Page 2 of 23
DR9.1 | Leprosy Epidemiology Classification and Clinical Features — SDL Guide (Part 2)
WHO Operational Classification — Paucibacillary vs Multibacillary
WHO Operational Classification of Leprosy: PB vs MB
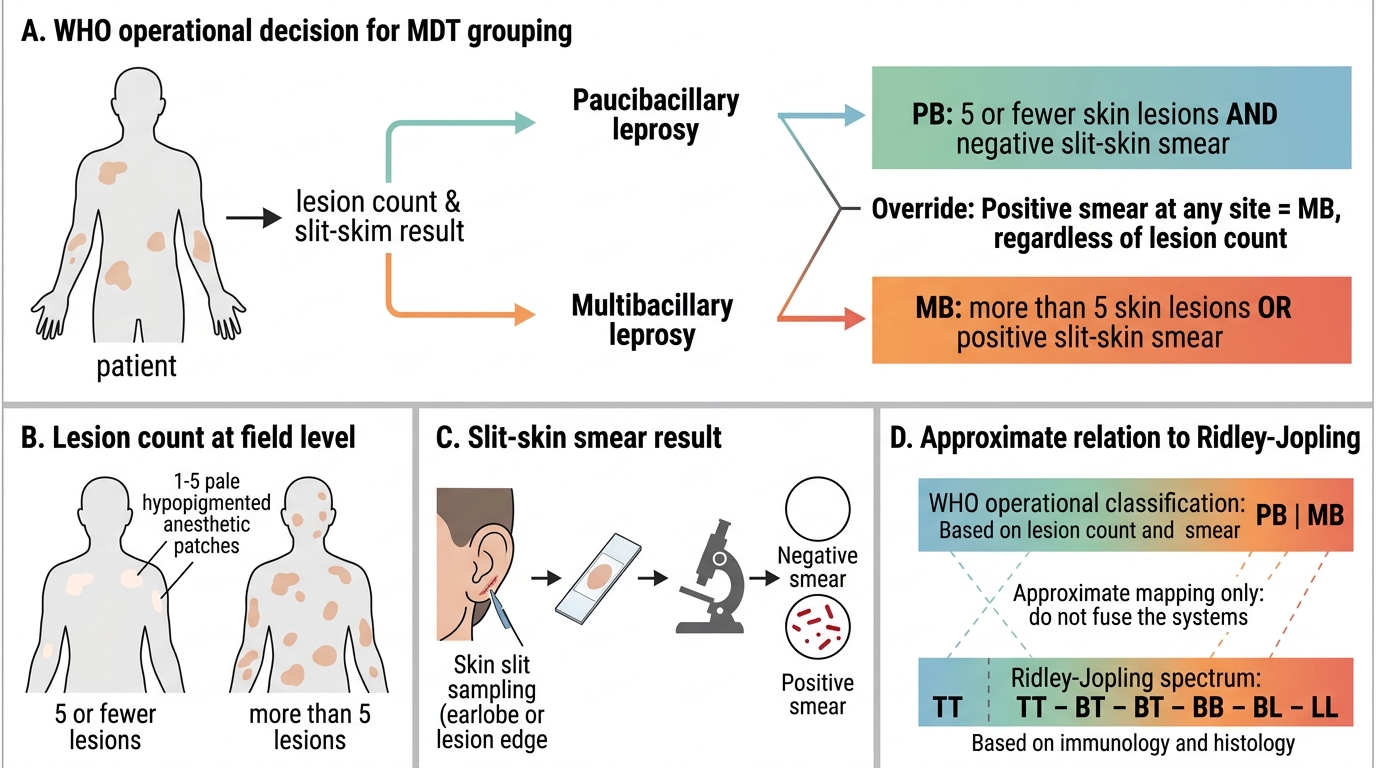
The Ridley-Jopling spectrum is precise but impractical for field programmes, because it requires skin-smear facilities and histopathology that are unavailable at most primary health centres. For this reason the World Health Organization devised a separate, deliberately simple operational classification whose only purpose is to decide which multidrug-therapy regimen a patient receives. This is a different system serving a different goal, and it must never be fused with the Ridley-Jopling spectrum. The operational classification sorts every patient into one of two groups: paucibacillary (PB) or multibacillary (MB).
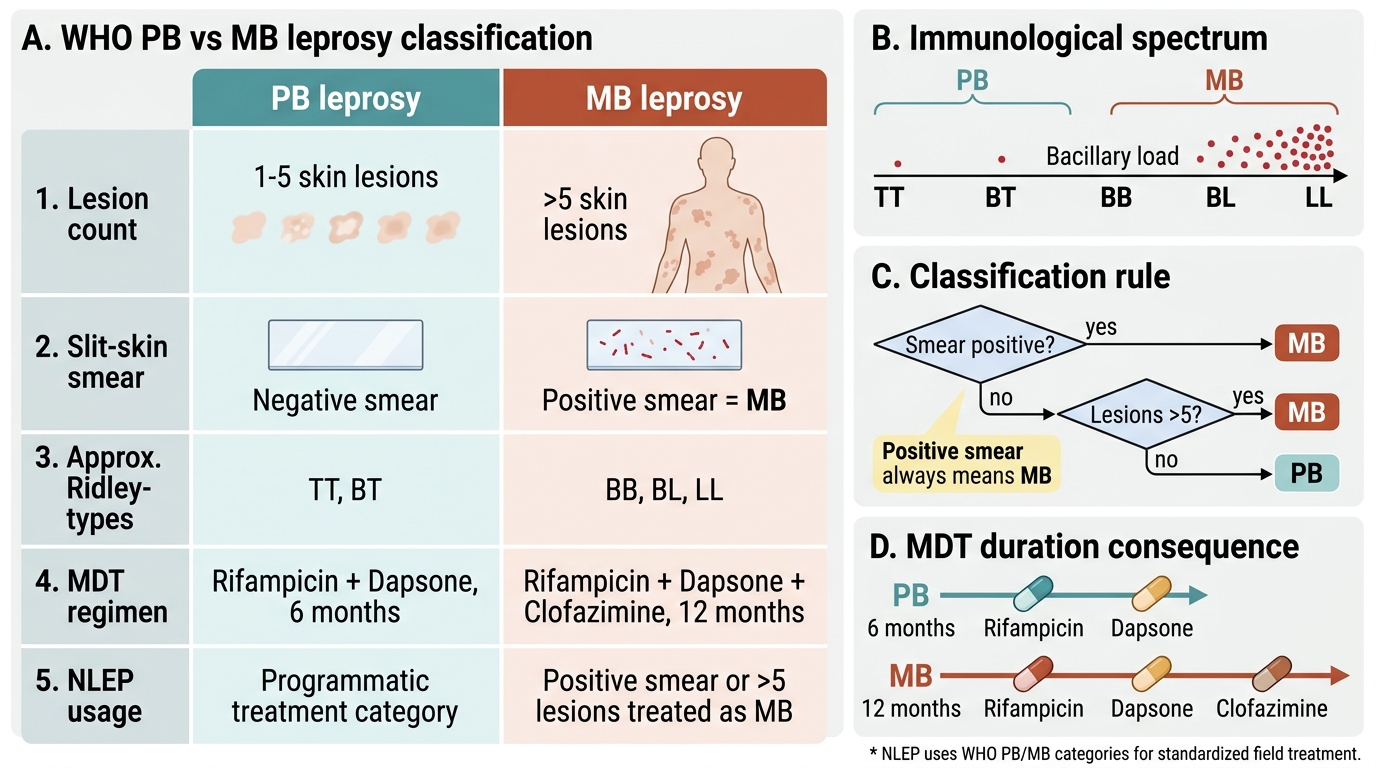
The criteria are defined so they can be applied by counting lesions and, where available, reading a smear. Paucibacillary (PB) leprosy is defined as 5 or fewer skin lesions AND a negative slit-skin smear. Multibacillary (MB) leprosy is defined as more than 5 skin lesions, OR a positive slit-skin smear at any site (a positive smear makes a patient MB regardless of lesion count). Because a positive smear overrides the lesion count, any smear-positive patient is automatically MB. This operational dichotomy maps approximately — but not exactly — onto the Ridley-Jopling spectrum: TT and most BT cases behave as PB, while BB, BL, and LL cases are MB. The mapping is approximate precisely because the two systems are built on different variables (immunology/histology versus a practical lesion-and-smear count), which is why we keep them conceptually separate.
WHO PB vs MB Leprosy Classification
The treatment consequence — developed fully in a later SDL — follows directly from this classification:
- PB leprosy is treated with rifampicin + dapsone for 6 months.
- MB leprosy is treated with rifampicin + dapsone + clofazimine for 12 months.
- A positive smear always means MB, and therefore the longer three-drug regimen.
Epidemiology and NLEP — India's Elimination Effort
Leprosy remains a global public-health problem concentrated in a small number of high-burden countries, and India carries the largest share of the world's new cases each year, alongside Brazil and Indonesia. Although the global introduction of multidrug therapy in the 1980s dramatically reduced the registered prevalence, the disease continues to generate over two hundred thousand new cases worldwide annually, and India alone detects roughly a hundred thousand new cases each year. Importantly, a significant proportion of new cases are multibacillary and a worrying fraction already show visible (Grade 2) disability at the time of diagnosis — direct evidence of continued delayed detection. Understanding this epidemiology is what justifies an active, programmatic approach rather than passive case-finding.
India's response is delivered through the National Leprosy Eradication Programme (NLEP), launched in 1983 and integrated into the general health system, which provides free multidrug therapy through government facilities and pursues a target of elimination defined as a prevalence of fewer than 1 case per 10,000 population, assessed at progressively finer administrative levels (national, state, district, and now sub-district/block). India achieved the WHO elimination target at the national level in 2005, but pockets of high endemicity persist, which is why the programme continues active case-detection campaigns, contact tracing, and — more recently — single-dose rifampicin post-exposure prophylaxis for contacts.
Key epidemiological and programmatic points:
- India reports the largest number of new leprosy cases of any country; the disease is far from eradicated.
- NLEP is the national programme; its operational elimination target is < 1 case per 10,000 population.
- A high proportion of new cases being MB, and the persistence of Grade 2 disability at diagnosis, both signal continued delayed detection and justify active surveillance.
- Leprosy is a notifiable condition under the programme, and free MDT is supplied through government blister packs.
Self-Assessment — Leprosy Classification
Before moving on, consolidate this module by working through the diagnostic and classification reasoning yourself, because the discipline of separating the two classification systems is built only by repeated deliberate practice. For each of the scenarios below, force yourself to do three things in strict order: first decide whether a WHO cardinal sign is present, and name which one; then place the patient on the Ridley-Jopling spectrum using the immunological reasoning about cell-mediated immunity and bacillary load; and finally — as a completely separate step — assign the WHO operational class and the corresponding multidrug-therapy regimen. Resist the temptation to short-circuit from a label such as 'borderline' straight to a drug regimen; always route the treatment decision deliberately through the PB versus MB criteria, remembering that a positive smear overrides any lesion count. Treating these as two independent decisions, every single time, is what protects your patients from being under-treated or mis-staged.
Work through these checkpoints:
- A single well-defined hypopigmented anaesthetic plaque, smear negative, lepromin strongly positive: which Ridley-Jopling type, and is this PB or MB?
- Seven ill-defined infiltrated lesions with a smear positive at the ear lobe: which end of the spectrum, and which MDT regimen and duration?
- A patient with just 3 lesions but a positive slit-skin smear: state the WHO class (and explain why the smear overrides the lesion count).
- An ill-defined hypopigmented macule with minimal sensory change in a child: why is 'indeterminate' the right label and why does it sit off the Ridley-Jopling spectrum?
If you can answer each of these confidently and keep the two classification systems separate while doing so, you have met the core objective of this module.
CLINICAL PEARL
Always test sensation over a suspicious patch and always palpate the peripheral nerves — these two bedside manoeuvres diagnose most leprosy without any laboratory. A hypopigmented patch that is genuinely anaesthetic to temperature and light touch, or a thickened ulnar, common peroneal, or greater auricular nerve, satisfies a WHO cardinal sign on its own. The commonest reason leprosy is missed for months is that the patch is treated as tinea or vitiligo because nobody tested its sensation. When you find leprosy, immediately do two separate things: place the patient on the Ridley-Jopling spectrum (for prognosis and reaction risk) AND assign the WHO operational class PB or MB (to choose the MDT regimen). Confusing these two systems — for example, treating a smear-positive 'borderline' patient with the 6-month PB regimen — is a classic and harmful error.