Page 2 of 11
DR7.1 | KOH Mount for Superficial Fungal Infection — SDL Guide (Part 2)
Interpreting the KOH Mount: Dermatophytes, Candida, and Tinea Versicolor
KOH Mount Patterns in Superficial Fungal Infections
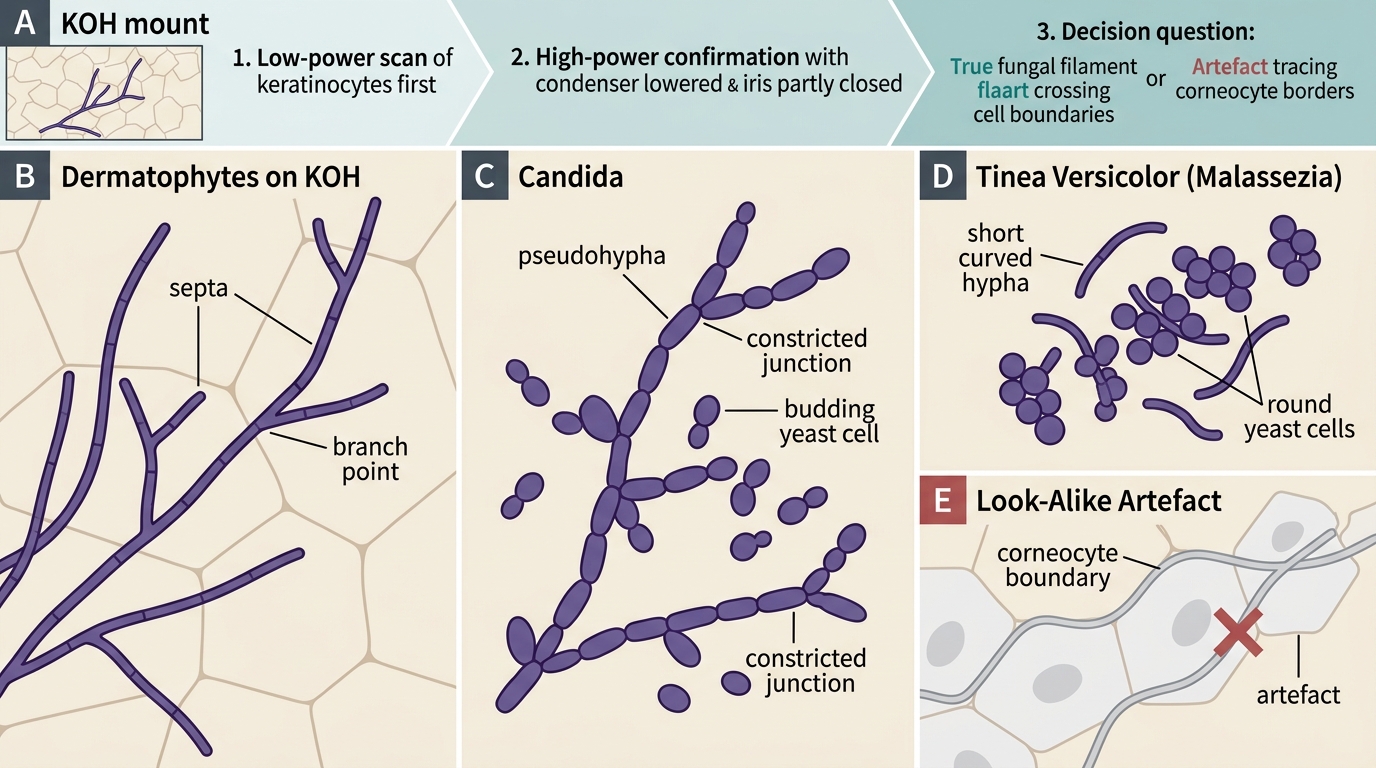
Reading the KOH mount is a matter of recognising a small number of characteristic patterns, and getting these right is the entire diagnostic payoff of the test. The three pathogen groups that cause superficial infection each have a distinctive microscopic signature, and you must also learn to dismiss the common look-alike artefact so that you neither miss disease nor over-diagnose it. Examine systematically at low power first to scan the whole preparation, then confirm any suspicious structure at high power with the condenser lowered and the iris partly closed for contrast. The discipline here is to ask of every filament: is it of uniform calibre, does it branch, and does it cross cell boundaries like a true hypha — or does it merely trace the polygonal outlines of corneocytes like an artefact? Holding that question in mind is what prevents the two opposite errors of missing a real infection and inventing one that is not there.
The characteristic findings are:
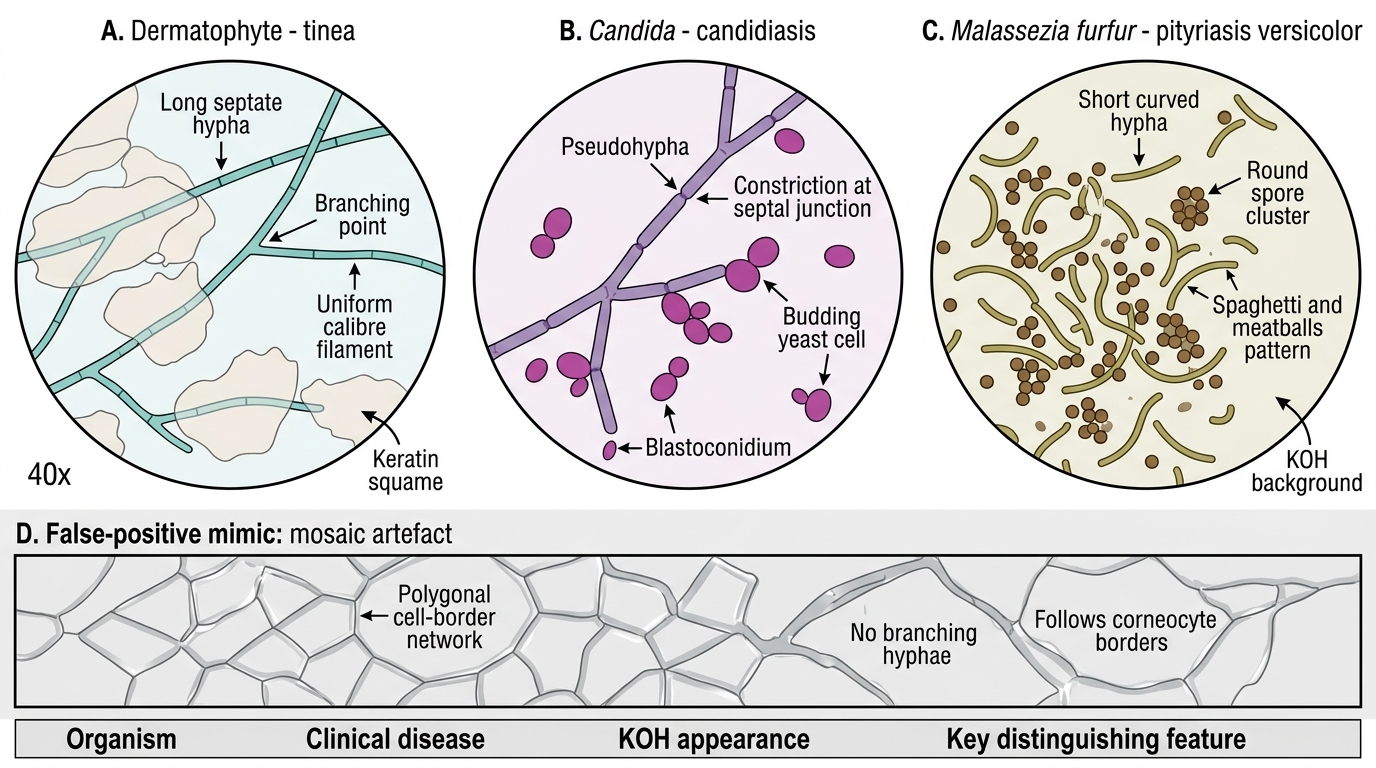
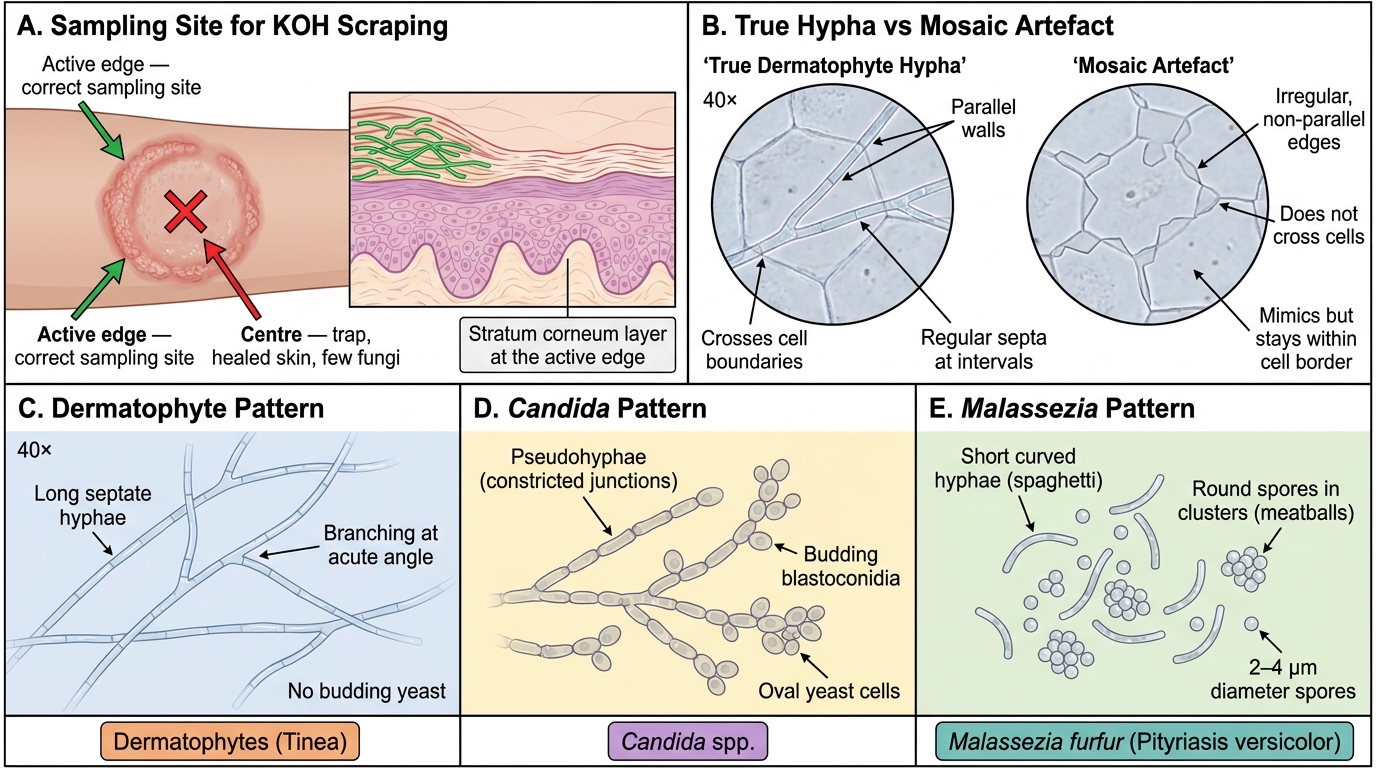
• Dermatophytes (Trichophyton, Microsporum, Epidermophyton — the cause of tinea/ringworm): long, branching, septate hyphae — slender filaments that cross cell boundaries, branch, and show regular cross-walls (septa). This is the single most important pattern to recognise.
• Candida: pseudohyphae together with budding yeast cells (blastoconidia) — chains of elongated yeast cells constricted at their junctions, accompanied by small oval budding forms; the absence of true regular septate branching hyphae helps distinguish it from a dermatophyte.
• Malassezia furfur (pityriasis/tinea versicolor): short, curved (stubby) hyphae mixed with clusters of round yeast spores — the classic "spaghetti and meatballs" appearance.
• Mosaic artefact (the key false positive to exclude): a refractile, geometric, polygonal network outlining the edges of corneocytes, produced by cholesterol/cell-wall debris; unlike true hyphae it does not branch, is not of uniform calibre, and lies along cell borders rather than crossing them.
KOH Mount Findings in Superficial Fungal Infections
| Organism | Clinical disease | KOH appearance | Key distinguishing feature |
|---|---|---|---|
| Dermatophytes | Tinea (corporis/cruris/pedis/capitis/unguium) | Long septate branching hyphae | Uniform-calibre filaments crossing cell boundaries |
| Candida | Cutaneous/mucosal candidiasis | Pseudohyphae + budding yeast | Constrictions at junctions; budding blastoconidia |
| Malassezia furfur | Pityriasis versicolor | Short curved hyphae + round spores | "Spaghetti and meatballs" |
| Mosaic artefact (false +) | None — artefact | Refractile polygonal network on cell borders | No branching; follows corneocyte outlines |
SELF-CHECK
A KOH mount taken from the active scaly margin of an itchy annular groin lesion shows long, branching, septate hyphae. Which organism does this represent?
A. Candida albicans
B. A dermatophyte (e.g. Trichophyton)
C. Malassezia furfur
D. Staphylococcus aureus
Reveal Answer
Answer: B. A dermatophyte (e.g. Trichophyton)
Long, branching, septate hyphae are the hallmark of a dermatophyte infection (tinea) — here, tinea cruris, most often caused by Trichophyton species in India. Candida shows pseudohyphae together with budding yeast cells rather than true uniform septate branching hyphae. Malassezia furfur shows short curved hyphae with clustered round spores (the "spaghetti and meatballs" pattern). Bacteria such as Staphylococcus aureus are not visualised on a KOH mount, which clears keratin to reveal fungal elements specifically.
Applied Practice: Common Pitfalls and Correlating KOH with Clinical Diagnosis
Using KOH Mount Wisely in Suspected Fungal Infection
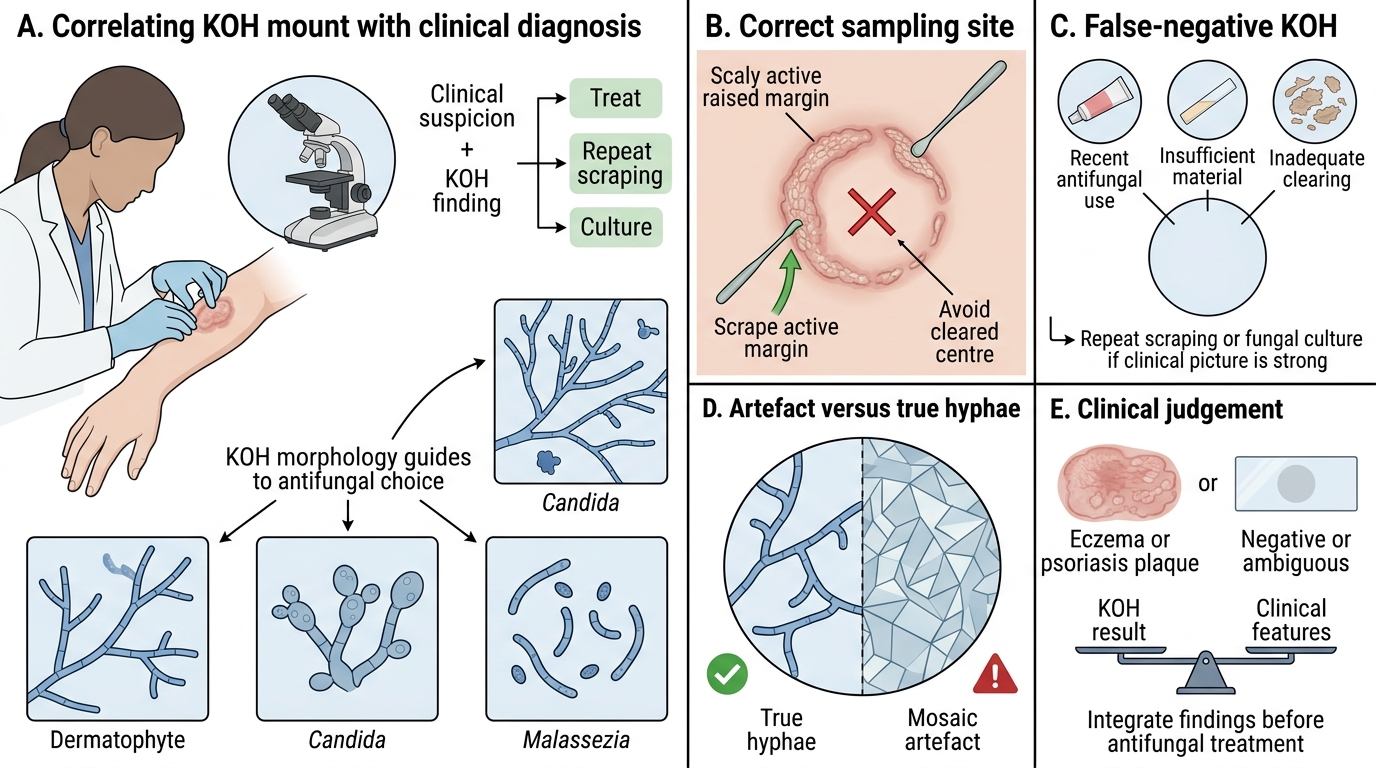
Applying the KOH mount well in practice means correlating what you see down the microscope with the clinical picture, and being honest about the test's limitations. A positive KOH confirms a fungal infection and, with the morphology, points you toward dermatophyte versus Candida versus Malassezia — directly shaping your choice of antifungal. A negative KOH, however, does not exclude fungal infection: false negatives are common and usually reflect a correctable sampling or technique error, so a confident clinical picture with a negative KOH should prompt a repeat scraping or a fungal culture rather than abandoning the diagnosis. The reverse error is equally important to guard against — over-reading a mosaic artefact as hyphae and committing a patient with eczema or psoriasis to a needless antifungal course. Treating the KOH result as one input into a clinical judgement, rather than an infallible verdict, is the mark of a clinician who uses the test wisely.
The pitfalls to anticipate are:
• Wrong sampling site — scraping the cleared centre instead of the active margin; the commonest cause of a false negative.
• Recent antifungal use — even brief topical treatment can render the KOH negative while the lesion is still fungal.
• Insufficient material or inadequate clearing — too few scales, or examining before keratin has cleared.
• Mosaic artefact mistaken for hyphae — the geometric, refractile, non-branching network of cholesterol/cell-wall debris that follows corneocyte borders; the key false positive to exclude.
• Tinea capitis — a negative skin scraping does not rule it out; affected hairs must be plucked and examined (and a culture or Wood's lamp considered).
A note on the Wood's lamp, a useful adjunct rather than a substitute for the KOH mount: in tinea capitis it produces a green fluorescence with Microsporum species, but it does NOT fluoresce with Trichophyton — which is the predominant cause of tinea capitis in India — so a non-fluorescent scalp lesion does not exclude tinea. For recalcitrant, chronic, or recurrent dermatophytosis, send a fungal culture for species identification, because treatment-resistant tinea linked to terbinafine resistance is now a major problem in India and culture (with sensitivity where available) guides drug choice.
Self-Assessment: KOH Mount Skill Check
KOH Mount Skill Check: Sampling, Artefact Recognition, and Microscopic Patterns
Before moving on, consolidate the skill by testing yourself against the situations you will actually meet in clinic, because procedural competence is demonstrated not by reciting steps but by making correct decisions when a lesion is in front of you. Work through each of the prompts below, committing to an answer before you reveal the reasoning, and pay particular attention to the points that most commonly go wrong: choosing the sampling site, selecting the KOH concentration, attaching the right pathogen to each microscopic pattern, and separating a true hypha from the mosaic artefact. If any answer is uncertain, return to the relevant section above rather than guessing, since the cost of a wrong KOH decision in practice is either a missed infection or an unnecessary drug course.
- Sampling: From which part of an annular tinea lesion should you scrape, and why is the centre a trap?
- Concentration and heat: What KOH strength would you use for a thick toenail, and why must you avoid boiling the slide?
- Pattern recognition: Match each finding — long branching septate hyphae; pseudohyphae with budding yeast; short curved hyphae with round spores — to its organism.
- Artefact: State two features that distinguish a true dermatophyte hypha from a mosaic artefact.
- Adjuncts: In suspected tinea capitis, what does a green Wood's lamp fluorescence tell you, and why does its absence not exclude the diagnosis in India?
SELF-CHECK
A KOH mount from a macerated toe-web lesion is reported as negative, but the clinical picture strongly suggests tinea pedis. What is the single most appropriate next step?
A. Conclude the lesion is not fungal and treat as eczema
B. Repeat the scraping from the active scaly area (ensuring no recent antifungal use and adequate clearing), and send a fungal culture if doubt persists
C. Start a 12-week course of oral terbinafine empirically without further testing
D. Immediately diagnose Candida and prescribe oral fluconazole
Reveal Answer
Answer: B. Repeat the scraping from the active scaly area (ensuring no recent antifungal use and adequate clearing), and send a fungal culture if doubt persists
A negative KOH mount does not exclude a fungal infection — false negatives are common and usually reflect a correctable error such as sampling the wrong site, recent antifungal use, insufficient material, or inadequate clearing time. With a clinically convincing tinea pedis, the correct response is to repeat the scraping from an appropriate active site after confirming no recent antifungal use and allowing adequate clearing, and to send a fungal culture if doubt persists, rather than abandoning the diagnosis, committing to a long empirical systemic course blindly, or jumping to an unsupported Candida diagnosis.
CLINICAL PEARL
Always scrape the active edge, never the centre. The single most common reason a clinically obvious ringworm gives a "negative" KOH is that the sample was taken from the cleared centre of the lesion rather than its raised, advancing scaly margin where viable fungus lives. If the clinical picture strongly suggests tinea but the KOH is negative, do not discard the diagnosis — repeat the scraping from the margin, ensure no antifungal has been used recently, allow adequate clearing time, and send a fungal culture if doubt persists. And never mistake the geometric, non-branching mosaic artefact for true hyphae: real dermatophyte hyphae are of uniform calibre, branch, and cross cell boundaries.