necrolysis (TEN), because detachment is more than 30% BSA
D. Fixed drug eruption, because it is drug-induced
Reveal Answer
Answer: B. SJS-TEN overlap, because detachment is between 10% and 30% BSA
Epidermal detachment of 18% BSA falls in the 10–30% range, which defines SJS-TEN OVERLAP. SJS is less than 10% BSA and TEN is more than 30% BSA — these cut-offs must be applied exactly.