Page 10 of 20
DR12.4 | Cutaneous Adverse Drug Reaction Recognition — SDL Guide (Part 3)
Immediate Recognition and Triage: When to Escalate
Immediate Recognition and Triage of Severe Cutaneous Drug Reactions
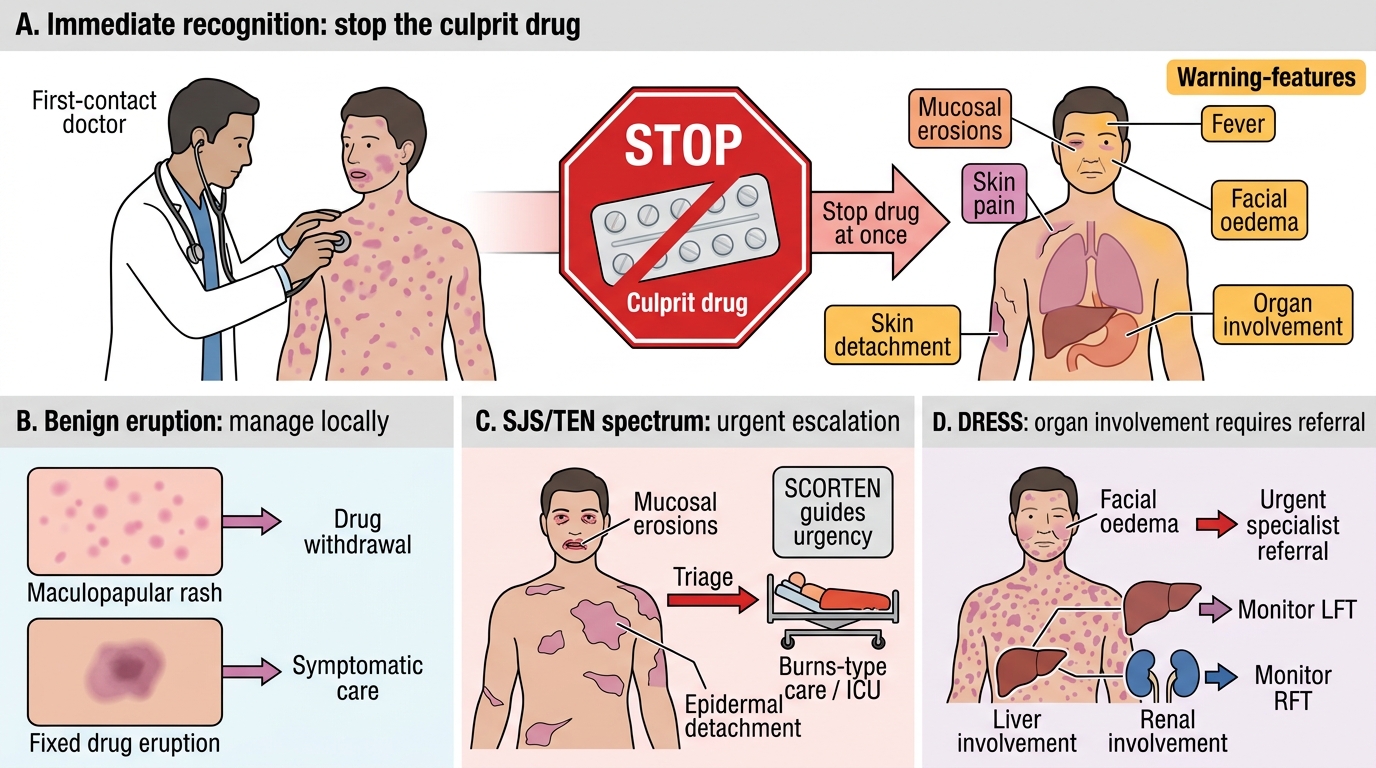
Recognition is only useful if it triggers the right immediate action, and the management thread running through every severe cutaneous drug reaction is the same first step: stop the culprit drug at once, because continuing it worsens the reaction and delaying its withdrawal increases mortality in SJS/TEN. Beyond that, recognition feeds directly into triage. A benign maculopapular rash or a simple fixed drug eruption can be managed with drug withdrawal and symptomatic care; but the moment warning features appear — mucosal erosions, skin pain or detachment, fever, facial oedema, or evidence of organ involvement — the patient must be escalated as a potential severe cutaneous adverse reaction.
For the SJS/TEN spectrum the urgency is greatest: these patients need transfer to a setting equipped for burns-type care, and the SCORTEN score (with referral to a burns unit or intensive care for higher scores) guides how aggressively. For DRESS, the recognition of organ involvement mandates urgent specialist referral and monitoring of liver and renal function. The primary-care or first-contact doctor's role is to recognise the severe reaction, stop the drug, begin supportive measures, and escalate — the detailed definitive management is covered in the companion module on primary care of adverse drug reactions (DR12.5). Early recognition and prompt drug withdrawal are the interventions that most change outcome.
- Universal first step: stop the culprit drug immediately — delay worsens SJS/TEN outcome.
- Escalate when mucosal erosions, skin pain/detachment, fever, facial oedema, or organ involvement are present.
- SJS/TEN: transfer for burns-type care; SCORTEN guides referral to burns unit/ICU.
- DRESS: urgent specialist referral; monitor liver and renal function.
- First-contact role: recognise, stop the drug, support, escalate (definitive care → DR12.5).
Applying the Recognition Framework
Recognition Framework for Drug Reactions
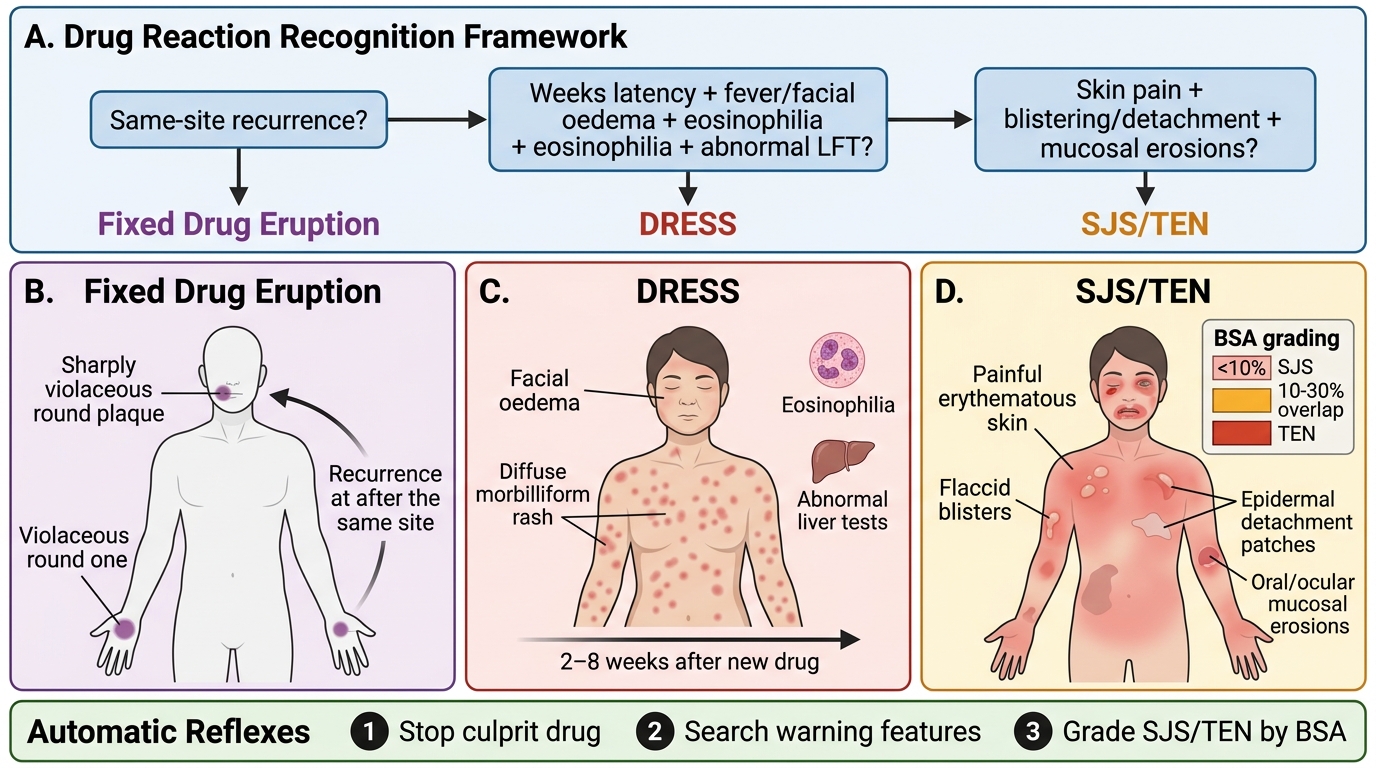
The final task is to apply this framework fluently to real presentations, because in practice these patients do not arrive labelled. Work through the discriminating questions in order: Is the lesion localised and does it recur at the same site (fixed drug eruption)? Is there a several-week latency with fever, facial oedema, eosinophilia and abnormal liver tests (DRESS)? Is there painful skin with blistering, detachment and mucosal erosions, gradable by BSA (SJS/TEN)? Each pattern points to a different diagnosis, a different urgency, and — through the companion module — a different management. The drug history, asking specifically about every new medicine in the preceding weeks, is the thread that ties the diagnosis to its cause.
Three reflexes should now be automatic. First, in any drug reaction, identify and stop the culprit drug. Second, actively search for the warning features that mark a severe reaction — mucosal involvement, systemic/organ features, skin pain or detachment — and never dismiss them. Third, grade SJS/TEN by BSA, using the exact cut-offs, because the grade determines the urgency of transfer. With these, you will reliably separate the benign from the dangerous and act in time.
- Discriminate by signature: same-site recurrence → fixed drug eruption; long latency + eosinophilia + organ involvement → DRESS; painful detachment + mucosal erosions → SJS/TEN.
- Always take a careful drug history of all new medicines in the preceding weeks.
- Reflexes: stop the culprit drug; hunt for warning features; grade SJS/TEN by BSA exactly.
CLINICAL PEARL
Two memory hooks anchor the dangerous reactions. For DRESS, remember it is slow and systemic — it appears two to six weeks after the drug, brings a swollen face and eosinophilia, and damages internal organs (the liver above all); a 'drug rash' weeks after starting carbamazepine or allopurinol with deranged liver enzymes is DRESS until proven otherwise. For SJS/TEN, fix the BSA cut-offs in your mind once and for all: SJS less than 10%, overlap 10–30%, TEN more than 30% — and remember painful skin with mucosal erosions is an emergency, not a viral rash.