Page 1 of 11
DR7.1 | KOH Mount for Superficial Fungal Infection — SDL Guide
Learning Objectives
- List the clinical presentations for which a KOH mount is indicated before starting antifungal therapy
- Explain the principle of potassium hydroxide keratin clearing and assemble the materials required for the test
- Perform the scraping and slide-preparation technique correctly, selecting the active scaly margin and using an appropriate KOH concentration
- Interpret KOH mount findings and distinguish dermatophyte hyphae, Candida, Malassezia, and the mosaic artefact
INSTRUCTIONS
The KOH mount is the single most useful bedside investigation in dermatology — cheap, rapid, and performed with materials available in any clinic. Before you commit a patient to weeks of systemic antifungal therapy, a two-minute KOH examination can confirm fungal infection, distinguish a dermatophyte from Candida, and spare you the cost and risk of treating an eczema or psoriasis as if it were ringworm. This module teaches you to scrape, mount, and read a KOH preparation, and to avoid the false positives and false negatives that trap the unwary.
References
- Neena Khanna. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Fungal Infections / Laboratory Diagnosis (textbook)
- Sacchidanand S et al (eds). IADVL Textbook of Dermatology, 4th ed. Ch: Superficial Fungal Infections and their Laboratory Diagnosis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 30-year-old man comes to your clinic with an itchy, ring-shaped, scaly rash spreading across his groin and inner thighs. The previous doctor prescribed a popular over-the-counter cream containing a potent steroid and an antifungal; the itch settled briefly but the rash has since spread, lost its sharp border, and become harder to recognise. You suspect a fungal infection — but it now looks atypical, and you are about to start him on weeks of oral medication. Before you do, you reach for a scalpel, a glass slide, and a bottle of potassium hydroxide (KOH). Within five minutes, under the microscope, you see long, branching, septate threads marching across the field. The diagnosis is confirmed, the steroid misuse is exposed, and your treatment is now evidence-based rather than a guess.
WHY THIS MATTERS
Superficial fungal infections are among the commonest reasons a patient walks into a dermatology or general clinic in India, and the country is currently living through an epidemic of chronic, recurrent, and treatment-resistant tinea. As a clinician you will be expected to confirm the diagnosis before prescribing — not least because empirical antifungal courses are long, occasionally hepatotoxic, and increasingly undermined by drug resistance. The KOH mount is the skill that lets you do this at the bedside, in real time, without waiting days for a culture. Mastering it means you treat fungal disease when it is truly fungal, withhold antifungals when it is not, and recognise the steroid-modified and mimicking presentations that fool the naked eye. It is a competency you will use on your very first day of clinical practice.
RECALL
Recall from your first-year microbiology that fungi possess a rigid cell wall built largely of chitin and that their cell membranes contain ergosterol rather than the cholesterol of human cells — these two features are exactly what make selective antifungal action and KOH microscopy possible. Recall also the basic structure of the skin: the outermost stratum corneum is composed of dead, keratin-rich corneocytes, and it is this keratin layer that dermatophytes colonise and that KOH dissolves. Finally, recall the difference between true hyphae (septate filamentous fungal growth) and yeast forms (rounded budding cells) — the morphological vocabulary you will now apply directly under the microscope.
When to Reach for the KOH Mount: Clinical Indications
Clinical Indications for KOH Mount
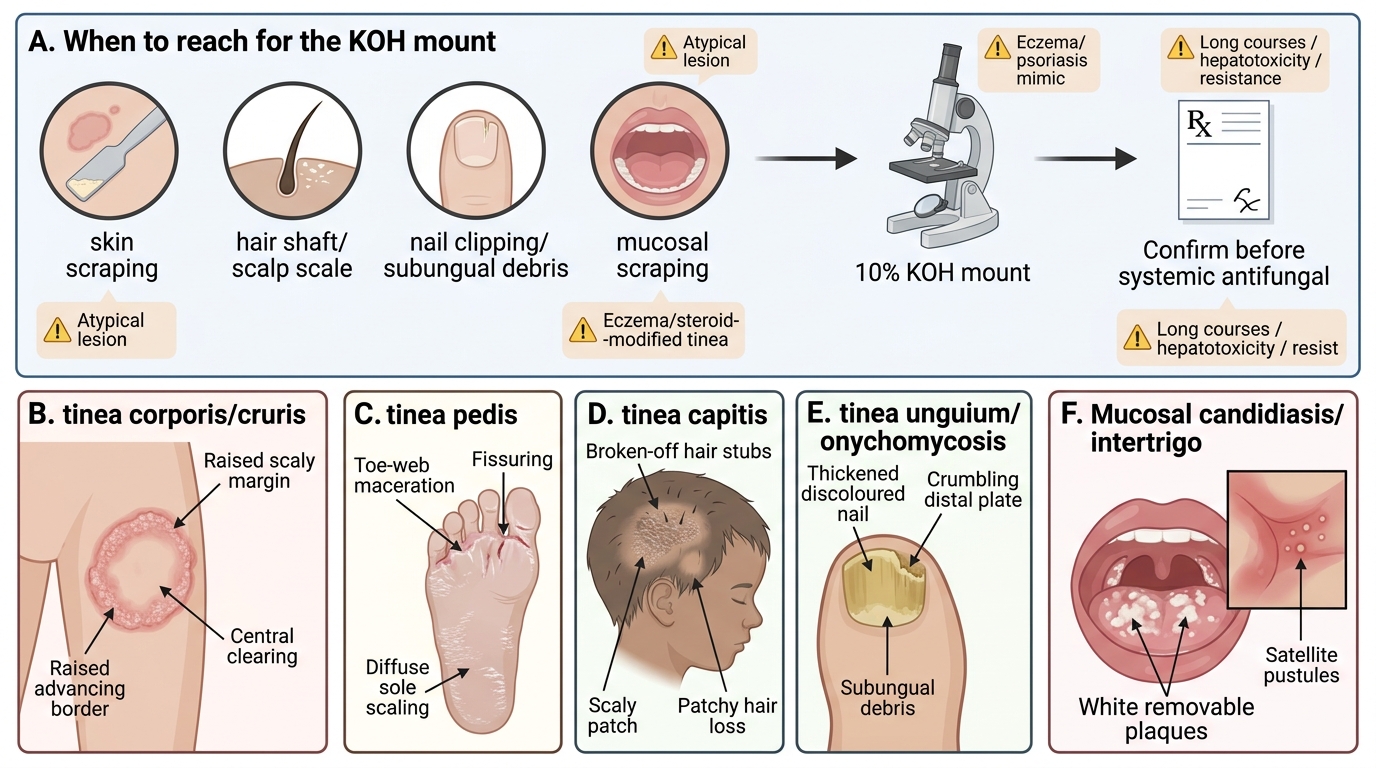
The decision to perform a KOH mount flows directly from clinical pattern recognition: whenever a skin, hair, nail, or mucosal lesion could plausibly be fungal, the KOH mount is the first-line confirmatory test before any systemic antifungal is prescribed. Because antifungal courses are long, occasionally hepatotoxic, and increasingly undermined by resistance, confirming the diagnosis cheaply at the bedside is good clinical economics as well as good medicine. The test is most valuable precisely when the clinical appearance is atypical, modified by prior treatment, or could be confused with a non-fungal disease such as eczema or psoriasis, where an empirical antifungal would waste weeks and mislead both you and the patient. In an Indian clinic, where chronic and recurrent tinea now dominates the dermatology workload, the habit of confirming before treating is what keeps your prescribing rational and your diagnoses honest.
The characteristic presentations that warrant a KOH mount include:
• Tinea corporis/cruris — annular (ring-shaped) scaly plaques with a raised, advancing, scaly margin and central clearing, often itchy.
• Tinea pedis — maceration, peeling, and fissuring of the toe web spaces, or diffuse scaling of the soles.
• Tinea capitis — scaly patches of the scalp with broken-off hair stubs or patchy hair loss, predominantly in children.
• Tinea unguium (onychomycosis) — thickened, discoloured, crumbling nails with subungual debris and onycholysis.
• Cutaneous/mucosal candidiasis — beefy-red intertriginous rash with satellite pustules, or white curd-like plaques on the oral or genital mucosa.
• Pityriasis (tinea) versicolor — hypopigmented or hyperpigmented finely scaly macules over the trunk.
• Steroid-modified (tinea incognito) lesions where the morphology is obscured — here the KOH mount is especially valuable because the eye can no longer be trusted.
Principle of Potassium Hydroxide Clearing and Required Materials
KOH Mount: Selective Clearing Principle and Required Materials
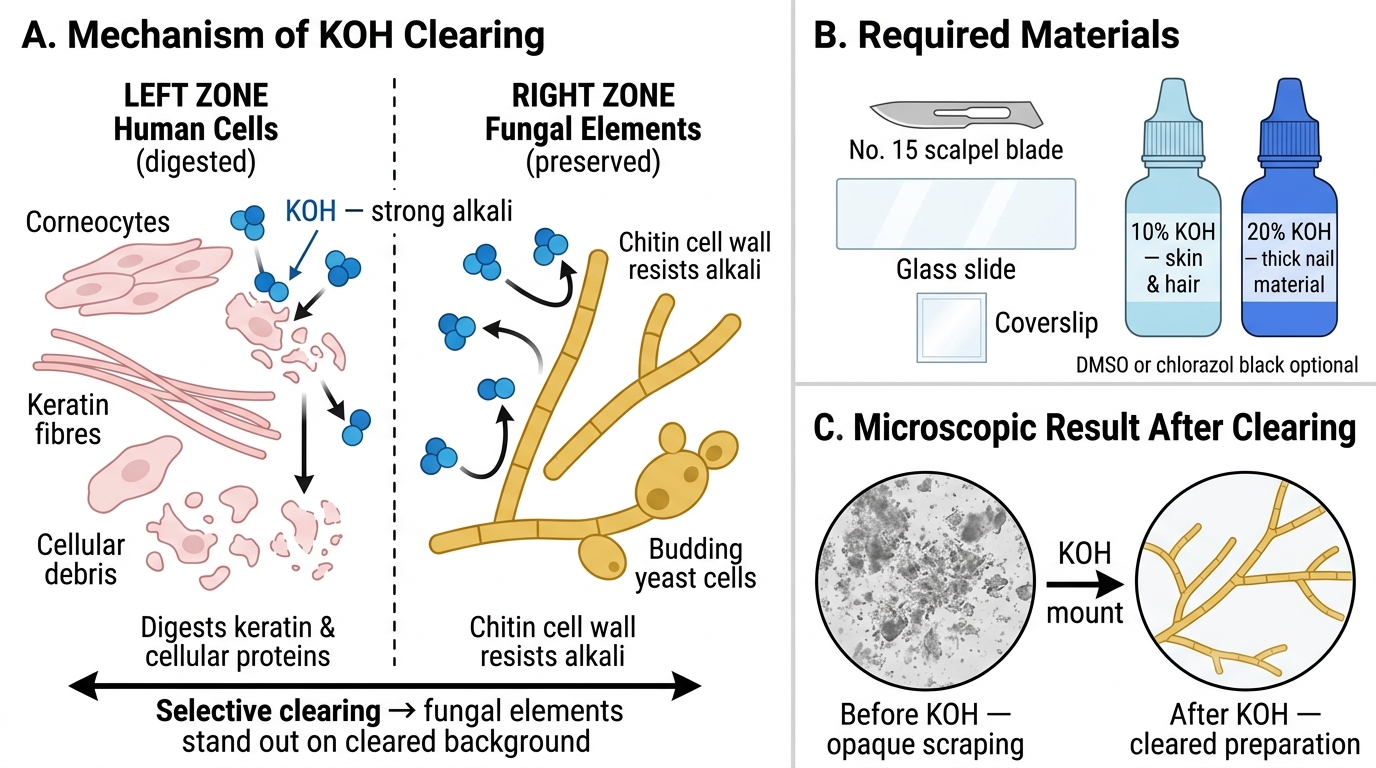
The KOH mount works on a simple chemical principle that exploits the difference between human and fungal cell composition. Potassium hydroxide is a strong alkali that digests keratin and other human cellular proteins, dissolving the dead corneocytes, cellular debris, and intercellular material that would otherwise obscure the field. Crucially, the chitin of the fungal cell wall resists this alkali, so the fungal elements — hyphae and yeasts — remain intact and stand out clearly against a cleared background. This selective clearing is why a few minutes of KOH exposure transforms an opaque skin scraping into a transparent preparation in which fungal threads are visible. Understanding this principle also explains every practical step that follows: why the concentration is higher for tough nail keratin, why gentle warming accelerates clearing, and why overheating ruins the preparation. The materials are deliberately minimal, which is precisely what makes the test deployable in any clinic without a formal laboratory.
The materials required are:
• A No. 15 scalpel blade or the edge of a glass slide / a blunt curette for scraping.
• Clean glass microscope slides and coverslips.
• 10–20% KOH solution (10% for skin and hair; 20% for thick nail material; some labs add DMSO or ink such as chlorazol black or Parker blue-black to speed clearing and improve contrast).
• A spirit lamp or other gentle heat source to accelerate clearing.
• A light microscope with 10× and 40× objectives, used with the condenser lowered and the iris diaphragm partly closed to increase contrast of the unstained elements.
SELF-CHECK
What is the principle by which potassium hydroxide allows fungal elements to be visualised in a skin scraping?
A. KOH stains fungal hyphae a deep blue while leaving human cells unstained
B. KOH digests keratin and human cellular debris while the chitinous fungal cell wall resists it, leaving fungal elements intact against a cleared background
C. KOH selectively kills bacteria so that only fungi remain visible
D. KOH dissolves fungal cell walls, releasing pigment that makes the organism visible
Reveal Answer
Answer: B. KOH digests keratin and human cellular debris while the chitinous fungal cell wall resists it, leaving fungal elements intact against a cleared background
Potassium hydroxide is a strong alkali that dissolves keratin and the dead corneocytes and cellular debris of the skin scraping, clearing the background. The fungal cell wall is composed largely of chitin, which resists alkaline digestion, so hyphae and yeast cells survive intact and become clearly visible against the now-transparent background. KOH does not stain the fungus (added dyes such as chlorazol black do that), does not act on bacteria, and does not dissolve the fungal wall — its whole value lies in selectively clearing human keratin while sparing chitin.
Scraping and Slide Preparation Technique
KOH Mount Sampling and Slide Preparation
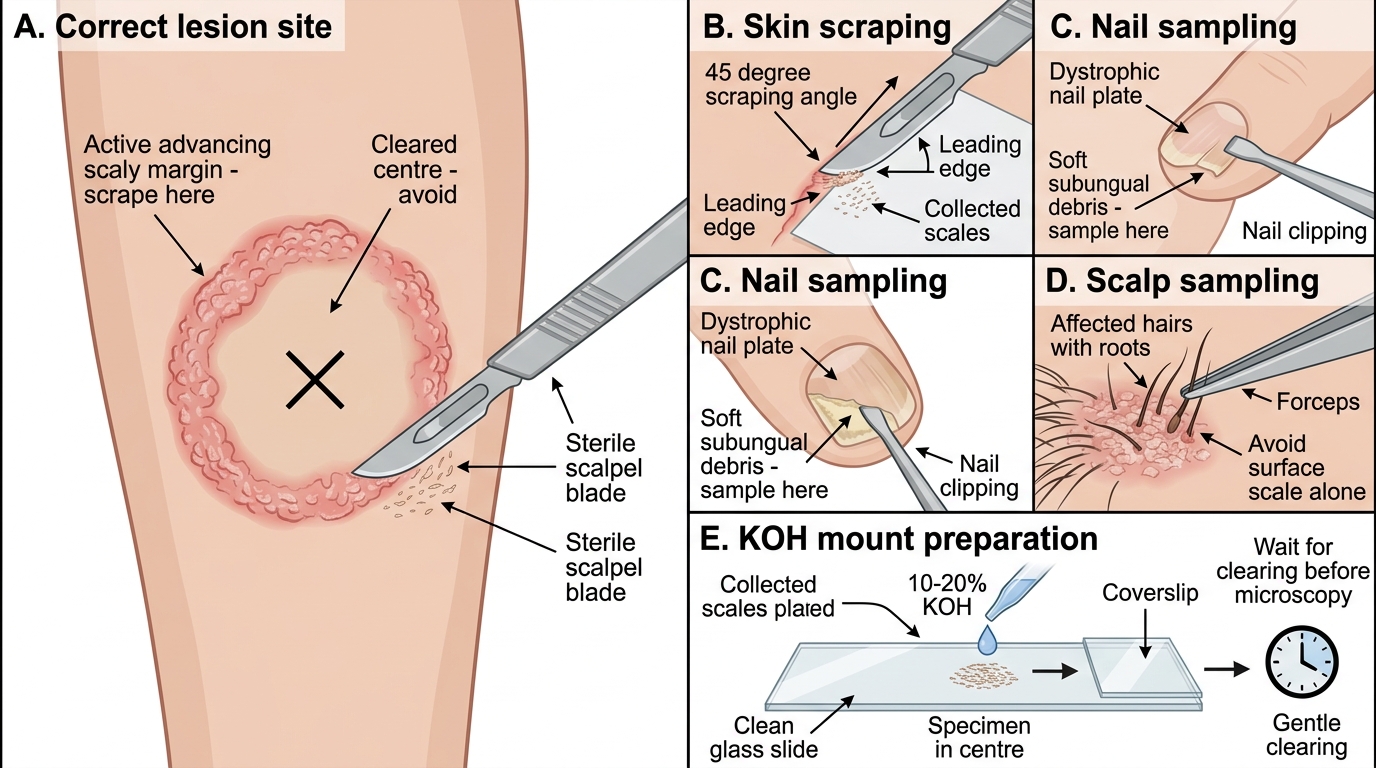
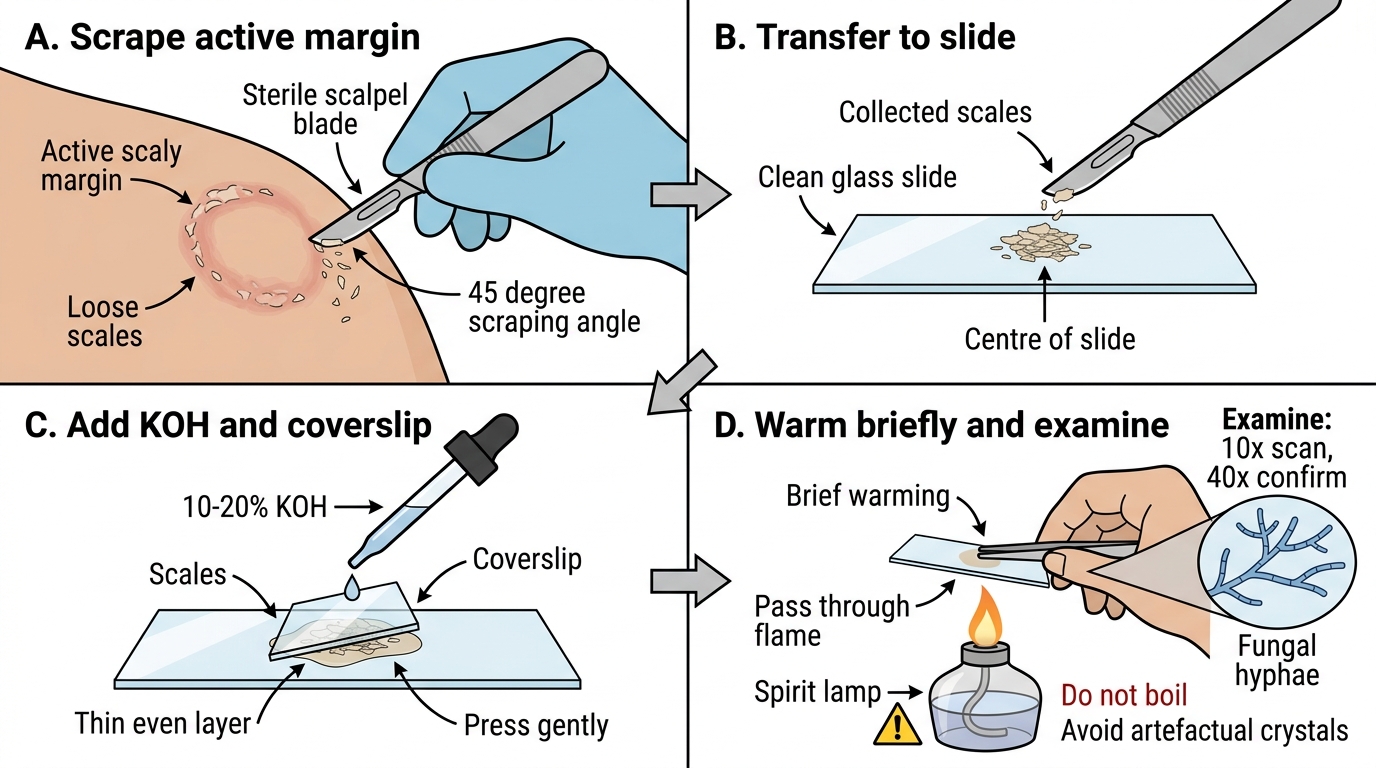
Correct technique is what separates a diagnostic KOH mount from a falsely negative one, and the single most important point is sampling the right part of the lesion. For a typical annular dermatophyte lesion you must scrape the active, advancing scaly margin, where viable fungus is concentrated — the centre of a ring has often already cleared and yields little or no fungus, a classic cause of false-negative results. Clean the area with spirit and let it dry, then hold the scalpel blade roughly perpendicular and scrape the leading edge so that fine scales fall onto a glass slide. The same logic of sampling where the organism actually lives applies to other sites: for nails you must reach the soft subungual debris under the diseased nail plate, and for the scalp you must obtain affected hairs with their roots rather than surface scale alone. Adequate material, gentle clearing, and patience before reading are the other determinants of a usable preparation.
The step-by-step sequence is:
1. Select and gently scrape the active scaly margin (for nails, clip the dystrophic nail and scrape the soft subungual debris from underneath; for scalp, pluck affected hairs with their roots rather than only scraping skin).
KOH Mount Preparation for Superficial Fungal Infection
- Collect the scales onto the centre of a clean slide.
- Add 1–2 drops of 10–20% KOH and apply a coverslip, pressing gently to spread the material into a thin, even layer.
- Warm the slide briefly over a spirit lamp to speed keratin clearing — pass it through the flame; do not boil, as overheating produces artefactual crystals and can destroy the hyphae.
- Wait about 10–15 minutes (longer for nail) for the keratin to clear, then examine under low power (10×) to scan, switching to high power (40×) to confirm and characterise any fungal elements, keeping the light reduced for contrast.