Page 4 of 23
DR9.2 | Leprosy Neurologic Examination — SDL Guide
Learning Objectives
- State why systematic nerve examination is central to leprosy diagnosis, classification, and disability prevention
- Identify the cardinal peripheral nerves examined in leprosy and their anatomical palpation sites
- Demonstrate the technique of nerve palpation, sensory testing, and voluntary muscle testing in a patient with leprosy
- Interpret examination findings to grade nerve function impairment and assign WHO disability grade, and recognise when urgent corticosteroid treatment is indicated
INSTRUCTIONS
Leprosy is, above all, a disease of peripheral nerves, and it is nerve damage — not the skin disease — that produces the deformity, disability, and stigma associated with the condition. A careful, reproducible neurological examination is therefore the most valuable clinical skill in leprosy care: it confirms the diagnosis (a thickened nerve is a cardinal sign), it tracks the disease, and — most importantly — it detects new nerve function impairment early, when corticosteroids can still recover function. This skills module teaches you the structured examination: which nerves to palpate and where, how to test sensation and motor power, and how to convert your findings into a nerve-function and WHO disability grade that drives management decisions.
References
- Neena Khanna. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Leprosy — Examination of Nerves (textbook)
- IADVL Textbook of Dermatology, 4th ed. Section: Leprosy — Nerve Function Assessment and Disability (textbook)
- National Leprosy Eradication Programme (NLEP) — Disability Prevention and Medical Rehabilitation (DPMR) Guidelines; WHO grading of disability (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 32-year-old woman who completed multidrug therapy for borderline leprosy six weeks ago returns because the skin lesions on her arm have suddenly become red, swollen, and tender. She mentions, almost in passing, that her right hand has felt 'weak' for a few days and she keeps dropping objects. You could be forgiven for focusing on the inflamed skin — but the real emergency is in her hand. When you test her grip and ask her to splay her fingers against resistance, the little and ring fingers are weak, and her ulnar nerve at the elbow is thickened and exquisitely tender. She is in a Type 1 reaction with acute neuritis, and the nerve damage happening right now is reversible — but only if you detect it today and start corticosteroids. If you miss it, she will leave with a claw hand that no treatment can undo. Everything hinges on whether you perform a competent neurological examination, and whether you do it before the skin distracts you.
WHY THIS MATTERS
Every clinician who manages leprosy must be able to examine the peripheral nerves competently, because nerve function — not the skin disease — determines a patient's lifelong outcome. The examination has three jobs that you will use at every leprosy encounter: it helps establish the diagnosis (a thickened nerve is one of the three WHO cardinal signs); it detects nerve function impairment early enough that corticosteroids can still recover lost sensation and power; and it produces the WHO disability grade that drives counselling, footwear, physiotherapy, and surgical referral. A structured, reproducible nerve examination performed at every visit is the single most effective way to prevent the deformities that cause leprosy's stigma. This is a hands-on skill you will perform repeatedly, and performing it the same careful way each time is what makes your findings trustworthy over months of follow-up.
RECALL
Before beginning, recall from Anatomy the surface course of the major peripheral nerves you will palpate: the ulnar nerve running behind the medial epicondyle of the elbow; the common peroneal nerve winding around the neck of the fibula just below and lateral to the knee; the posterior tibial nerve passing behind the medial malleolus; the greater auricular nerve crossing the sternocleidomastoid in the posterior triangle of the neck; and the radial cutaneous nerve over the lateral wrist. Recall also the motor territories: ulnar nerve to the intrinsic hand muscles (clawing of the ring and little fingers when damaged), common peroneal nerve to the dorsiflexors of the foot (foot drop when damaged), and posterior tibial nerve to the small muscles of the foot and the sole's sensation. This anatomy is the scaffold on which the leprosy nerve examination is built.
Why Nerve Examination Is Central to Leprosy Care
Why Nerve Examination Is Central to Leprosy Care
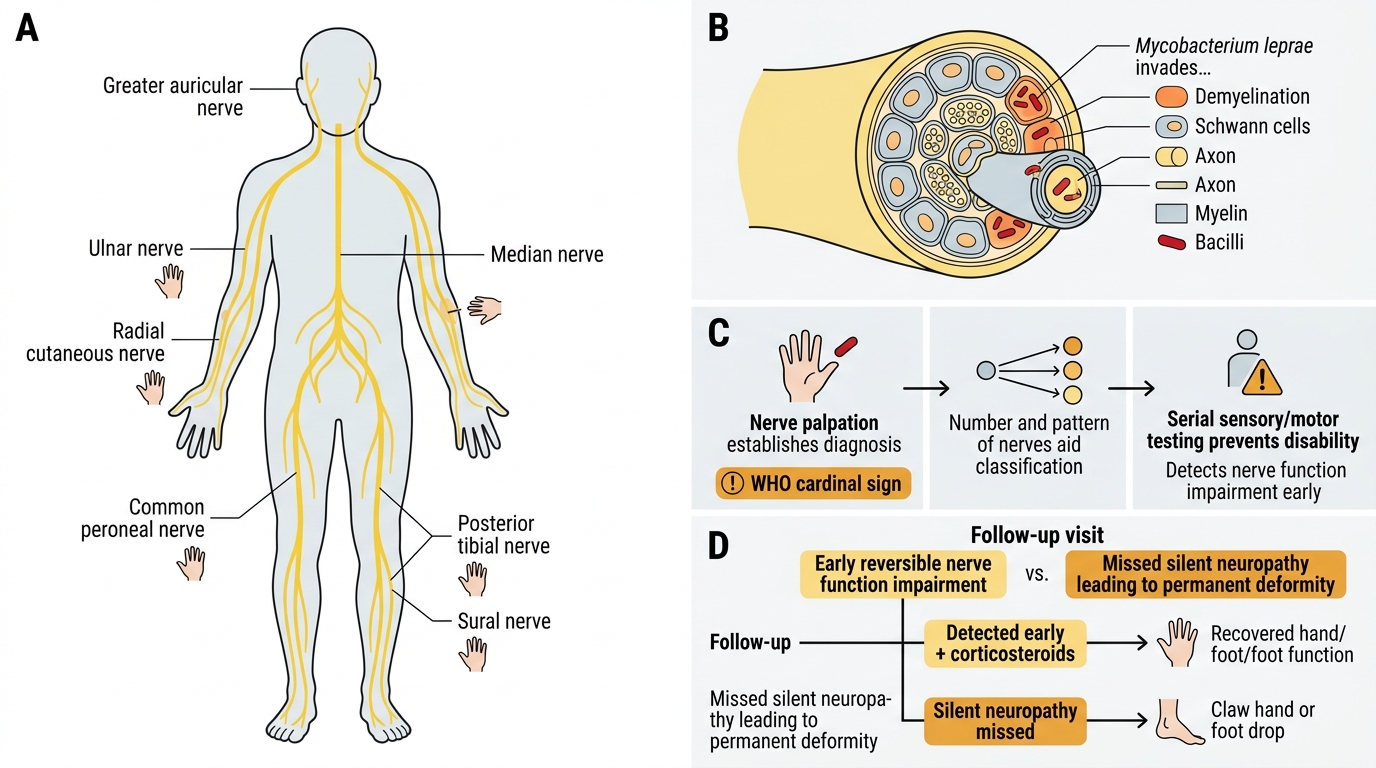
The clinical indication for nerve examination in leprosy is absolute: because Mycobacterium leprae invades Schwann cells and damages peripheral nerves, the nerve examination is simultaneously a diagnostic test, a classification aid, and the principal tool for preventing disability. A thickened peripheral nerve is one of the three WHO cardinal signs, so palpation can establish the diagnosis on its own. The pattern and number of nerves involved help locate a patient on the disease spectrum. And — most consequentially — repeated examination detects nerve function impairment (NFI): new sensory or motor loss that, if caught early and treated with corticosteroids, is largely reversible, but if missed becomes permanent deformity.
Not every patient needs the same intensity of assessment at every moment, but every leprosy patient needs a documented baseline nerve examination at diagnosis and a repeat examination at every follow-up visit, because nerve damage can progress silently. A particular trap is silent neuropathy — nerve function loss occurring WITHOUT pain or visible skin inflammation, especially in borderline cases — which is detected only by actively testing sensation and power at each visit rather than waiting for the patient to complain. The borderline patients (BT, BB, BL) are at highest risk because they are prone to Type 1 reactions that attack the nerves acutely.
Key reasons the examination is non-negotiable:
- A thickened nerve is a WHO cardinal sign and can diagnose leprosy by itself.
- Early detection of NFI allows corticosteroid rescue of nerve function; delay makes the loss permanent.
- Silent neuropathy has no symptoms and is found only by routine active testing.
- The examination yields the WHO disability grade that drives downstream care.
Peripheral Nerves Affected and Their Anatomical Landmarks
Peripheral Nerves Examined in Leprosy
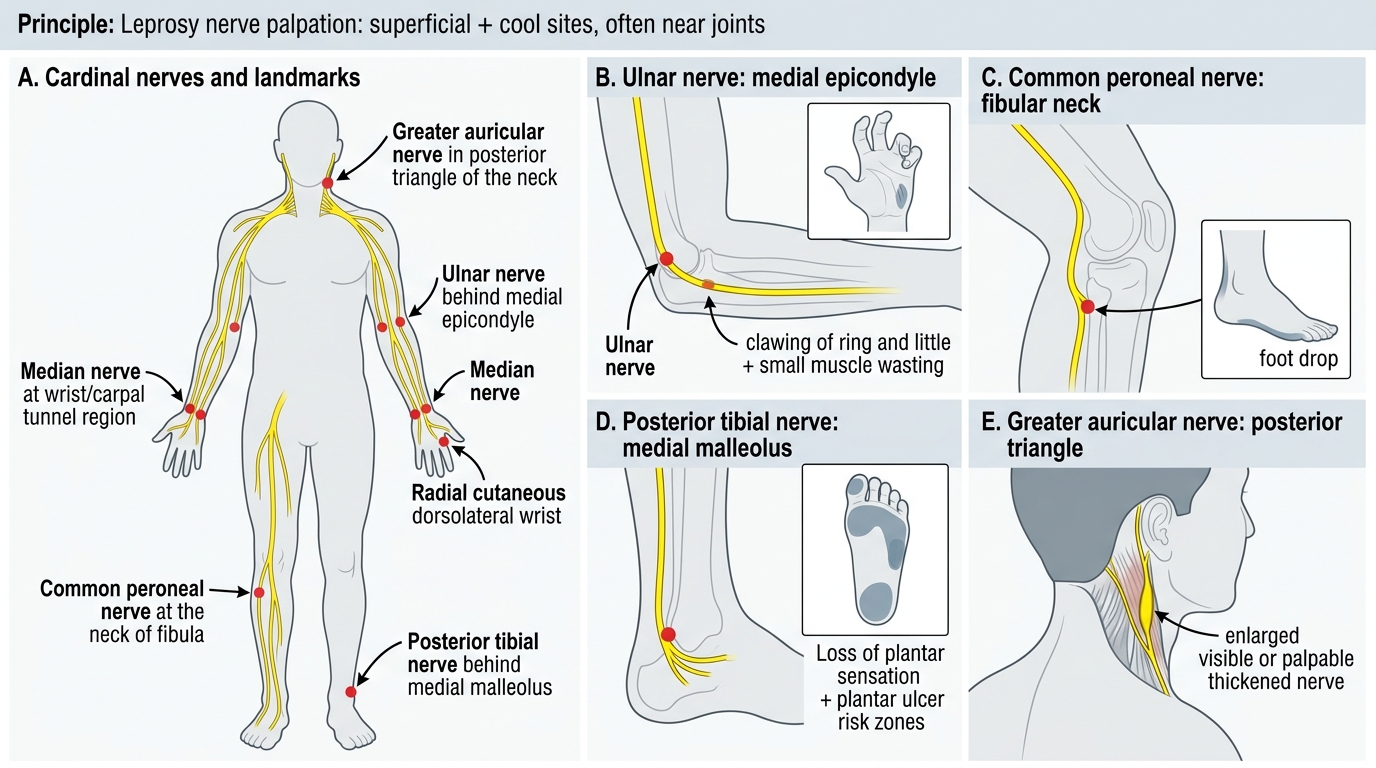
The principle behind nerve palpation in leprosy is that the organism preferentially damages peripheral nerves at sites where they are superficial and cool — typically where a nerve crosses a joint or lies just under the skin — so a defined set of nerves is examined at defined landmarks every time. Knowing exactly where each nerve lies, what it supplies, and which deformity its damage produces lets you predict and interpret your findings rather than palpating blindly. The materials required are minimal: your hands for palpation, a wisp of cotton wool and ideally a graded monofilament for sensory testing, and a warm and a cold object for temperature testing.
The cardinal nerves examined in leprosy, with their landmarks and consequences of damage, are summarised below. The ulnar nerve is the most commonly affected nerve in leprosy and is palpated behind the medial epicondyle of the elbow; its damage causes clawing of the ring and little fingers with wasting of the small hand muscles. The common (lateral) peroneal nerve is palpated at the neck of the fibula and its damage causes foot drop. The posterior tibial nerve is palpated behind the medial malleolus and its damage causes loss of sole sensation (predisposing to plantar ulcers) and clawing of the toes. The greater auricular nerve is palpated in the posterior triangle of the neck and may be visibly enlarged. The radial cutaneous nerve is palpated over the lateral aspect of the wrist.
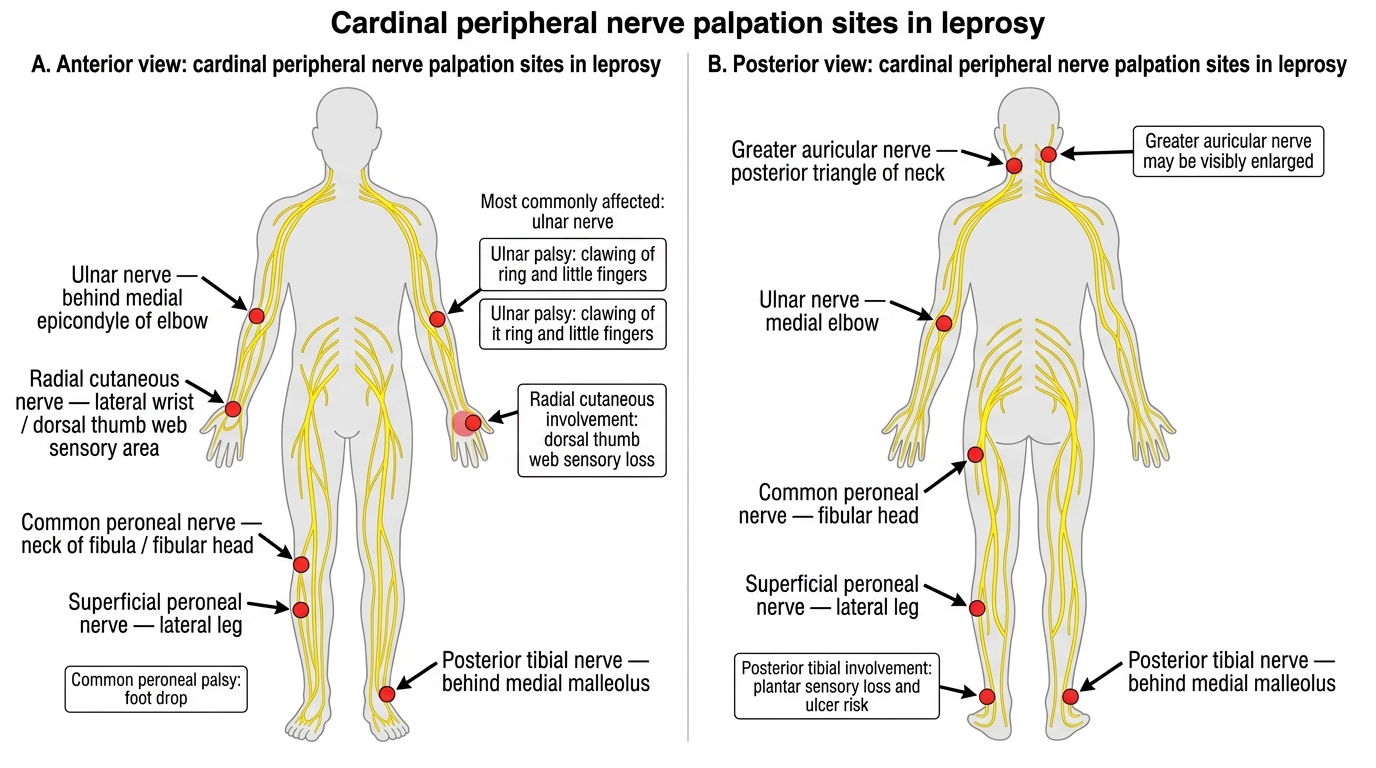
Six Cardinal Peripheral Nerve Palpation Sites in Leprosy
Nerves and their landmarks:
- Ulnar — behind medial epicondyle of elbow — claw hand (ring + little fingers); most commonly affected.
- Common peroneal — neck of fibula — foot drop.
- Posterior tibial — behind medial malleolus — plantar sensory loss, clawed toes, plantar ulcer risk.
- Greater auricular — posterior triangle of neck — often visibly enlarged.
- Radial cutaneous — lateral wrist — sensory loss over dorsal thumb web.
SELF-CHECK
Which peripheral nerve is MOST commonly affected in leprosy, where is it palpated, and what deformity follows its damage?
A. Common peroneal nerve, palpated behind the medial malleolus, causing foot drop
B. Ulnar nerve, palpated behind the medial epicondyle of the elbow, causing clawing of the ring and little fingers
C. Posterior tibial nerve, palpated at the neck of the fibula, causing wrist drop
D. Greater auricular nerve, palpated at the elbow, causing claw hand
Reveal Answer
Answer: B. Ulnar nerve, palpated behind the medial epicondyle of the elbow, causing clawing of the ring and little fingers
The ulnar nerve is the most commonly affected nerve in leprosy. It is palpated behind the medial epicondyle of the elbow, and its damage produces clawing of the ring and little fingers (ulnar claw) with wasting of the intrinsic hand muscles. The other options scramble the landmark-to-deformity pairings: the common peroneal nerve is palpated at the neck of the fibula (foot drop), and the posterior tibial nerve is palpated behind the medial malleolus (plantar sensory loss and clawed toes).
Technique of Nerve Palpation, Sensory Testing, and Voluntary Muscle Testing
Provided image
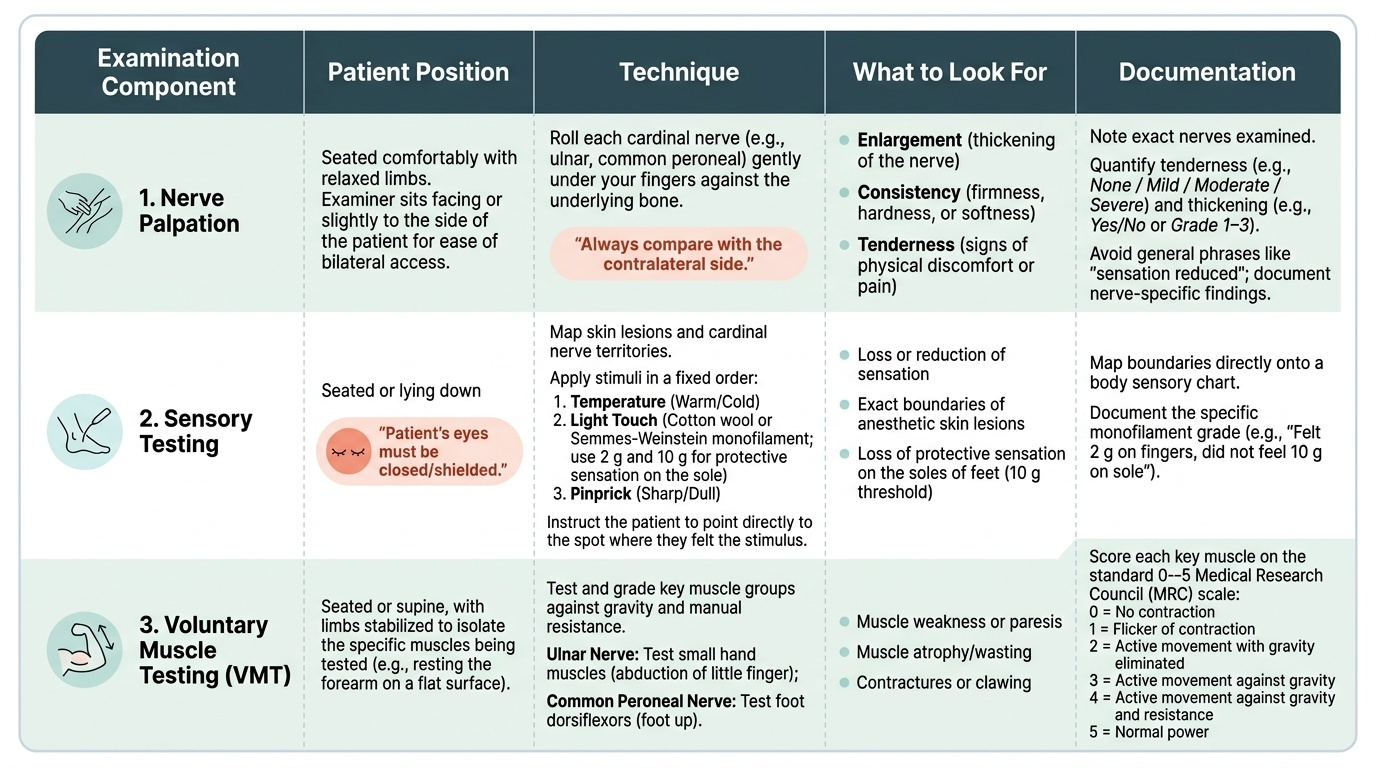
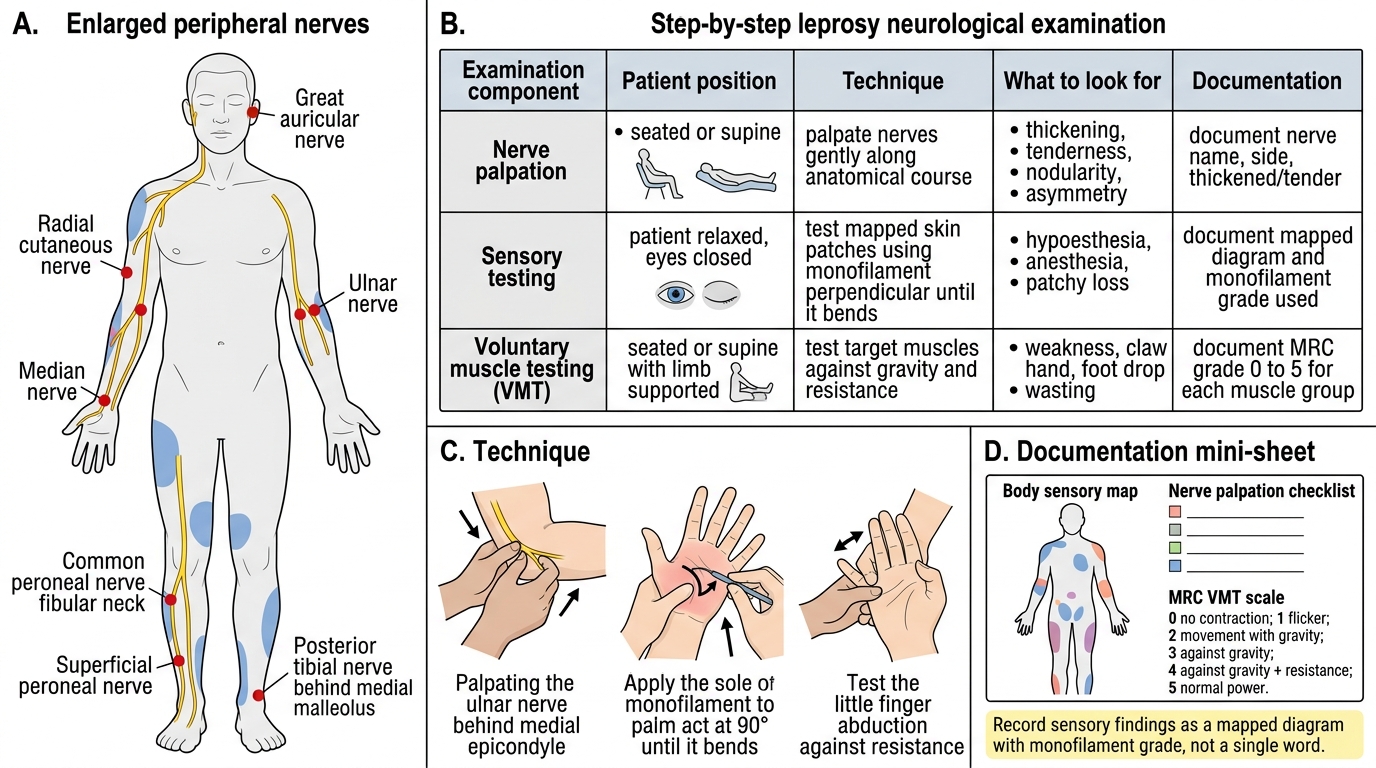
The technique of the leprosy neurological examination follows a fixed sequence so that findings are reproducible across examiners and across months of follow-up, which is essential when you are trying to detect a small new deficit. Begin by positioning and reassuring the patient, then examine in three components in the same order every time: nerve palpation, sensory testing, and voluntary muscle testing. Throughout, compare the two sides and document quantitatively (which fingers, which monofilament grade, which muscle power), because 'sensation reduced' recorded once is useless for detecting change later.
For nerve palpation, roll each cardinal nerve gently under your fingers against the underlying bone, assessing three things: enlargement (thickening), consistency, and tenderness — and always compare with the contralateral nerve. For sensory testing, map the skin lesions and the territories of the cardinal nerves using graded stimuli in the order temperature, then light touch (cotton wool or a Semmes-Weinstein monofilament — the 2 g/10 g monofilament tests protective sensation on the sole), then pinprick; the patient closes their eyes and points to where they feel the stimulus. For voluntary muscle testing (VMT), grade the key muscles (e.g., small hand muscles for the ulnar nerve, foot dorsiflexors for the common peroneal nerve) on the standard 0-5 Medical Research Council scale.
Leprosy Neurological Examination: Step-by-Step Procedure
The standard VMT (MRC) grades are:
- 0 = no contraction; 1 = flicker of contraction; 2 = movement only with gravity eliminated; 3 = movement against gravity; 4 = movement against gravity and some resistance; 5 = normal power.
- Record sensory findings as a mapped diagram with the monofilament grade used, not as a single word.