Page 4 of 11
DR7.2 | Superficial Fungal Infection Management — SDL Guide
Learning Objectives
- Recognise the morphology and distribution of dermatophytoses, candidiasis, and pityriasis versicolor
- Explain the etiopathogenesis of superficial fungal infections and the host factors driving the current Indian epidemic of chronic tinea
- Construct a site-specific differential diagnosis and select appropriate confirmatory investigations
- Formulate resistance-aware topical and systemic management for superficial fungal infections, including recalcitrant terbinafine-resistant tinea
INSTRUCTIONS
Superficial fungal infection is one of the commonest presentations in Indian dermatology, and the country is in the grip of an epidemic of chronic, recurrent, and treatment-resistant tinea. Managing it well means more than reaching for an antifungal cream — it means confirming the diagnosis, recognising the steroid-modified and mimicking presentations, choosing topical versus systemic therapy rationally by site and organism, and responding correctly when terbinafine fails. This module equips you to manage a case of fungal infection from recognition through investigation to a resistance-aware treatment plan.
References
- Neena Khanna. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Fungal Infections (textbook)
- Sacchidanand S et al (eds). IADVL Textbook of Dermatology, 4th ed. Ch: Superficial Fungal Infections / Management of Dermatophytosis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 35-year-old farmer returns to your clinic for the fourth time in eight months. The itchy, scaly rash that began in his groin has now spread to his abdomen, buttocks, and thighs in broad, poorly-defined plaques. He has used several over-the-counter creams — most of them containing a potent steroid — and each time the itch eased before the rash flared worse. A previous course of oral terbinafine for a full month barely helped. His wife and son have similar lesions. This is not a simple ringworm: it is the face of India's epidemic of chronic dermatophytosis, where steroid misuse, household spread, and rising drug resistance have turned a once-trivial infection into a frustrating, relapsing disease. Managing him well demands a systematic approach — confirm, investigate, and treat with the resistance problem firmly in mind.
WHY THIS MATTERS
You will see superficial fungal infections on your very first day of clinical practice, and in India you will see them constantly — often in their difficult, chronic, steroid-modified, and treatment-resistant forms. Getting the management right matters because the wrong approach has real consequences: an unconfirmed diagnosis wastes weeks of therapy on the wrong disease; a topical steroid-antifungal combination cream eases itch while spreading the infection; and an automatic month of terbinafine now frequently fails because of resistance. Knowing how to confirm the diagnosis, when to choose systemic over topical therapy, how long to treat each site, and what to do when terbinafine fails is core clinical competence. It also positions you to counter the steroid-misuse and irrational-prescribing practices that drive much of the current epidemic.
RECALL
Recall from the companion skills SDL on the KOH mount that dermatophytes show long, branching, septate hyphae while Candida shows pseudohyphae with budding yeast — the bedside confirmation that should precede systemic antifungal therapy. Recall from your microbiology and pharmacology foundations that the fungal cell membrane depends on ergosterol, and that antifungals act at different points in its synthesis: allylamines such as terbinafine inhibit squalene epoxidase, while azoles such as itraconazole and fluconazole inhibit lanosterol 14-α-demethylase (CYP51). Understanding these targets explains both how the drugs work and how mutations in the squalene epoxidase gene produce the terbinafine resistance now seen across India.
Recognising Superficial Fungal Infections: Morphology and Distribution Patterns
Morphology and Distribution of Superficial Fungal Infections
The first step in managing a fungal infection is recognising it, and recognition rests on reading the morphology and the site together, because the same dermatophyte produces a different clinical picture depending on the body region it colonises. Classical dermatophytosis presents as an annular (ring-shaped) lesion with a raised, scaly, advancing margin and relative central clearing — but in India this textbook picture is increasingly distorted by steroid misuse into broad, ill-defined, widespread plaques. Learning to name the infection by its site is the foundation, because site largely dictates whether topical therapy will suffice or systemic treatment is mandatory. You should also be able to separate dermatophyte disease from candidiasis and pityriasis versicolor on appearance, since each is managed differently.
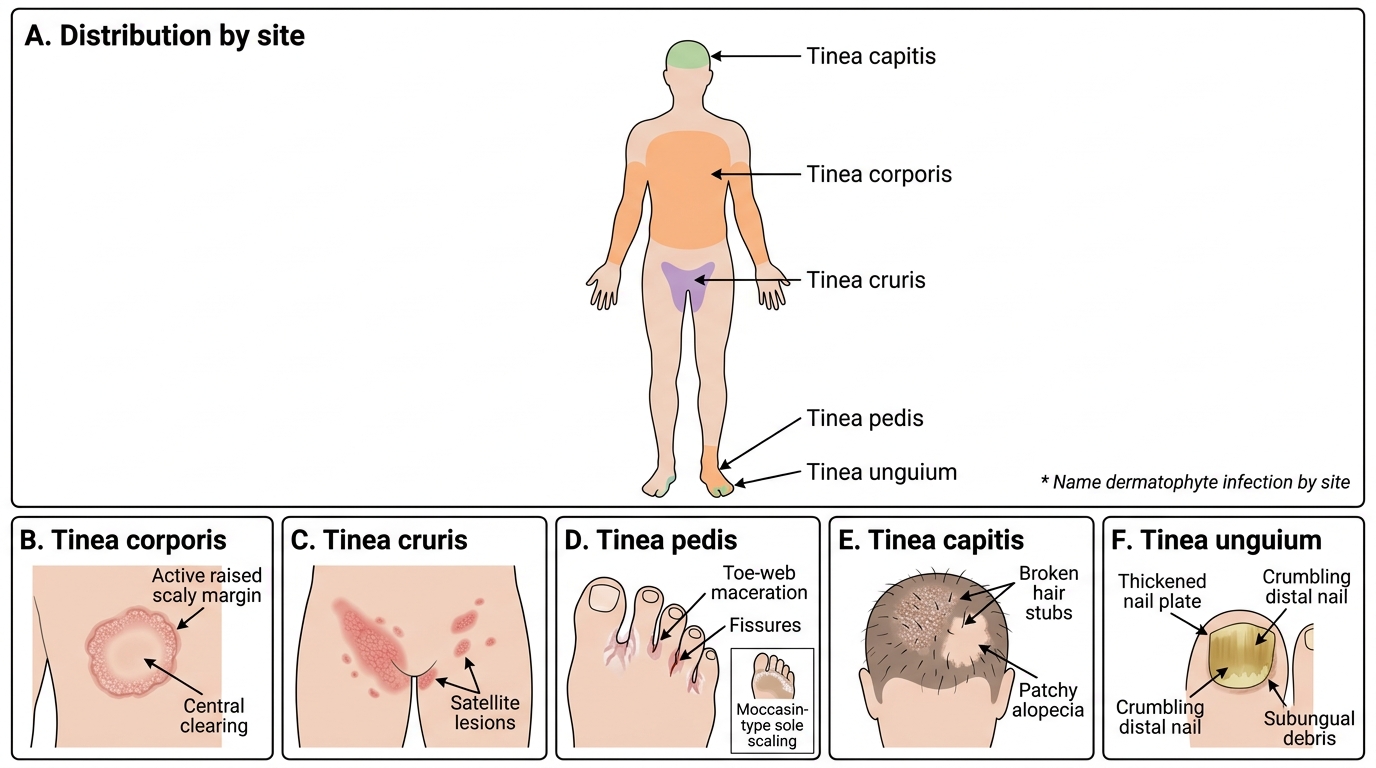
The characteristic patterns are:
• Tinea corporis — annular scaly plaque with an active raised margin and central clearing on the trunk or limbs.
• Tinea cruris — erythematous scaly plaques in the groin and inner thighs, often with satellite lesions; common in hot, humid conditions.
• Tinea pedis — maceration, peeling, and fissuring of the toe web spaces, or diffuse "moccasin" scaling of the soles.
• Tinea capitis — scaly scalp patches with broken hair stubs or patchy alopecia, predominantly in children.
• Tinea unguium (onychomycosis) — thickened, discoloured, crumbling nails with subungual debris and onycholysis.
• Cutaneous candidiasis — beefy-red intertriginous rash with satellite pustules; oral/genital candidiasis shows white curd-like plaques.
• Pityriasis versicolor — hypopigmented or hyperpigmented finely scaly macules over the trunk and shoulders.
Etiopathogenesis: Why Fungi Establish and How Host Factors Drive Severity
Etiopathogenesis of Superficial Fungal Infections
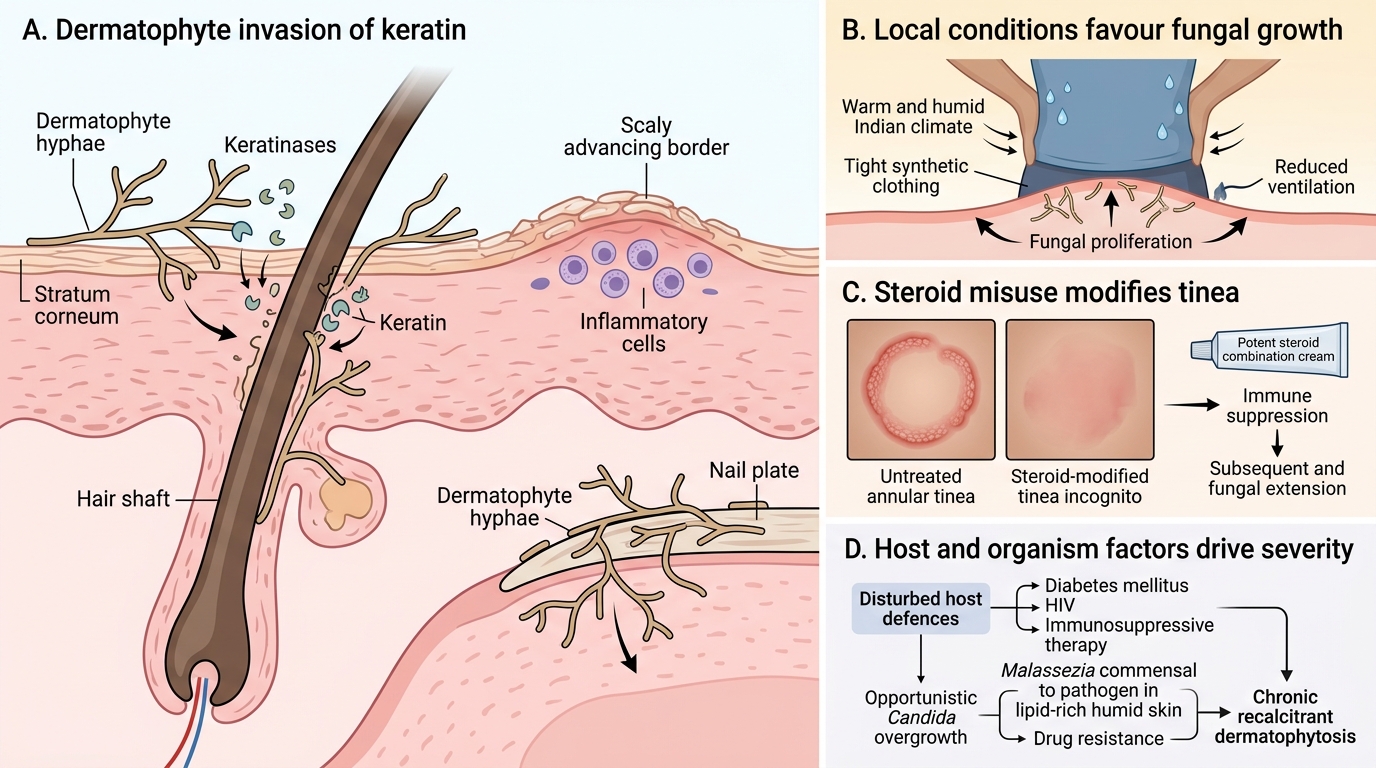
Understanding why these fungi establish and persist explains both the clinical picture and the modern Indian problem of chronic, recalcitrant disease. Dermatophytes are keratinophilic fungi that secrete keratinases to digest and invade the keratin of the stratum corneum, hair, and nail, provoking a host inflammatory response that produces the raised, scaly, advancing margin. They thrive in warmth, humidity, occlusion, and sweat — conditions abundant in the Indian climate and exaggerated by tight synthetic clothing. Candida, by contrast, is an opportunist that overgrows when local or systemic host defences are disturbed, while Malassezia is a skin commensal that converts to a pathogen under favourable lipid and humidity conditions. What has transformed dermatophytosis from a trivial to an epidemic disease in India is the convergence of several host and drug factors, foremost among them the rampant misuse of potent topical corticosteroid combination creams and the emergence of drug resistance.
The key contributory factors are:
• Climate and occlusion — heat, humidity, sweating, and tight clothing favour dermatophyte growth.
• Topical corticosteroid misuse — potent steroid-antifungal-antibacterial combination creams suppress inflammation, modify the morphology (tinea incognito), and allow the fungus to spread widely.
• Host immunosuppression — diabetes mellitus, HIV, and immunosuppressive therapy predispose to extensive and candidal infection.
• Household and community spread — shared clothing, towels, and close contact perpetuate familial clusters.
• Rising terbinafine resistance — mutations in the squalene epoxidase (SQLE) gene of Trichophyton (notably the T. mentagrophytes/indotineae complex) underlie the chronic, recurrent, terbinafine-unresponsive tinea now widespread in India; itraconazole has consequently become the commonly used agent for such cases.
SELF-CHECK
Which mechanism best explains the rising terbinafine resistance seen in chronic dermatophytosis in India?
A. Mutations in the lanosterol 14-α-demethylase (CYP51) gene reducing azole binding
B. Mutations in the squalene epoxidase (SQLE) gene reducing terbinafine binding
C. Acquired loss of the fungal chitin cell wall
D. Increased ergosterol synthesis driven by topical antibacterials
Reveal Answer
Answer: B. Mutations in the squalene epoxidase (SQLE) gene reducing terbinafine binding
Terbinafine is an allylamine that acts by inhibiting the fungal enzyme squalene epoxidase. Point mutations in the squalene epoxidase (SQLE) gene — well documented in the Trichophyton mentagrophytes/indotineae complex now widespread in India — reduce the drug's binding to its target and produce clinical terbinafine resistance, contributing to chronic, recurrent, treatment-unresponsive tinea. CYP51 mutations affect azole binding (not terbinafine); the chitinous cell wall is not lost; and the resistance is a target-enzyme mutation rather than a consequence of antibacterial-driven ergosterol synthesis. Because of this resistance, itraconazole (a triazole) has become the commonly used agent for recalcitrant disease.
Clinical Features and Diagnosis: Site-Specific Patterns and KOH Confirmation
Clinical Diagnosis of Superficial Fungal Infections
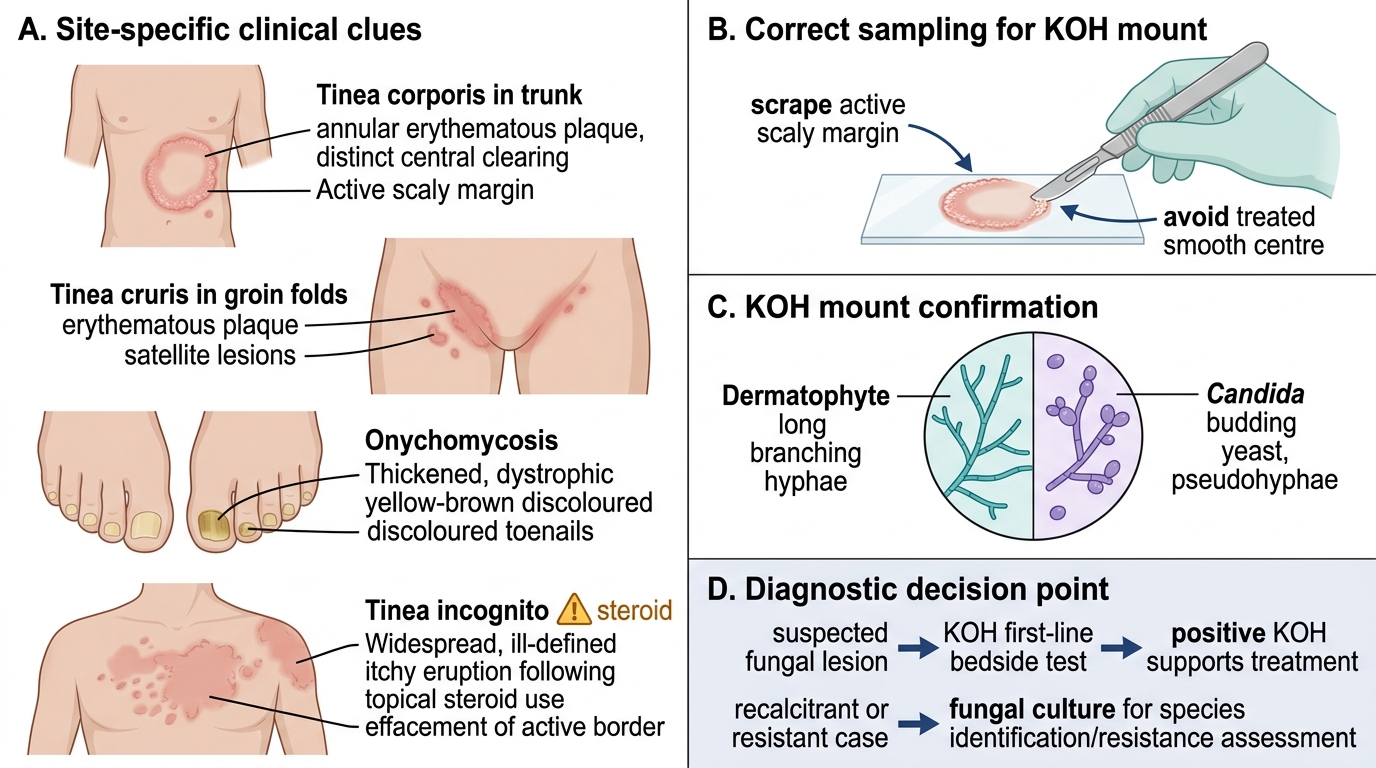
Accurate diagnosis combines reading the site-specific clinical features with bedside confirmation, and the cardinal rule is to confirm fungal infection before committing a patient to weeks of systemic therapy. Each site has features that both suggest the diagnosis and warn of mimics: an annular plaque with an active margin suggests tinea corporis, groin involvement with satellite lesions suggests tinea cruris, and dystrophic discoloured nails suggest onychomycosis — but the Indian reality of widespread steroid use means many lesions arrive as tinea incognito, with the diagnostic active border effaced and the disease spread far beyond its original site. The KOH mount is therefore the essential first-line confirmatory test, demonstrating septate branching hyphae and distinguishing dermatophyte from Candida; a fungal culture is reserved for recalcitrant cases needing species identification or resistance assessment. A correct diagnosis at this stage is what makes the entire management plan rational.
Key diagnostic points by situation:
• KOH mount — first-line bedside confirmation; scrape the active scaly margin, examine for long branching septate hyphae (dermatophyte) versus pseudohyphae with budding yeast (Candida).
• Tinea incognito — suspect when a chronic, widespread, ill-defined, itchy eruption follows topical steroid use; the active border is lost but the KOH remains positive.
• Onychomycosis — examine all nails; distal-lateral subungual onychomycosis (DLSO) is the commonest pattern; confirm by KOH/culture of subungual debris before long systemic therapy.
• Wood's lamp — an adjunct in tinea capitis: green fluorescence occurs with Microsporum but NOT with Trichophyton, which is the predominant Indian cause, so absence of fluorescence does not exclude the diagnosis.
• Fungal culture — reserved for recalcitrant, recurrent, or diagnostically uncertain cases, and where species identification or resistance information will change management.