Page 5 of 23
DR9.2 | Leprosy Neurologic Examination — SDL Guide (Part 2)
Interpreting Findings — NFI Grading and Disability Classification
Leprosy NFI and WHO Disability Grading
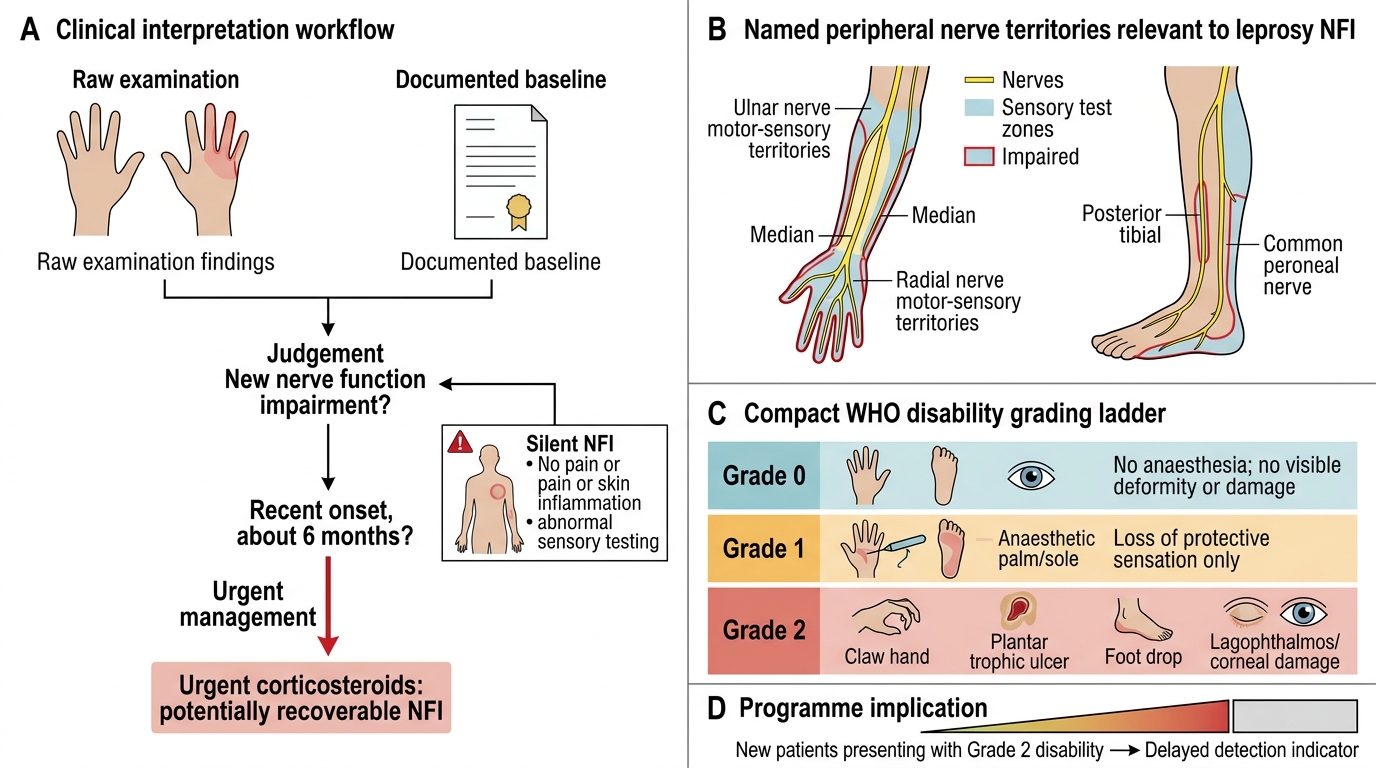
Interpreting the examination means converting your raw findings into two clinically actionable judgements: whether there is new nerve function impairment, and what WHO disability grade the patient has. Nerve function impairment (NFI) is defined as a new loss of sensory or motor function in the territory of a named nerve, occurring during treatment or within a defined period after release from treatment; the key word is new, which is why a documented baseline is indispensable. NFI of recent onset (conventionally within about six months) is the finding that mandates urgent corticosteroids, because at that stage the loss is still recoverable. Remember that NFI can be 'silent' — present on testing but without pain or skin inflammation — particularly in borderline disease.
The WHO disability grading translates examination findings into a simple 0-1-2 scale applied separately to each eye, each hand, and each foot. Grade 0 means no anaesthesia and no visible deformity or damage. Grade 1 means loss of protective sensation (anaesthesia) is present but there is no visible deformity or damage. Grade 2 means visible deformity or damage is present — for example lagophthalmos and corneal damage in the eye, clawing or a resorbed digit or a trophic ulcer in the hand, or foot drop or a plantar ulcer in the foot. The proportion of new patients presenting at Grade 2 is an important programme indicator of delayed detection.
Interpretation rules to apply:
- New sensory or motor loss = NFI; recent-onset NFI is an indication for urgent corticosteroids.
- Grade the eye, hand, and foot separately: Grade 0 (normal), Grade 1 (anaesthesia only), Grade 2 (visible deformity/damage).
- Suspect silent neuropathy whenever testing shows loss without pain or inflammation.
SELF-CHECK
On examination a leprosy patient has loss of protective sensation in the hand but no visible deformity, claw, ulcer, or resorption. What is the WHO disability grade for that hand?
A. Grade 0 — because there is no visible deformity
B. Grade 1 — anaesthesia (loss of protective sensation) is present but there is no visible deformity or damage
C. Grade 2 — any sensory loss automatically counts as visible damage
D. Grade 3 — sensory loss in the hand is the most severe grade
Reveal Answer
Answer: B. Grade 1 — anaesthesia (loss of protective sensation) is present but there is no visible deformity or damage
WHO disability grading is applied separately to each eye, hand, and foot. Grade 1 is defined as loss of protective sensation (anaesthesia) WITHOUT visible deformity or damage — exactly this scenario. Grade 0 requires no anaesthesia at all. Grade 2 requires VISIBLE deformity or damage (claw hand, trophic ulcer, digit resorption, lagophthalmos, foot drop, plantar ulcer). There is no Grade 3 in the WHO leprosy disability scale, which runs only 0, 1, and 2.
Applied Practice — Examination in Common Leprosy Scenarios
Examination Patterns in Common Leprosy Scenarios
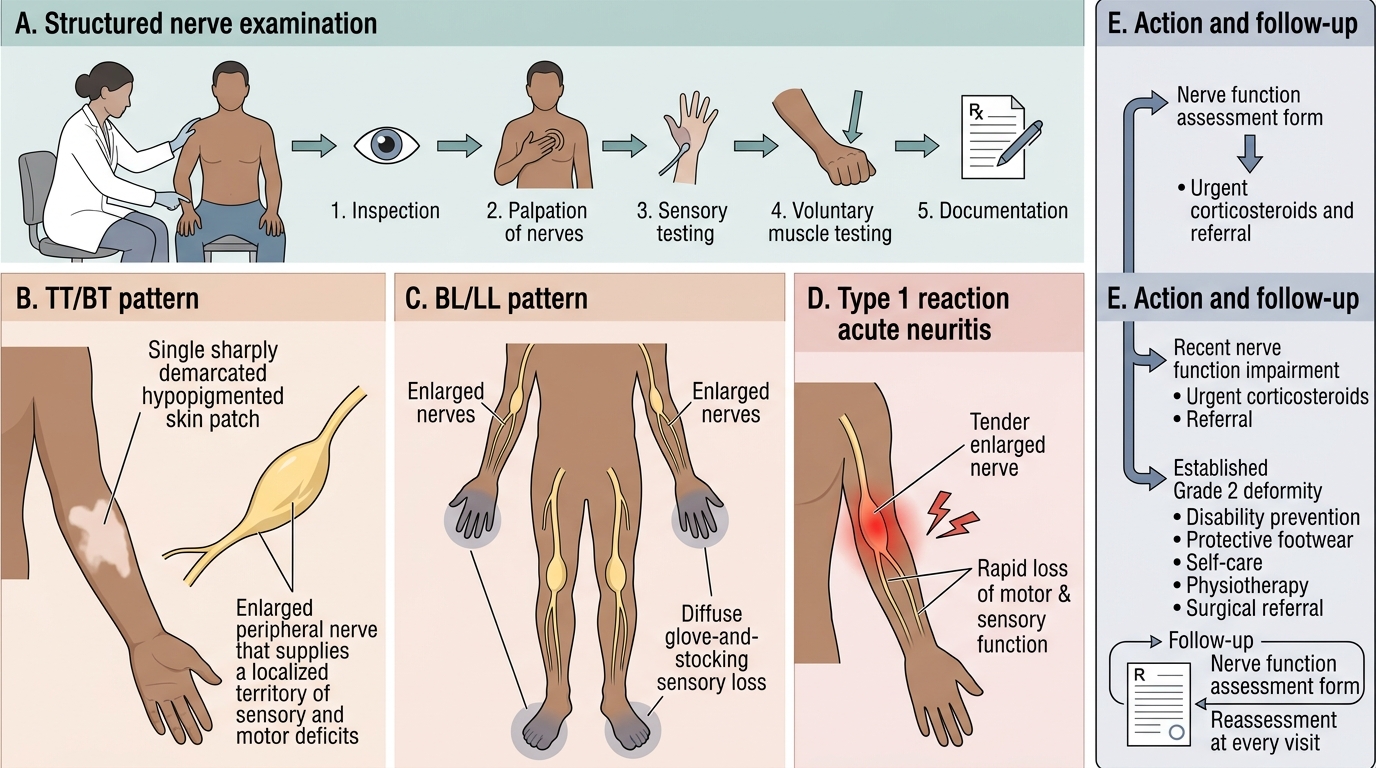
Putting the examination to work means recognising the patterns you will actually meet and translating them into action, because the same structured examination yields very different findings across the disease spectrum. In tuberculoid/borderline-tuberculoid (TT/BT) disease you typically find a single or few thickened nerves with a sharply demarcated sensory and motor deficit in that nerve's territory. In borderline-lepromatous/lepromatous (BL/LL) disease you find multiple, often symmetrical nerve involvement with a more diffuse glove-and-stocking sensory loss. During a Type 1 (reversal) reaction you find acute neuritis — a nerve that is suddenly tender, enlarged, and losing function — which is the time-critical emergency from the opening scenario.
Your examination findings drive concrete decisions and a documentation discipline. A patient with recent-onset motor or sensory loss (NFI) in any scenario needs urgent corticosteroid therapy and prompt referral; a patient with established Grade 2 deformity needs disability-prevention measures (protective footwear, self-care, physiotherapy, surgical referral) rather than steroids alone. Every finding is recorded on a standard nerve-function-assessment form with a follow-up plan, because the value of today's examination is realised only when it is compared with the next one. Under NLEP/DPMR practice, nerve function is reassessed at every visit during treatment and for a defined surveillance period afterward.
Applied checkpoints:
- TT/BT → few nerves, sharply demarcated deficit; BL/LL → multiple nerves, diffuse glove-and-stocking loss.
- Acute tender enlarged nerve with new weakness during/after MDT → Type 1 reaction with neuritis → urgent corticosteroids.
- Document every assessment on a standard form and set the next review date; compare serially to catch silent progression.
Self-Assessment — Leprosy Neurological Examination
Consolidate this skill by mentally rehearsing the full examination and then reasoning through the scenarios below, because a neurological examination is only as good as your ability to interpret it under time pressure at the bedside. For each scenario, walk through the same disciplined sequence you would use on a real patient: palpate and compare the cardinal nerves for thickening and tenderness, map sensation with graded stimuli, grade the key muscles on the 0-5 scale, then decide (a) is there NEW nerve function impairment, (b) what is the WHO disability grade for each affected part, and (c) does this finding require urgent corticosteroids or disability-prevention measures? Naming the nerve, the grade, and the action — in that order — is the habit that turns a competent examination into a competent decision.
Test yourself on these:
- A patient develops clawing of the right ring and little fingers with a tender, thickened ulnar nerve two months after starting MDT — name the nerve, the likely mechanism, and the immediate management.
- A foot with loss of protective sensation on the sole but no ulcer and no deformity — assign the WHO grade for that foot.
- A foot drop with a visibly wasted anterior compartment — assign the WHO grade and state the responsible nerve.
- A borderline patient with no symptoms but new inability to feel the 10 g monofilament on the sole at this visit compared with the last — what is this called, and why does it still warrant treatment?
If you can move from examination findings to nerve, to grade, to action for each of these, you have met the objective of this skills module.
CLINICAL PEARL
Acute neuritis in leprosy is a medical emergency: a nerve that becomes suddenly tender, thickened, and weak is losing function that you can still save with corticosteroids — but only if you act the same day. Do not let inflamed skin lesions distract you from testing nerve function. At every leprosy visit, actively test sensation and power even in a patient with no complaints, because silent neuropathy — nerve damage without pain or visible inflammation — is common in borderline disease and is detectable only by routine testing against a documented baseline. The mantra is: palpate every cardinal nerve, map sensation, grade power, compare with last visit, and treat new (recent-onset) impairment urgently. A claw hand or foot drop prevented today is a lifetime of disability and stigma avoided.