Page 5 of 11
DR7.2 | Superficial Fungal Infection Management — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Differential Diagnosis and Investigations in Superficial Fungal Infection
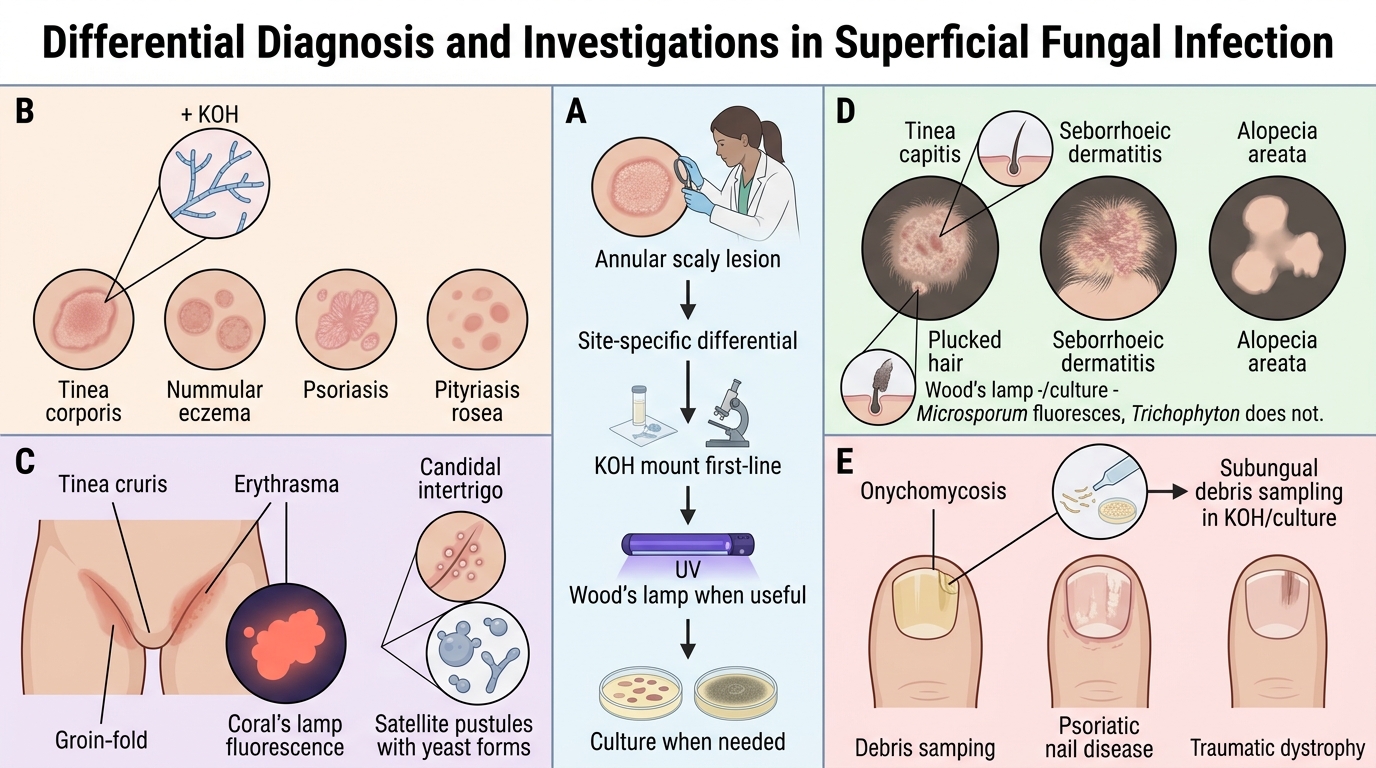
Because several common dermatoses mimic superficial fungal infection, building a site-specific differential and choosing the right investigations prevents the frequent error of treating an eczema or psoriasis as tinea (and vice versa). The clinical overlap is real: nummular eczema, psoriasis, and pityriasis rosea can all resemble tinea corporis; erythrasma and intertrigo mimic tinea cruris; seborrhoeic dermatitis and alopecia areata mimic tinea capitis; and psoriatic or traumatic nail changes mimic onychomycosis. The discriminating tool in most cases is the KOH mount, supported where needed by the Wood's lamp and culture. Working through the differential explicitly, rather than assuming every annular scaly lesion is fungal, is what keeps your prescribing accurate in a setting where both fungal infection and its mimics are common.
Differentials and investigations by site:
• Tinea corporis vs nummular eczema, psoriasis, pityriasis rosea — KOH positive in tinea; eczema/psoriasis KOH-negative with their own clinical features.
• Tinea cruris vs erythrasma (coral-red fluorescence on Wood's lamp, due to Corynebacterium) vs candidal intertrigo (satellite pustules, KOH shows yeast).
• Tinea capitis vs seborrhoeic dermatitis, alopecia areata — KOH/culture of plucked hairs; Wood's lamp (Microsporum fluoresces, Trichophyton does not).
• Onychomycosis vs psoriatic nail (pitting, oil-drop sign) vs traumatic dystrophy — KOH and culture of subungual debris; dermoscopy may help.
• Investigations overall — KOH mount (first-line), fungal culture (speciation/resistance in recalcitrant cases), Wood's lamp (adjunct), and dermoscopy for nail and scalp assessment.
Management: Topical, Systemic, and Resistance-Aware Prescribing
Provided image
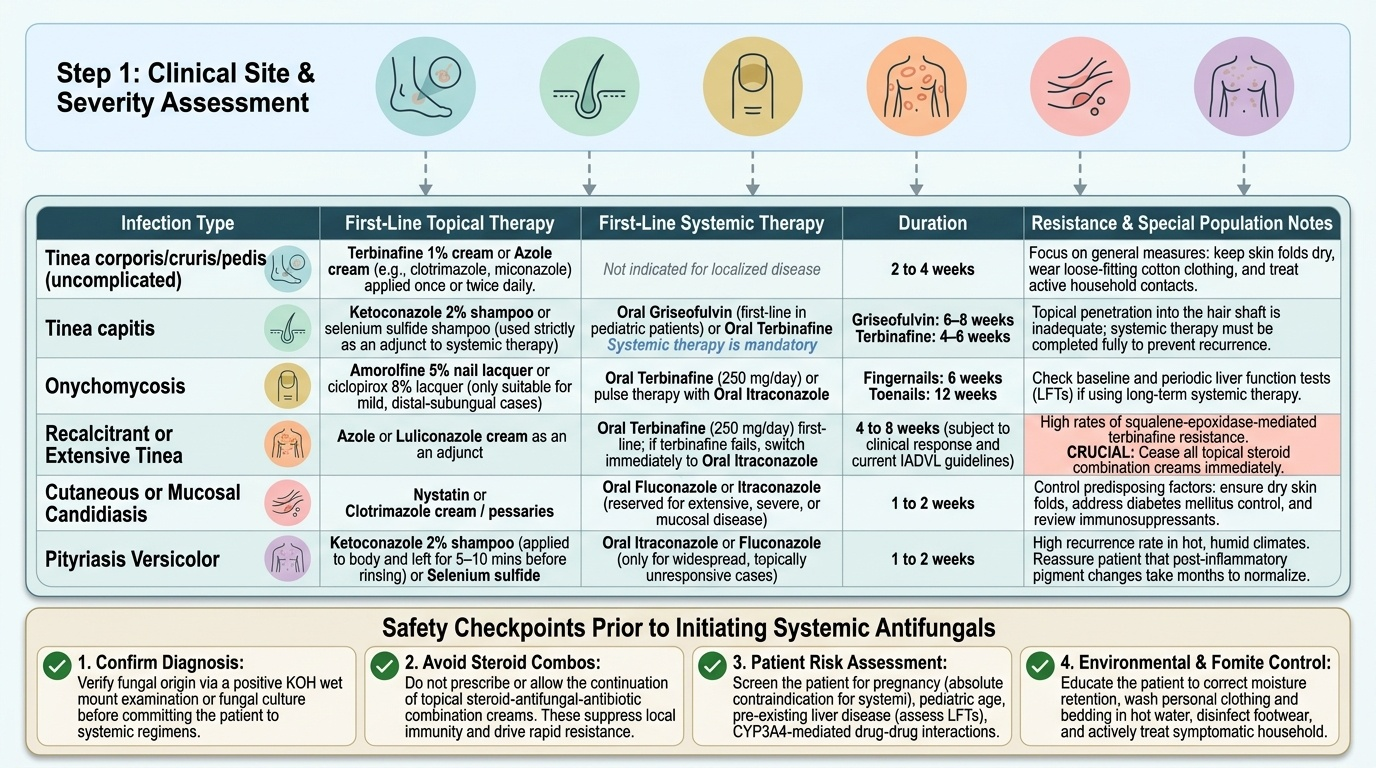
Rational management of superficial fungal infection is organised by infection type, extent, and site, and in the current Indian context it must be explicitly resistance-aware. The guiding principles are: confirm the diagnosis first; use topical antifungals for localised, uncomplicated disease; escalate to systemic antifungals for extensive, recurrent, hair-bearing, or nail disease where topical penetration is inadequate; treat for an adequate duration; address predisposing factors and household contacts; and — crucially — stop the topical steroid combination creams that drive spread and resistance. When first-line oral terbinafine fails in chronic or recurrent dermatophytosis, the now-standard response is to switch to itraconazole, reflecting the squalene-epoxidase-mediated terbinafine resistance widespread across the country. The plan below states drug choice and duration by infection type, but durations should be confirmed against current IADVL guidance for the individual patient.
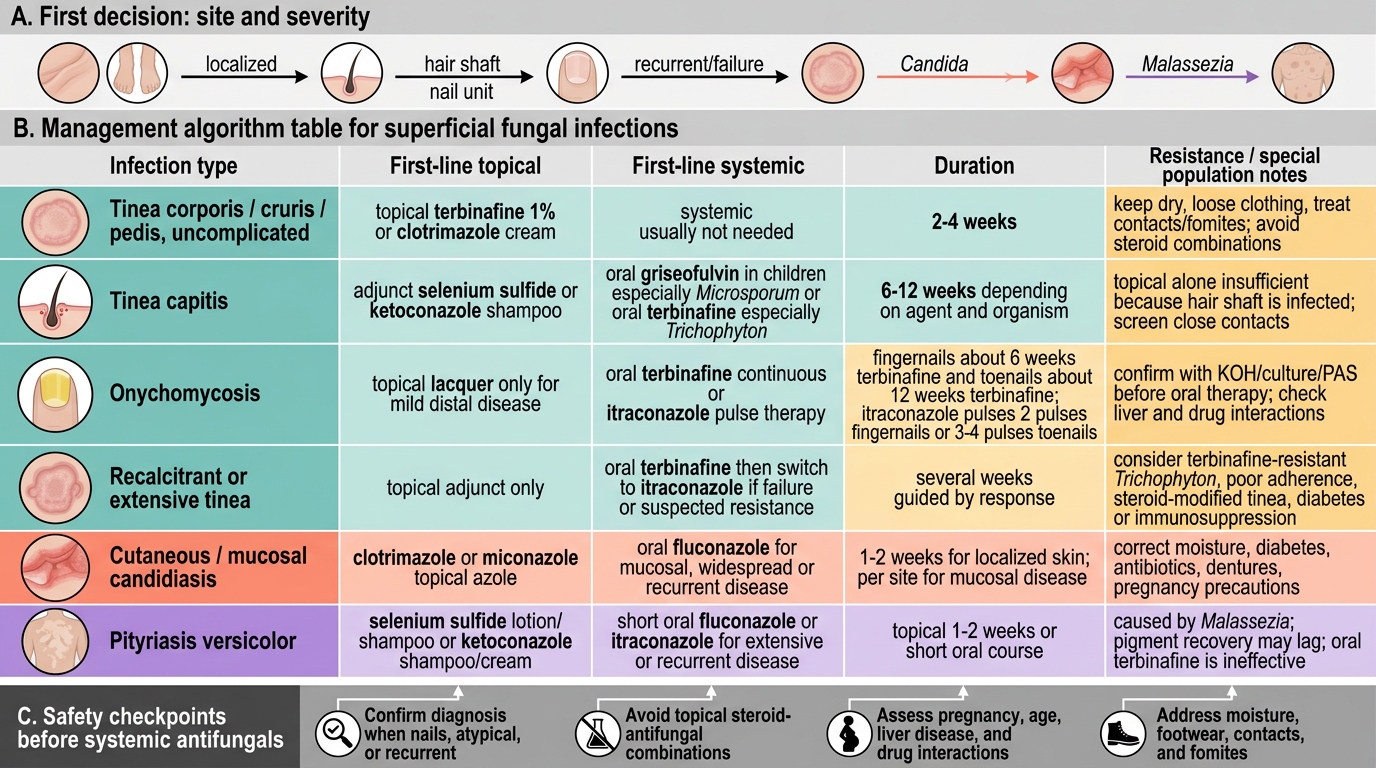
Management of Superficial Fungal Infections
- Tinea corporis/cruris/pedis (localised) — topical terbinafine or an azole (e.g. clotrimazole) cream for ~2–4 weeks; general measures (keep dry, loose clothing, treat contacts).
- Tinea corporis/cruris (extensive or recurrent) — oral terbinafine 250 mg/day for several weeks; if it fails, switch to itraconazole for recalcitrant terbinafine-resistant disease.
- Tinea capitis — systemic therapy is mandatory (topical alone is insufficient in the hair shaft): oral griseofulvin (first-line in children, especially for Microsporum) or terbinafine, with an adjunct antifungal shampoo; treat for several weeks per guideline.
- Onychomycosis — systemic therapy required: oral terbinafine continuous, or itraconazole pulse therapy; toenails need longer treatment than fingernails — confirm exact durations against current guidance.
- Cutaneous/mucosal candidiasis — topical azole (clotrimazole/miconazole) for localised disease; oral fluconazole for mucosal or widespread infection; correct predisposing factors.
- Pityriasis versicolor — topical selenium sulfide or ketoconazole (shampoo/cream); a short oral azole course (e.g. fluconazole or itraconazole) for extensive/recurrent disease.
| Drug | Class | Mechanism | Spectrum | Indian use note |
|---|---|---|---|---|
| Terbinafine | Allylamine | Inhibits squalene epoxidase | Dermatophytes (cidal) | First-line for tinea; rising resistance |
| Itraconazole | Triazole | Inhibits CYP51 | Dermatophytes, Candida, Malassezia | Now common for recalcitrant tinea |
| Fluconazole | Triazole | Inhibits CYP51 | Candida (primary), some dermatophytes | Mainstay for candidiasis |
| Griseofulvin | — | Disrupts fungal microtubules | Dermatophytes | First-line tinea capitis in children |
| Clotrimazole/Ketoconazole | Topical azole | Inhibits CYP51 | Broad superficial | Topical for localised disease |
SELF-CHECK
A 22-year-old man has extensive tinea corporis that has not responded to 4 weeks of oral terbinafine 250 mg/day. A KOH mount confirms septate branching hyphae. What is the most appropriate next step?
A. Add a potent topical corticosteroid combination cream to settle the inflammation
B. Switch to oral itraconazole, considering terbinafine-resistant dermatophytosis, and reinforce general/contact measures
C. Stop all antifungals as the diagnosis must be wrong
D. Repeat the identical terbinafine course for another 4 weeks
Reveal Answer
Answer: B. Switch to oral itraconazole, considering terbinafine-resistant dermatophytosis, and reinforce general/contact measures
A KOH-confirmed dermatophytosis that fails an adequate course of oral terbinafine in the current Indian setting should raise terbinafine resistance (squalene epoxidase mutations in the T. mentagrophytes/indotineae complex). The appropriate response is to switch to oral itraconazole, which has become the commonly used agent for recalcitrant terbinafine-resistant tinea, while reinforcing general measures, treating household contacts, and stopping steroid-containing creams. Adding a potent steroid combination cream would worsen and spread the infection (tinea incognito); the diagnosis is confirmed by KOH so it is not wrong; and simply repeating the failed terbinafine course ignores the likely resistance.
Self-Assessment: Fungal Infection Management
Fungal Infection Management: Route, Resistance, and Duration
Consolidate your management skill by reasoning through the decisions you will actually make in clinic, because competence in managing fungal infection is demonstrated by correct drug-and-duration choices, not by listing antifungals. Test yourself against the situations below, deciding in each case whether topical or systemic therapy is indicated, which agent and duration you would choose, and how the Indian resistance problem changes your plan. Pay special attention to the high-yield decision points that examiners and real patients both probe: the mandatory systemic treatment of tinea capitis, the long durations needed for onychomycosis, the recognition of steroid-modified tinea incognito, and the switch from terbinafine to itraconazole when first-line treatment fails. Where you are unsure of an exact duration, note that it should be confirmed against current IADVL guidance rather than recalled approximately.
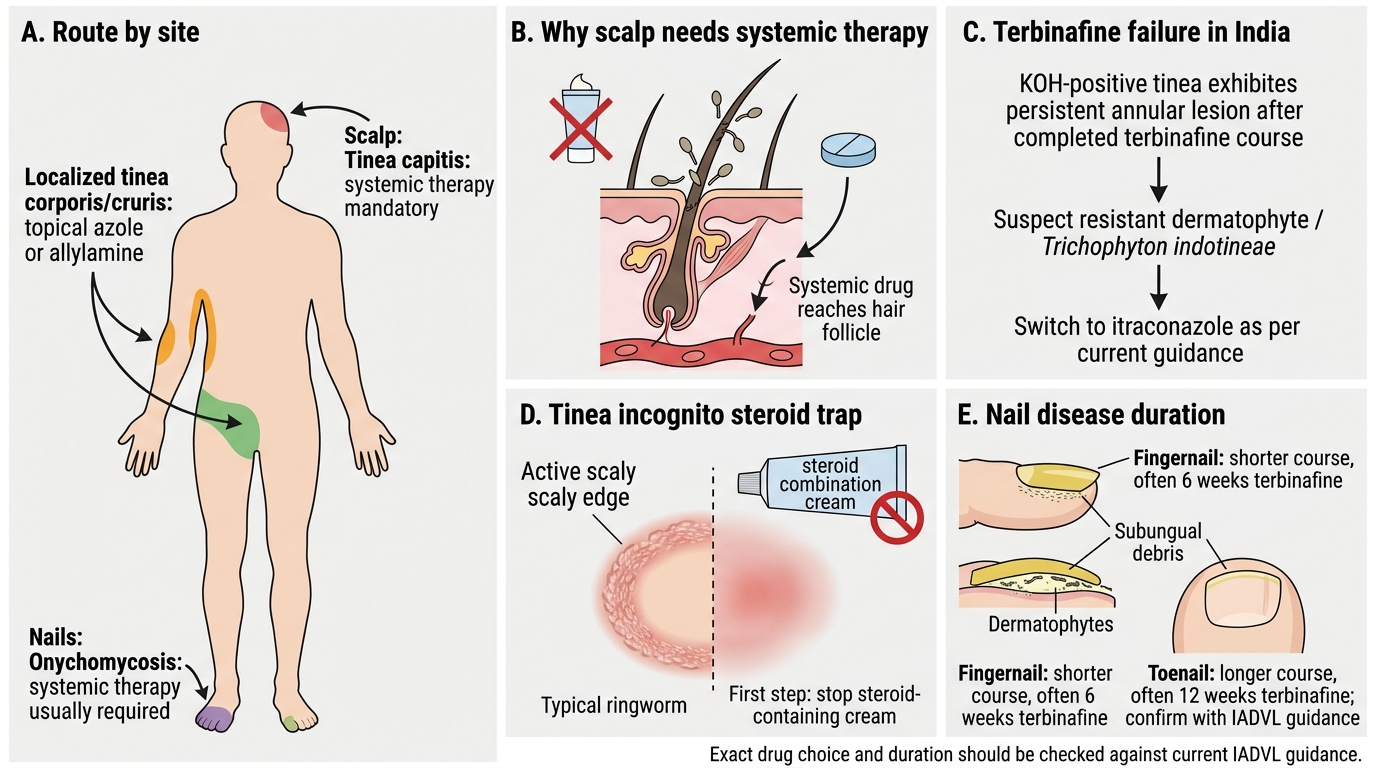
- Site dictates route: Why can tinea capitis never be treated with topical antifungals alone, and what is the first-line systemic drug in a child?
- Resistance response: A KOH-confirmed tinea fails a full course of terbinafine — what is your next drug and why?
- Steroid trap: How would you recognise tinea incognito, and what is the first management step regarding the patient's current cream?
- Nail disease: Why does onychomycosis require systemic therapy, and how does toenail treatment differ from fingernail treatment?
- Right drug for the organism: Which oral antifungal is the mainstay for mucosal candidiasis, and which is first-line for tinea capitis in children?
SELF-CHECK
Regarding the treatment of tinea capitis in a child, which statement is correct?
A. A topical antifungal cream applied to the scalp is sufficient for cure
B. Systemic antifungal therapy (e.g. oral griseofulvin or terbinafine) is mandatory because topical agents cannot reach the fungus within the hair shaft
C. Oral fluconazole is the established first-line agent for all tinea capitis
D. No treatment is needed as tinea capitis resolves spontaneously at puberty
Reveal Answer
Answer: B. Systemic antifungal therapy (e.g. oral griseofulvin or terbinafine) is mandatory because topical agents cannot reach the fungus within the hair shaft
Tinea capitis involves the hair shaft, which topical antifungals cannot adequately penetrate, so systemic therapy is mandatory for cure — oral griseofulvin is the classic first-line agent in children (particularly effective for Microsporum), and oral terbinafine is also widely used (especially for Trichophyton species), usually with an adjunct antifungal shampoo to reduce shedding. A topical cream alone will not cure it; fluconazole is the mainstay for candidiasis rather than the established universal first-line for tinea capitis; and while some endothrix infections may improve around puberty, relying on spontaneous resolution risks scarring alopecia and ongoing transmission and is not acceptable management.
CLINICAL PEARL
When terbinafine fails a KOH-confirmed tinea, think resistance and switch to itraconazole — and always stop the steroid cream. India is living through an epidemic of chronic, recurrent dermatophytosis driven by squalene-epoxidase-mediated terbinafine resistance and by rampant misuse of potent topical steroid-antifungal combination creams. The combination cream is the patient's enemy disguised as a friend: it eases the itch while spreading the infection and producing tinea incognito. The two reflexes that most improve outcomes are switching the failed terbinafine to itraconazole for recalcitrant disease and treating the whole household and environment to break the cycle of reinfection.