Page 7 of 23
DR9.3 | Slit Skin Smear in Leprosy — SDL Guide
Learning Objectives
- Enumerate the indications for performing a slit-skin smear in leprosy
- Describe the principle of the smear and the staining method used to demonstrate Mycobacterium leprae
- Describe the standard sites and the step-by-step technique of slit-skin smear collection
- Interpret the Bacteriological Index and Morphological Index and apply smear results to WHO classification, treatment monitoring, and relapse detection
INSTRUCTIONS
The slit-skin smear is the simplest laboratory test in leprosy and, in many ways, the most decisive: a single positive smear at any site reclassifies a patient as multibacillary and commits them to the longer three-drug regimen. It confirms the diagnosis where the clinical picture is ambiguous, provides a baseline bacterial load before treatment, tracks the response to multidrug therapy, and detects relapse after release from treatment. As a future clinician you will need to know exactly when to request a smear, understand the staining principle, recognise a correctly taken specimen, and — most importantly — interpret the Bacteriological and Morphological Indices that the report contains. This module builds that competence so that a smear result becomes an actionable clinical decision rather than an opaque number.
References
- Neena Khanna. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Leprosy — Laboratory Diagnosis (textbook)
- IADVL Textbook of Dermatology, 4th ed. Section: Leprosy — Slit-Skin Smear and Bacteriological/Morphological Index (textbook)
- National Leprosy Eradication Programme (NLEP) Laboratory Manual; WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy 2018 (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Two patients sit in your clinic on the same morning. The first has four hypopigmented patches and you are fairly sure he is paucibacillary — six months of treatment, you think. The second has what looks like only five patches, and on clinical grounds you are tempted to treat her identically. But you order a slit-skin smear on both. The first man's smear is negative at every site. The woman's smear, taken from her ear lobe, is teeming with acid-fast bacilli — a Bacteriological Index of 4+. In that single result, everything changes: she is multibacillary, not paucibacillary, and she needs twelve months of three-drug therapy, not six months of two drugs. Had you classified her on the appearance of her skin alone, you would have under-treated her, risked relapse, and left her infectious for longer. A few drops of dermal pulp on a glass slide, stained red against a blue background, just made the most important treatment decision of her year.
WHY THIS MATTERS
The slit-skin smear matters to you as a clinician because it converts a clinical impression into an objective treatment decision, and the stakes of that decision are high. A positive smear at any site defines a patient as multibacillary, doubling the treatment duration and adding a third drug — so a smear can be the difference between adequate and inadequate therapy. Beyond initial classification, the smear is how you monitor whether treatment is working (the bacterial load should fall over time) and how you detect relapse after a patient has finished therapy. You will need to know when a smear is indicated, what a correctly taken specimen looks like, and how to read the Bacteriological Index report. Understanding this test protects your patients from both under-treatment and unnecessary over-treatment, and it underpins the surveillance that keeps leprosy programmes honest.
RECALL
Before beginning, recall from Microbiology that Mycobacterium leprae is an acid-fast bacillus: its waxy, mycolic-acid-rich cell wall resists decolourisation by acid-alcohol after staining with carbol fuchsin, which is the basis of the Ziehl-Neelsen stain — bacilli appear red against a blue (methylene blue) counterstain. Recall that for leprosy specifically, a modified acid-fast stain, the Fite-Faraco stain, is often preferred for tissue sections because M. leprae is less strongly acid-fast than M. tuberculosis and can be lost with the harsher standard decolourisation. Recall also from the classification module that the bacillary load rises steadily from the tuberculoid pole (smear negative) to the lepromatous pole (smear strongly positive), and that a positive smear places a patient in the WHO multibacillary group.
When and Why to Perform a Slit-Skin Smear
When and Why to Perform a Slit-Skin Smear
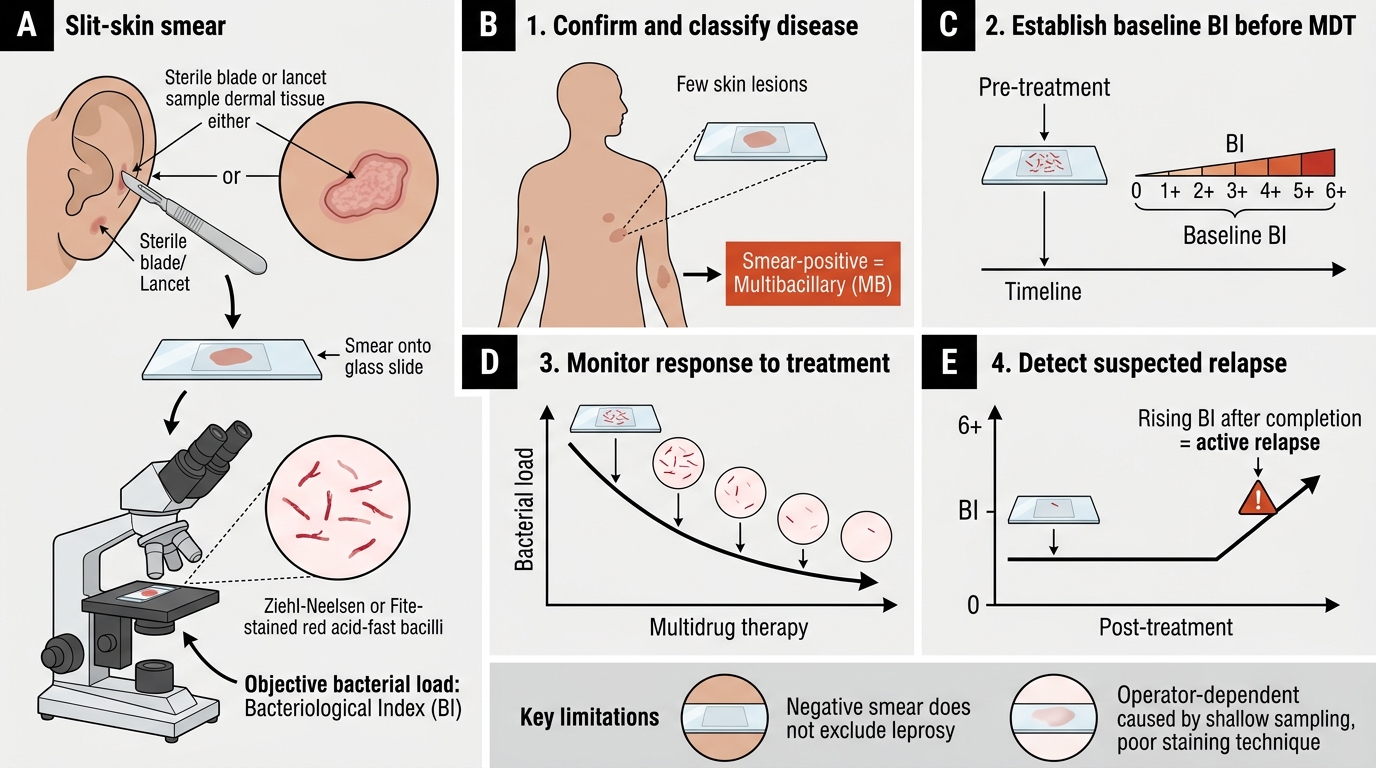
The clinical indication for a slit-skin smear is to obtain an objective measure of a patient's bacterial load when that information will change management, and there are four well-defined situations in which it does. First, it is used to confirm and classify disease — most importantly to establish multibacillary status, since a positive smear at any site defines a patient as MB regardless of how few lesions they have. Second, it provides a baseline bacterial load (a baseline Bacteriological Index) before multidrug therapy begins, against which later smears are compared. Third, it is used to monitor the response to treatment, since the bacterial load should fall progressively on adequate therapy. Fourth, it is the key test in suspected relapse, where a rising bacterial load after completion of treatment signals returning active disease.
Understanding the limitations of the test is part of using it well. The smear is insensitive at the tuberculoid end of the spectrum — paucibacillary patients are smear-negative by definition, so a negative smear never excludes leprosy. The result is also operator-dependent: an inadequately deep or poorly stained specimen can be falsely negative. For these reasons the WHO operational classification can be applied on clinical (lesion-count) grounds alone where smear facilities are unavailable, but the smear remains the definitive way to detect the smear-positive patient who must be treated as MB. There are practical precautions too — bleeding tendency or anticoagulation warrants care when making the incision.
Indications to remember:
- Classification — a positive smear at any site = multibacillary (overrides lesion count).
- Baseline BI before starting MDT.
- Monitoring the fall in bacterial load during treatment.
- Suspected relapse — detecting a rising bacterial load after release from treatment.
- Remember the key limitation: a negative smear does not exclude leprosy (paucibacillary disease is smear-negative).
SELF-CHECK
A patient has only 4 skin lesions, but a slit-skin smear taken from the ear lobe is positive for acid-fast bacilli. How should this patient be classified and treated?
A. Paucibacillary — because there are 5 or fewer lesions, treat with rifampicin + dapsone for 6 months
B. Multibacillary — because a positive smear at any site overrides the lesion count, treat with rifampicin + dapsone + clofazimine for 12 months
C. Indeterminate — a single positive smear is not enough to classify
D. Paucibacillary — the smear result does not affect WHO operational classification
Reveal Answer
Answer: B. Multibacillary — because a positive smear at any site overrides the lesion count, treat with rifampicin + dapsone + clofazimine for 12 months
A positive slit-skin smear at ANY site defines a patient as multibacillary (MB) regardless of how few skin lesions are present — the smear result overrides the lesion count. This patient therefore receives the MB regimen: rifampicin + dapsone + clofazimine for 12 months, not the 6-month paucibacillary regimen. Classifying on lesion count alone here would under-treat the patient. This is exactly why the smear is requested when the clinical picture is borderline.
Principle, Staining Basis, and Materials Required
Principle and Materials for Slit-Skin Smear in Leprosy
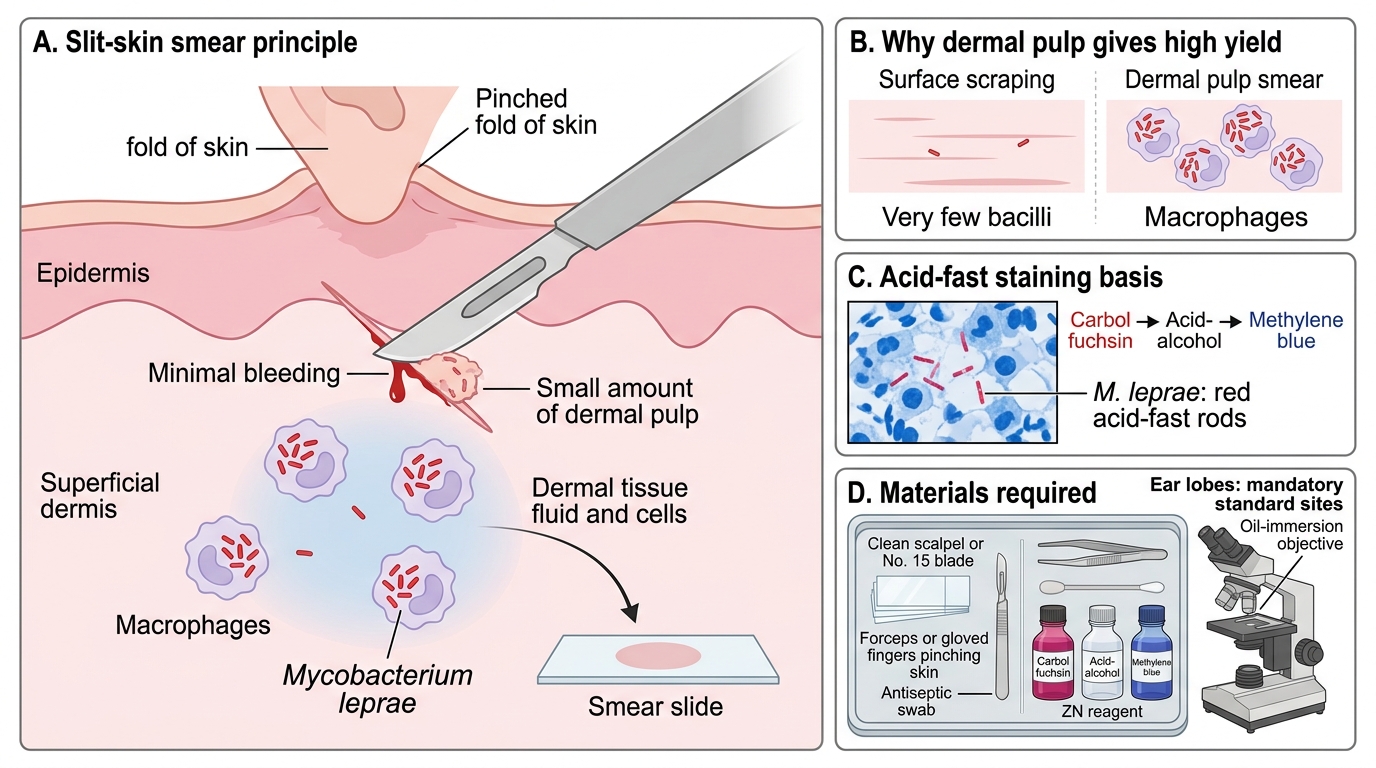
The principle of the slit-skin smear is to sample dermal tissue fluid and cells — where intracellular M. leprae reside within macrophages — and to demonstrate the bacilli microscopically using an acid-fast stain. Because the organism lives in the cooler, more superficial dermis and is carried in skin macrophages, a smear of dermal pulp (deliberately containing as little blood as possible) gives a far higher yield than a surface scraping or a blood smear. The staining basis is acid-fastness: after staining with carbol fuchsin, M. leprae resists decolourisation and retains the red dye, appearing as red rods against a blue counterstained background.
The Ziehl-Neelsen (ZN) stain is standard for skin smears, while the modified Fite-Faraco stain is preferred for tissue (biopsy) sections because M. leprae is less acid-fast than M. tuberculosis and the gentler decolourisation of the Fite method avoids washing the bacilli out. The materials required are simple and available even at a primary health centre: a clean scalpel or a small curved (No. 15) blade, glass slides, a pair of forceps or gloved fingers to pinch the skin, an antiseptic, carbol fuchsin and acid-alcohol and methylene blue (ZN reagents), and a microscope with an oil-immersion objective for reading. The ear lobes are mandatory standard sites because they are almost always involved in multibacillary disease and give a high yield; an active skin lesion is smeared in addition.
Materials and principle in brief:
- Sample dermal pulp (minimise blood) — bacilli live intracellularly in dermal macrophages.
- Stain by acid-fastness: Ziehl-Neelsen for smears (red bacilli on blue background); Fite-Faraco preferred for tissue sections.
- Read under the oil-immersion objective.
- Ear lobes are mandatory sites; add an active lesion.
Step-by-Step Procedure for Slit-Skin Smear Collection
Slit-Skin Smear Collection for Leprosy
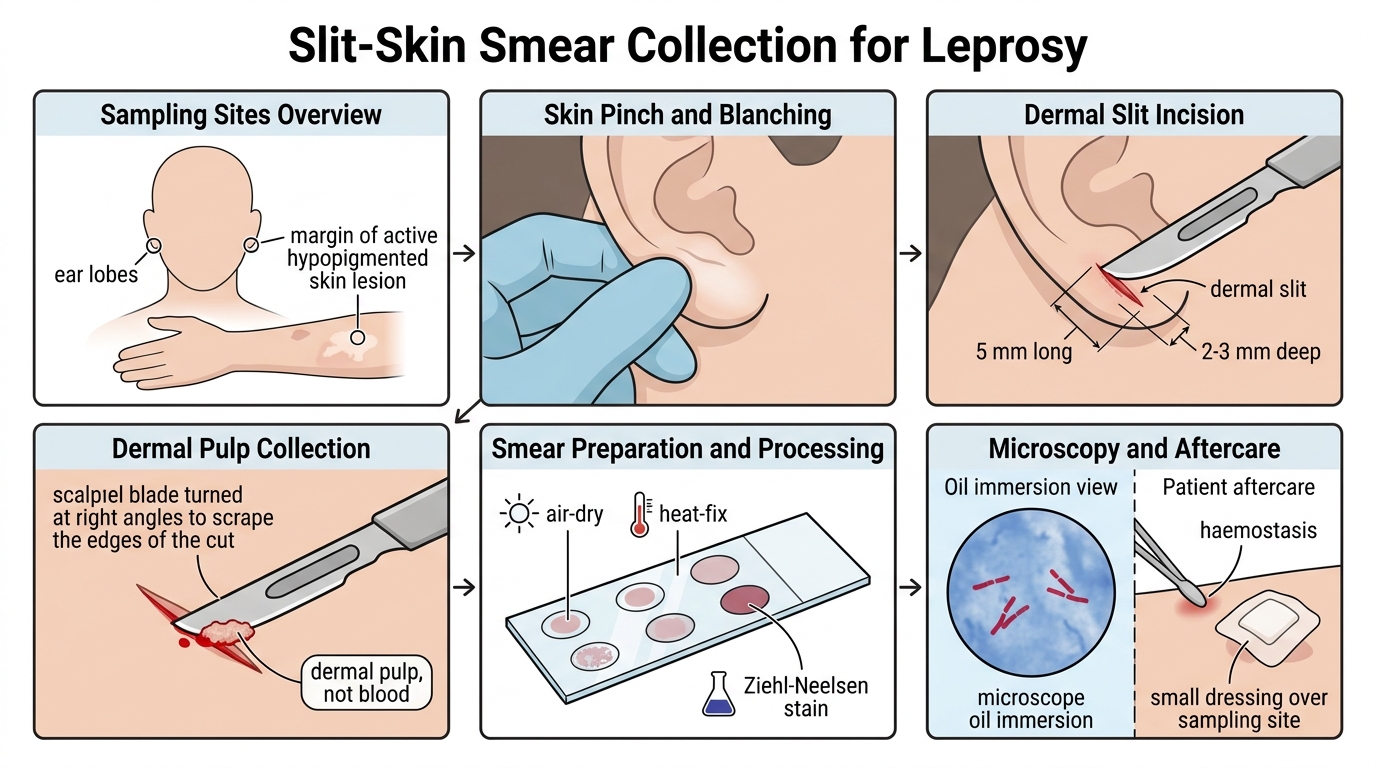
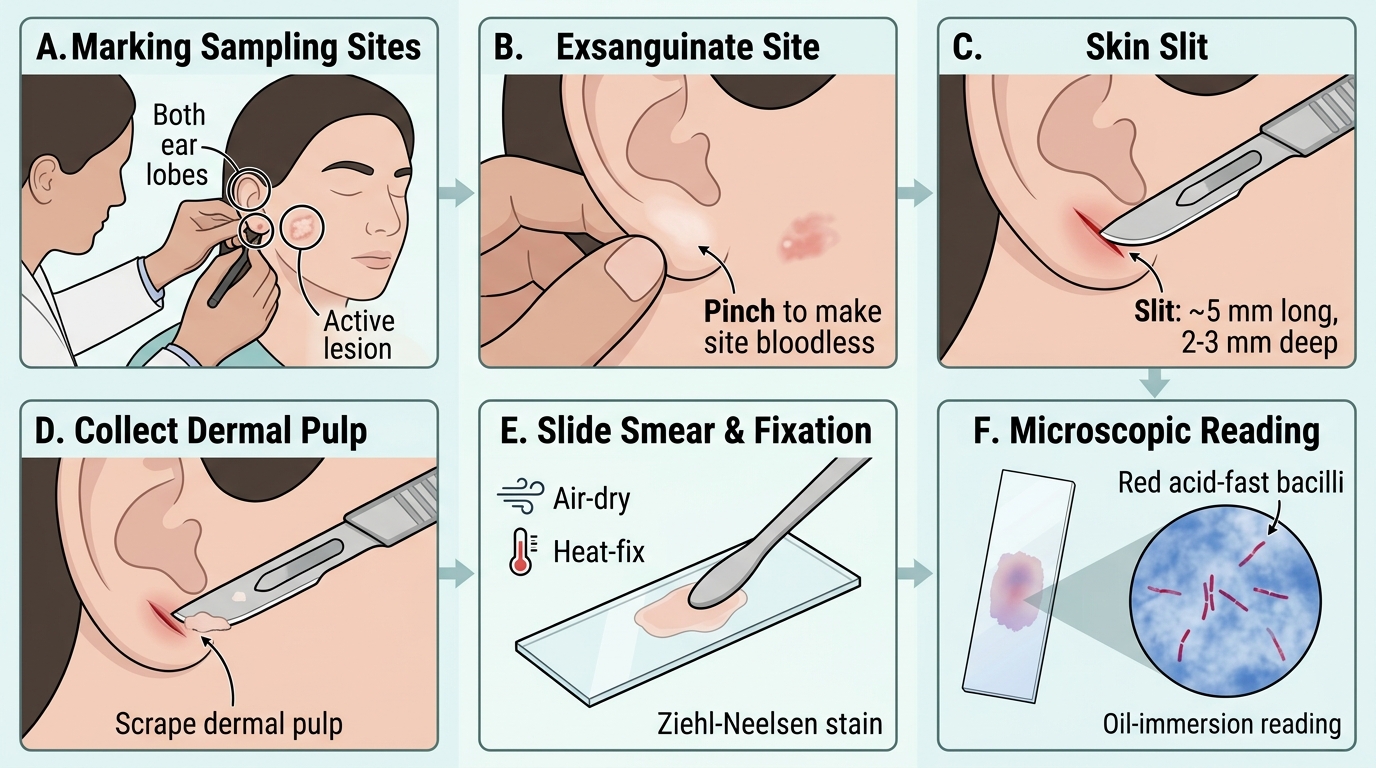
The technique of slit-skin smear collection is a short, reproducible sequence, and performing each step correctly is what determines whether the result is trustworthy. The aim throughout is to obtain dermal pulp with minimal blood contamination, because blood dilutes the specimen and lowers the apparent bacterial count. A minimum of about three sites is sampled — conventionally both ear lobes plus at least one active lesion — and up to six sites may be taken; each site is smeared onto a labelled slide.
The procedure runs as follows. Select and clean the site (ear lobe and an active lesion margin). Pinch the chosen fold of skin firmly between gloved finger and thumb (or forceps) and maintain the pinch throughout to squeeze the area bloodless so the incision bleeds as little as possible. With the pinch held, make a small incision about 5 mm long and 2-3 mm deep into the dermis with the scalpel. Turn the blade at right angles and scrape the cut edges to collect dermal pulp (tissue fluid and cells, not blood). Smear the collected pulp as a small circular film on a glass slide, allow it to air-dry, and heat-fix it. Stain by the Ziehl-Neelsen method and examine under oil immersion, reading multiple fields. Finally, attend to the patient — achieve haemostasis and apply a dressing — and label and transport the slides correctly.
Slit-Skin Smear Procedure for Leprosy
Sequence to memorise:
- Pinch to make the site bloodless → small slit (~5 mm long, 2-3 mm deep) → scrape dermal pulp → smear → air-dry → heat-fix → Ziehl-Neelsen stain → oil-immersion reading.
- Sample a minimum of ~3 sites (both ear lobes + an active lesion); minimise blood in every specimen.