Page 1 of 23
DR9.1 | Leprosy Epidemiology Classification and Clinical Features — SDL Guide
Learning Objectives
- Describe the global and Indian epidemiology of leprosy and the goals of the National Leprosy Eradication Programme (NLEP)
- Identify the three cardinal signs used by WHO to diagnose leprosy
- Describe the Ridley-Jopling immunological spectrum (TT, BT, BB, BL, LL, Indeterminate) by clinical, bacteriological, and histological features
- Apply the WHO operational classification (paucibacillary vs multibacillary) and explain how it differs from the Ridley-Jopling spectrum and why it guides multidrug therapy
INSTRUCTIONS
Leprosy remains a disease of major public-health and personal consequence in India, which still reports the largest number of new cases of any country in the world. A clinician who recognises the disease early, classifies it correctly, and starts the right treatment can prevent the nerve damage, deformity, and lifelong stigma that follow late diagnosis. This module builds the diagnostic foundation for the rest of the leprosy cluster: it teaches you to recognise the disease at the bedside, to place a patient on the Ridley-Jopling immunological spectrum, and — separately — to assign the WHO operational class that determines which multidrug-therapy regimen the patient receives. Keeping these two classification systems distinct is the single most important conceptual skill in leprosy care.
References
- Neena Khanna. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Leprosy (textbook)
- IADVL Textbook of Dermatology, 4th ed. Section: Leprosy — Classification and Clinical Features (textbook)
- National Leprosy Eradication Programme (NLEP) Operational Guidelines, Government of India; WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy 2018 (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old farmer comes to your outpatient clinic worried about a single pale patch on his forearm that he first noticed eight months ago. It does not itch, it does not hurt — in fact, he tells you almost as an afterthought, he cannot feel a cigarette ember or hot tea spilled on that exact patch of skin. He has been to two practitioners who treated him for a fungal infection with creams that did nothing. As you examine him, you notice the patch is well-defined, hypopigmented, and dry, and when you test it with a wisp of cotton he genuinely cannot feel your touch over the lesion while feeling it perfectly on the surrounding skin. You palpate behind his elbow and feel a thickened, cord-like ulnar nerve. In that moment, two cardinal signs of leprosy have already declared themselves. The diagnosis this man has been missing for eight months is one of the most treatable — and most stigmatised — diseases in medicine, and how you classify it in the next ten minutes determines whether he receives six months or twelve months of therapy.
WHY THIS MATTERS
Leprosy is not a disease of the past in India. India accounts for more new leprosy cases each year than any other country, and as a future clinician — whether in a primary health centre, a district hospital, or a dermatology clinic — you will encounter undiagnosed cases. The cost of missing or mis-classifying leprosy is measured in irreversible nerve damage, visible deformity, and the profound social stigma that still attaches to this disease. Correct early diagnosis and classification directly determine the treatment regimen, the duration of therapy, the intensity of follow-up, and the patient's risk of disability. Every later skill in this cluster — neurological examination, slit-skin smear, reaction management, multidrug therapy, and disability counselling — depends on the classification you make first. This is foundational clinical reasoning you will use throughout your career.
RECALL
Before beginning, recall from Microbiology that the causative organism, Mycobacterium leprae, is an obligate intracellular acid-fast bacillus that cannot be cultured on artificial media, multiplies very slowly (generation time ~12-14 days), prefers cooler body temperatures (which explains its predilection for skin, peripheral nerves, eyes, and testes), and has a unique tropism for Schwann cells of peripheral nerves. Recall from Immunology the axis of cell-mediated immunity (the TH1 response, mediating granuloma formation and bacillary killing) versus the predominantly humoral TH2 response. As you will see, it is the strength of a patient's cell-mediated immunity against M. leprae that determines where they fall on the disease spectrum — from the high-immunity tuberculoid pole to the low-immunity lepromatous pole.
Recognising Leprosy — Morphology and Cardinal Signs
Recognising Leprosy: Cardinal Signs and Morphology
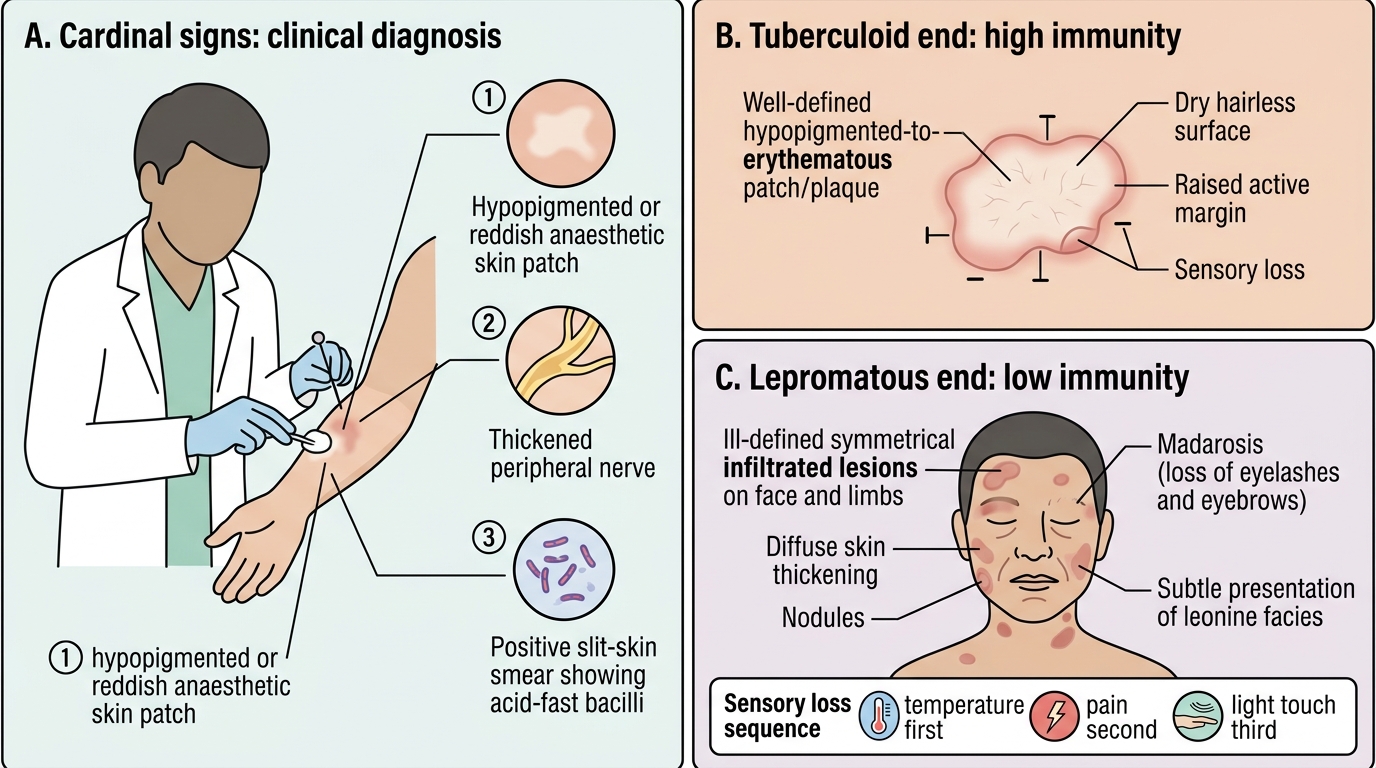
Leprosy presents to the clinician primarily through the skin and the peripheral nerves, and the diagnosis is fundamentally clinical. The World Health Organization defines three cardinal signs, and the presence of any ONE of them establishes the diagnosis of leprosy: (1) a hypopigmented or reddish skin patch with definite loss of sensation; (2) a thickened or enlarged peripheral nerve, with or without tenderness; and (3) a positive slit-skin smear demonstrating acid-fast bacilli. The genius of this definition is that it allows diagnosis at the most peripheral health facility without any laboratory beyond a skin smear, and the anaesthetic skin patch alone — confirmed by sensory testing — is enough to begin treatment.
The skin lesions of leprosy vary along the disease spectrum, and learning to read their morphology is the first diagnostic step. At the high-immunity (tuberculoid) end, lesions are few — often a single, well-defined, hypopigmented or erythematous patch or plaque with a dry, hairless, anaesthetic surface and a raised active margin. At the low-immunity (lepromatous) end, lesions are numerous, ill-defined, symmetrically distributed, and infiltrated, producing diffuse thickening of the skin, nodules, loss of eyebrows (madarosis), and in advanced disease the characteristic leonine facies. Sensory loss within lesions follows a sequence: temperature sensation is lost first, then pain, then light touch.
Ridley-Jopling Spectrum of Leprosy
Key points to anchor before moving on:
- The diagnosis requires any one of the three cardinal signs — anaesthetic patch, thickened nerve, or positive smear.
- Sensory loss over a skin lesion is the most specific bedside clue and distinguishes leprosy from common mimics like tinea or vitiligo.
- Nerve thickening can be felt even when the overlying skin looks normal.
SELF-CHECK
A patient presents with a single hypopigmented patch. Which single finding, by itself, is sufficient to satisfy a WHO cardinal sign and support a clinical diagnosis of leprosy?
A. Itching over the patch
B. Definite loss of sensation (anaesthesia) demonstrable over the patch
C. A positive family history of leprosy
D. A KOH mount negative for fungal hyphae
Reveal Answer
Answer: B. Definite loss of sensation (anaesthesia) demonstrable over the patch
One of the three WHO cardinal signs is a hypopigmented or reddish skin patch with DEFINITE loss of sensation. Demonstrable anaesthesia over the lesion is the single most specific bedside finding and, on its own, satisfies a cardinal sign sufficient to diagnose leprosy. Itching argues AGAINST leprosy (lesions are typically asymptomatic). Family history and a negative KOH are supportive context but are not cardinal signs. The other two cardinal signs are a thickened peripheral nerve and a positive slit-skin smear.
Mycobacterium leprae and the Immunological Basis of Disease
Immunological Spectrum of Leprosy
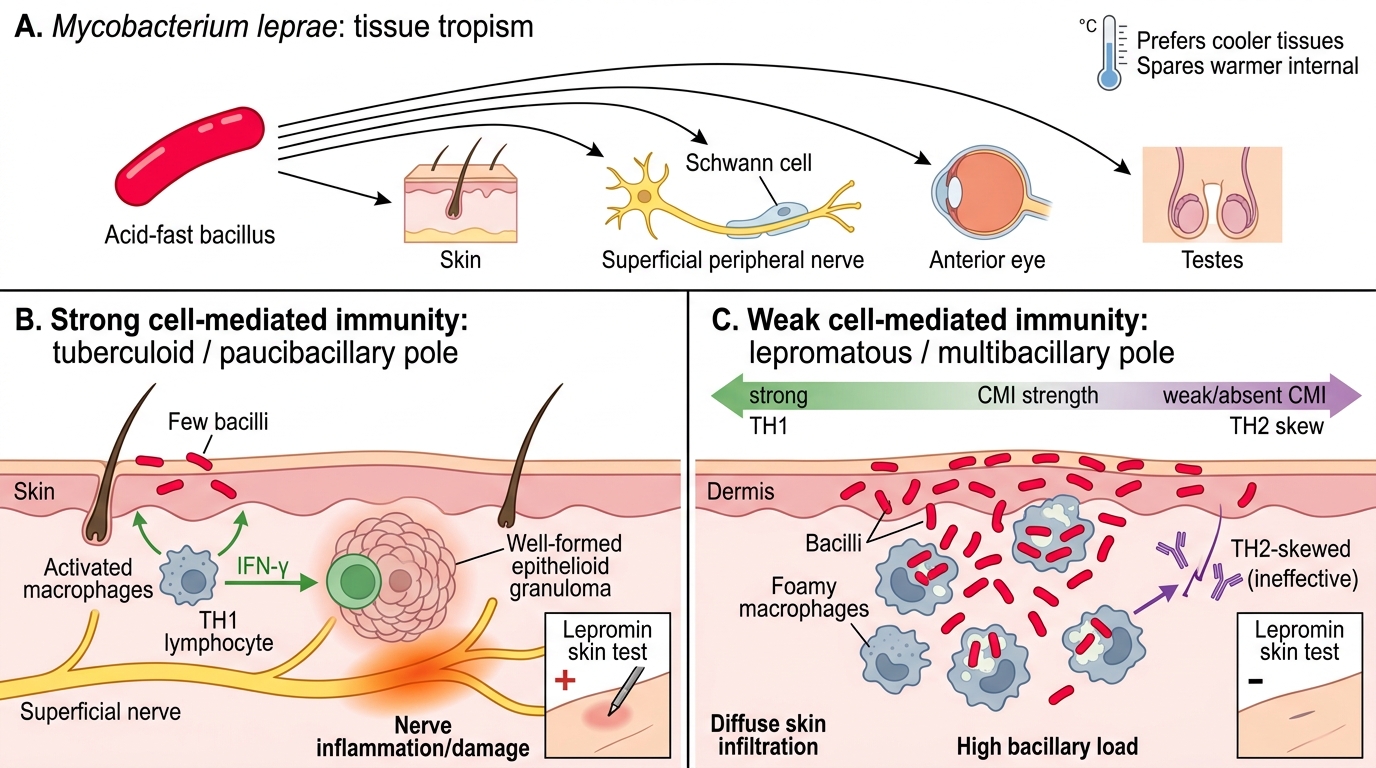
The remarkable clinical diversity of leprosy — from a single trivial-looking patch to widespread disfiguring infiltration — is explained almost entirely by the host's immune response rather than by differences in the organism itself. Mycobacterium leprae is an obligate intracellular acid-fast bacillus with a strong tropism for Schwann cells and skin macrophages, and a preference for cooler tissues that explains why it targets the skin, superficial nerves, the anterior eye, and the testes while sparing warmer internal organs. Because it cannot be grown in artificial culture, the disease is understood and classified largely through the immune-pathological response it provokes.
The organising principle is the strength of cell-mediated immunity (CMI) directed against M. leprae. Where CMI is strong (a vigorous TH1 response with interferon-gamma, macrophage activation, and well-formed epithelioid granulomas), the host contains and kills the bacilli efficiently — producing paucibacillary disease with few lesions, prominent nerve damage from the brisk immune reaction, and a positive lepromin (Mitsuda) skin test. Where CMI is weak or absent (a TH2-skewed response with abundant but ineffective antibody), bacilli multiply unchecked inside foamy macrophages, producing multibacillary disease with numerous lesions, very high bacillary loads, and a negative lepromin test. The continuous gradient between these two immunological poles is exactly what the Ridley-Jopling classification captures.
This immunological framing has two crucial clinical consequences:
- Nerve damage in tuberculoid disease comes from the immune reaction to a few bacilli (intense local inflammation in a nerve), whereas in lepromatous disease it comes from heavy bacillary infiltration of many nerves over time.
- The immunologically unstable borderline parts of the spectrum are the most prone to acute immune-mediated episodes called lepra reactions (covered in a later SDL).
Ridley-Jopling Spectrum — Clinical and Histological Features
Ridley-Jopling Spectrum of Leprosy
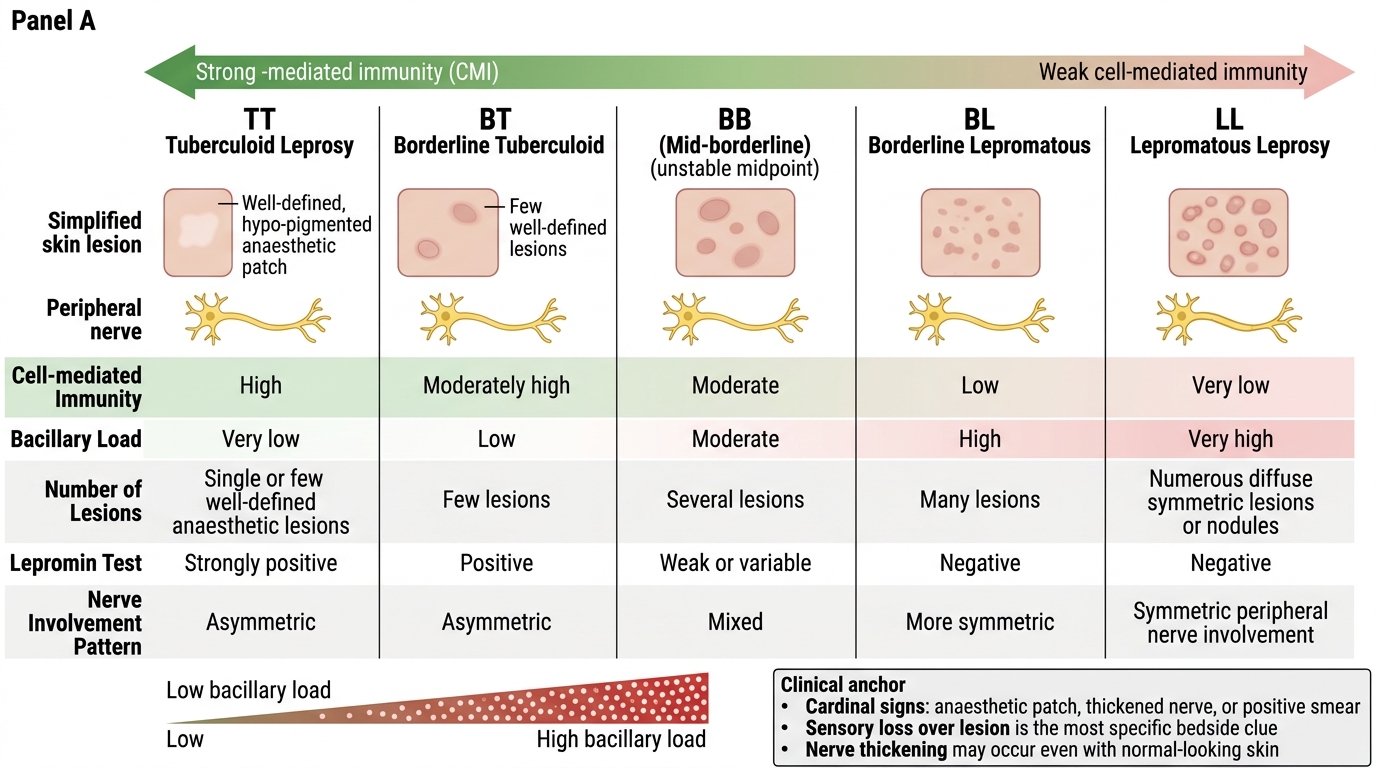
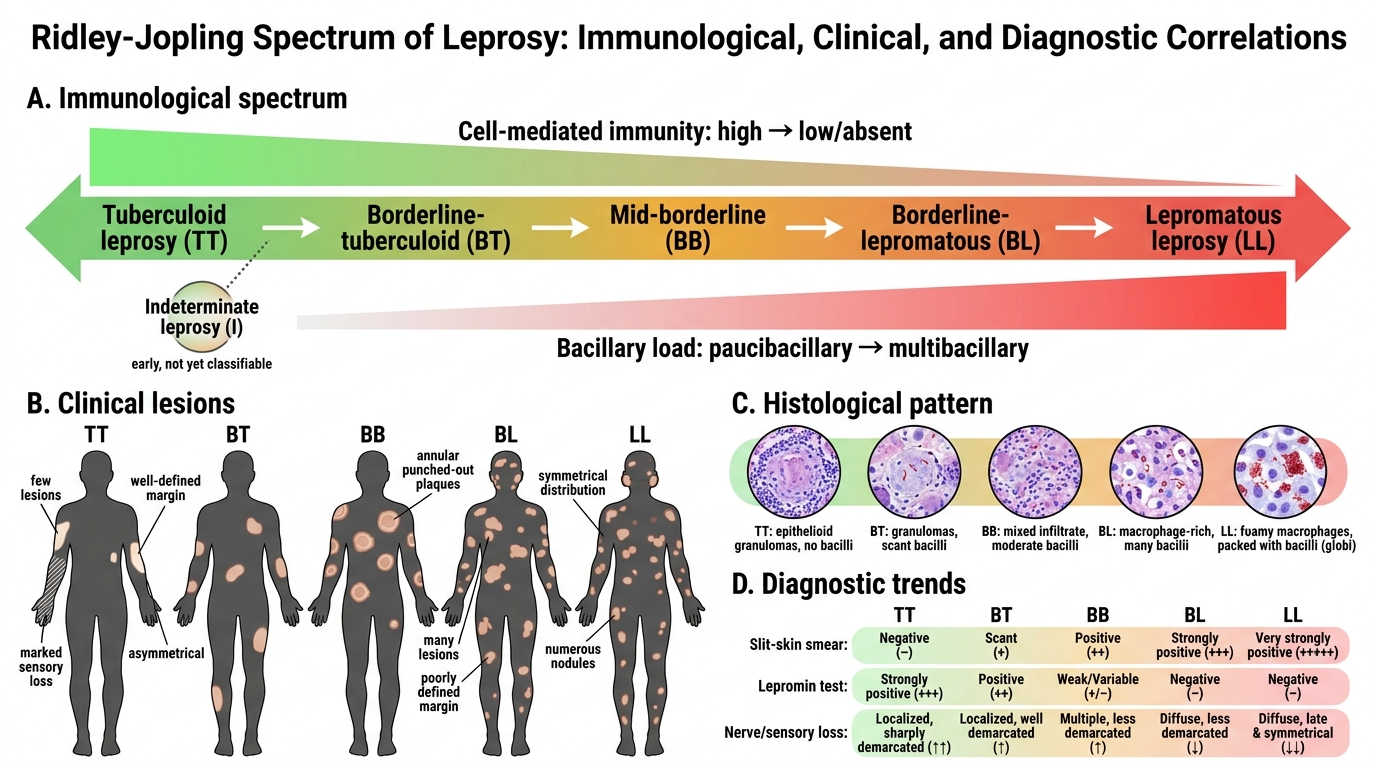
The Ridley-Jopling classification is an immunological and histological spectrum that grades a patient's disease according to their cell-mediated immunity against M. leprae. It runs as a continuum through five points — Tuberculoid (TT) → Borderline-Tuberculoid (BT) → Mid-Borderline (BB) → Borderline-Lepromatous (BL) → Lepromatous (LL) — with Indeterminate (I) leprosy standing apart as an early, not-yet-classifiable lesion. The tuberculoid (TT) pole represents high host immunity and a paucibacillary state; the lepromatous (LL) pole represents low or absent immunity and a multibacillary state; the borderline group (BT, BB, BL) is immunologically unstable and sits between them. This is a continuous spectrum precisely because the underlying variable — cell-mediated immunity — is itself continuous.
Moving from the TT pole to the LL pole, the clinical, bacteriological, and histological features change in a predictable, internally consistent way that you should be able to reconstruct from the immunology alone. As immunity falls, the number of lesions rises, lesions become less well-defined and more symmetrical, sensory loss becomes less sharply demarcated, bacillary load (and the slit-skin smear result) rises, the lepromin test turns from strongly positive to negative, and the histology shifts from well-formed epithelioid granulomas with lymphocytes and no bacilli (TT) to sheets of foamy (Virchow) macrophages packed with bacilli and no organised granuloma (LL). Indeterminate leprosy, by contrast, is a single ill-defined hypopigmented macule with minimal sensory change and nonspecific histology — an early lesion that may heal spontaneously or evolve toward one of the determinate types.
| Feature | TT (Tuberculoid) | BT | BB (Mid-borderline) | BL | LL (Lepromatous) |
|---|---|---|---|---|---|
| Cell-mediated immunity | High | Moderate-high | Intermediate (unstable) | Low | Absent |
| Number of lesions | Single / very few | Few, asymmetric | Several | Many | Innumerable, symmetric |
| Lesion definition | Well-defined, dry, anaesthetic | Fairly defined | 'Punched-out'/annular | Ill-defined | Diffuse infiltration, nodules |
| Sensory loss | Marked, early | Present | Present | Less marked | Late, glove-and-stocking |
| Bacillary load / smear | Negative | Negative or scanty | Moderate | High | Very high (BI 5-6) |
| Lepromin (Mitsuda) test | Strongly positive | Positive | Negative | Negative | Negative |
| Histology | Epithelioid granuloma, lymphocytes, no bacilli | Granuloma with some disorganisation | Diffuse epithelioid, no Langhans | Foamy macrophages, many bacilli | Sheets of foamy (Virchow) macrophages, globi |
Key points:
- Memorise the order TT → BT → BB → BL → LL as a one-way gradient of falling immunity and rising bacillary load.
- Indeterminate leprosy is NOT a point on this spectrum — it is an early, unclassified lesion.
- BB (mid-borderline) is the most immunologically unstable point and the least stable clinically.
SELF-CHECK
Which statement about the Ridley-Jopling spectrum is correct?
A. The lepromatous (LL) pole has high cell-mediated immunity and a low bacillary load
B. The correct order from high to low immunity is LL → BL → BB → BT → TT
C. The tuberculoid (TT) pole has high cell-mediated immunity, few lesions, a negative smear, and a strongly positive lepromin test
D. Indeterminate leprosy is the most advanced point on the Ridley-Jopling spectrum
Reveal Answer
Answer: C. The tuberculoid (TT) pole has high cell-mediated immunity, few lesions, a negative smear, and a strongly positive lepromin test
The tuberculoid (TT) pole represents HIGH cell-mediated immunity: the host contains the organism, producing few well-defined anaesthetic lesions, a negative (paucibacillary) slit-skin smear, and a strongly positive lepromin (Mitsuda) test. The spectrum runs TT → BT → BB → BL → LL in the direction of FALLING immunity and RISING bacillary load, so option 2 reverses the conventional direction and option 1 inverts the LL pole's features. Indeterminate leprosy is an early, not-yet-classifiable lesion that stands apart from the spectrum, not its most advanced point.