Page 8 of 23
DR9.3 | Slit Skin Smear in Leprosy — SDL Guide (Part 2)
Interpreting the Smear — Bacteriological Index and Morphological Index
Interpreting Slit-Skin Smear: BI and MI
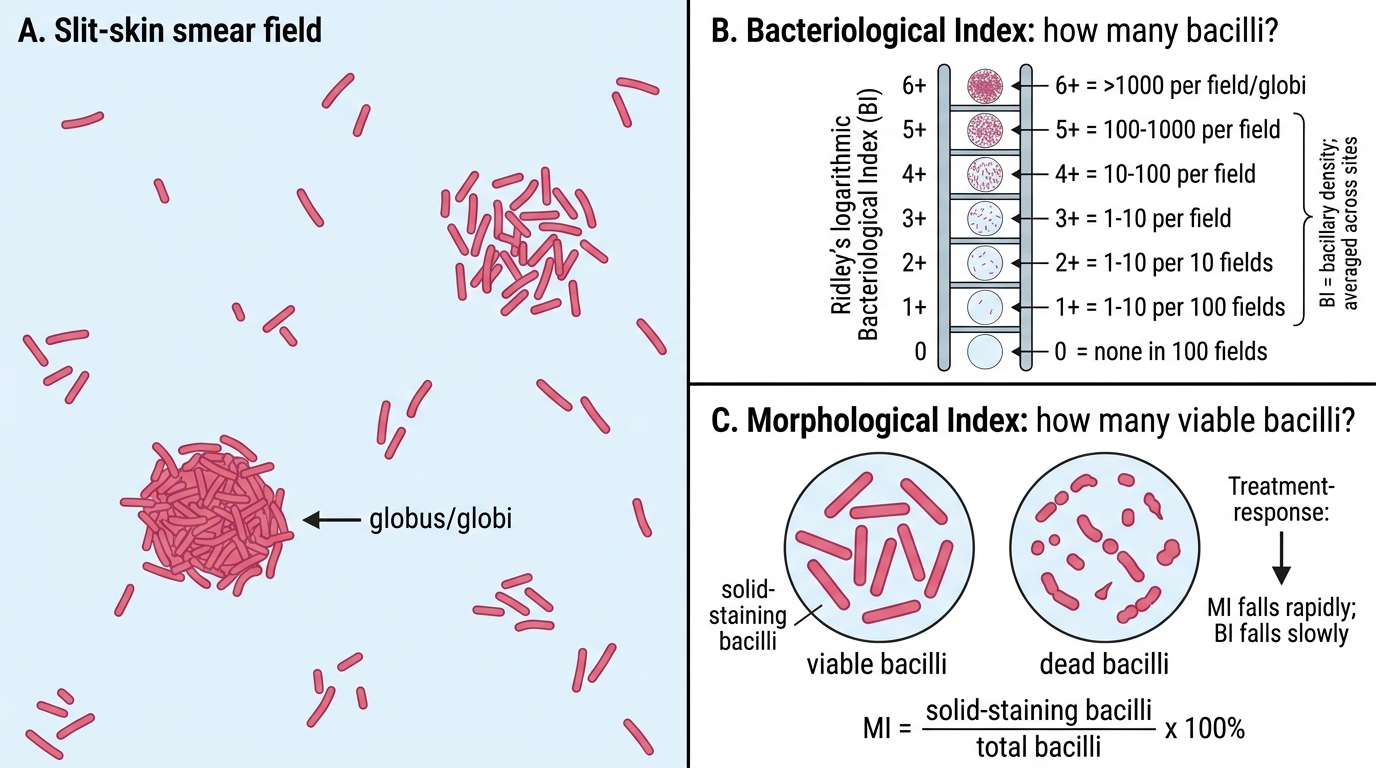
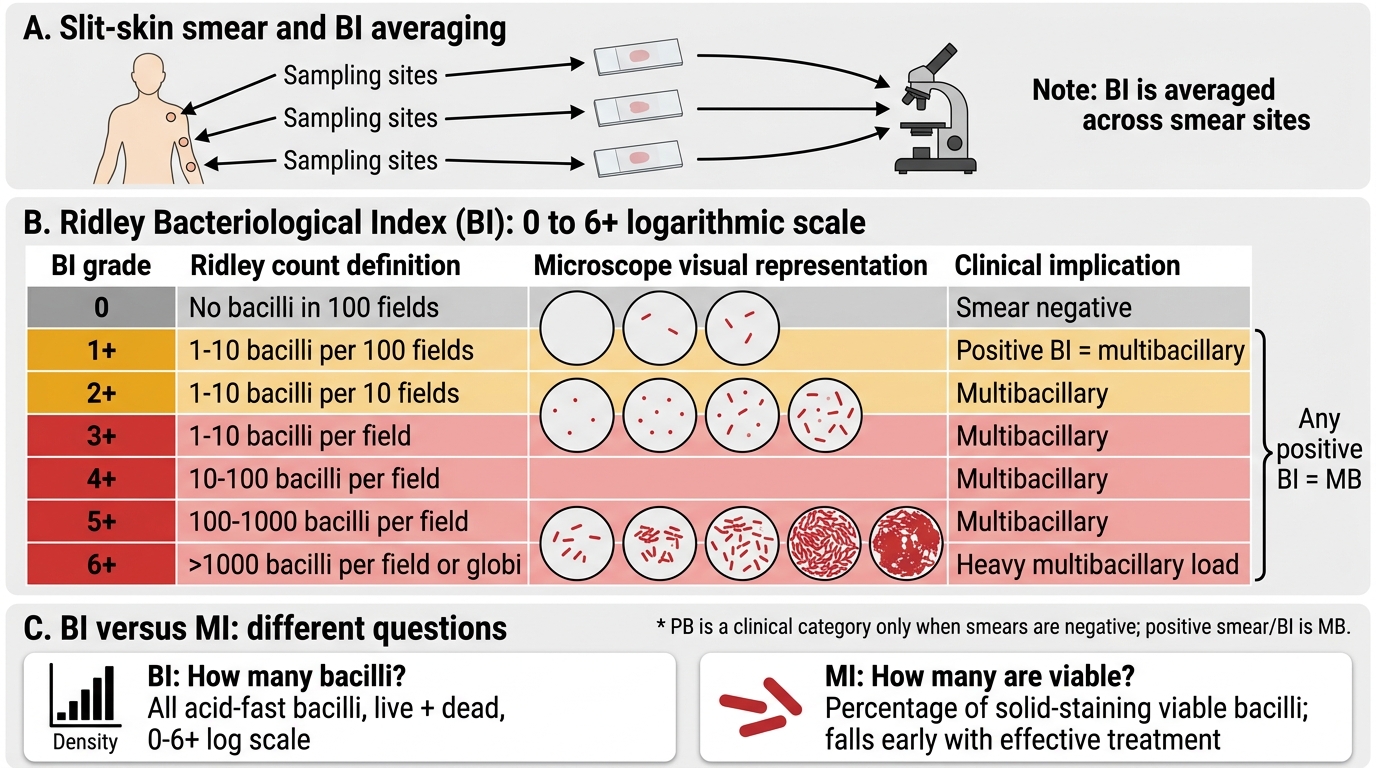
Interpreting a slit-skin smear means reading two indices that answer two different questions: how many bacilli are present, and how many of them are alive. The Bacteriological Index (BI) quantifies the density of acid-fast bacilli using Ridley's logarithmic scale from 0 to 6+, where each step represents roughly a tenfold change in bacillary density. A BI of 0 means no bacilli are seen in 100 oil-immersion fields; 1+ means 1-10 bacilli per 100 fields; 2+ means 1-10 per 10 fields; 3+ means 1-10 per field; 4+ means 10-100 per field; 5+ means 100-1000 per field; and 6+ means more than 1000 bacilli per field, often in clumps called globi. The BI is averaged across the sampled sites, and a smear-negative (BI 0 at all sites) result, combined with five or fewer lesions, supports a paucibacillary classification — whereas any positive BI makes the patient multibacillary.
The Morphological Index (MI) is the percentage of solid-staining (uniformly stained, intact) bacilli out of the total bacilli counted, and it estimates the proportion of viable organisms — dead bacilli stain irregularly, fragmented, or beaded. The MI is therefore a marker of bacterial viability and, historically, of treatment response and infectivity: with effective therapy the MI falls toward zero quickly even before the BI changes much, because rifampicin kills bacilli rapidly while their staining debris persists. In practice the MI is technically demanding and observer-dependent, so it is used less now than the BI, but its concept — distinguishing how many bacilli are present (BI) from how many are alive (MI) — remains important.
Ridley Bacteriological Index Grades in Leprosy
Key interpretation points:
- BI = bacillary density on a 0-6+ log scale; any positive BI = multibacillary; BI is averaged across sites.
- MI = percentage of solid-staining (viable) bacilli; estimates viability and falls early with effective treatment.
- BI measures how many bacilli; MI measures how many are alive — they answer different questions.
SELF-CHECK
What does the Morphological Index (MI) measure, and how does it differ from the Bacteriological Index (BI)?
A. MI measures the total number of bacilli on a 0-6 scale; BI measures the percentage that are dead
B. MI is the percentage of solid-staining (viable) bacilli, estimating viability; BI is the density of all acid-fast bacilli on Ridley's 0-6+ logarithmic scale
C. MI and BI measure the same thing using different stains
D. MI measures bacillary density and BI measures the depth of the skin incision
Reveal Answer
Answer: B. MI is the percentage of solid-staining (viable) bacilli, estimating viability; BI is the density of all acid-fast bacilli on Ridley's 0-6+ logarithmic scale
The Bacteriological Index (BI) measures the DENSITY of all acid-fast bacilli (live and dead) on Ridley's logarithmic 0 to 6+ scale. The Morphological Index (MI) is the PERCENTAGE of solid-staining, uniformly stained bacilli out of the total — these are the viable organisms, since dead bacilli stain irregularly or fragmented. So BI tells you how many bacilli are present, while MI tells you how many are alive. The MI falls early with effective treatment (rifampicin kills bacilli fast) even before the BI drops, because staining debris of dead bacilli persists.
Applied Practice — SSS in Diagnosis and Monitoring
Applied Use of Slit-Skin Smear BI in Leprosy
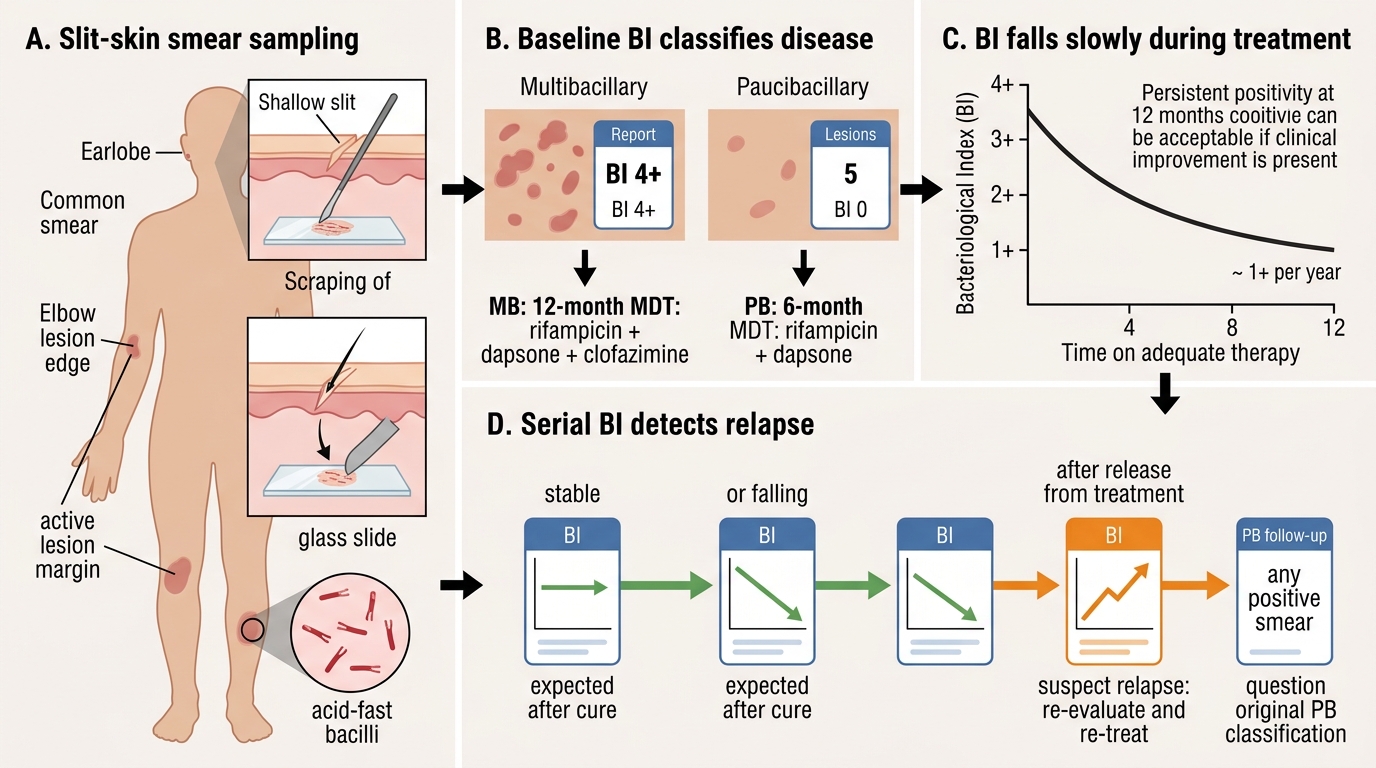
Applying the slit-skin smear in practice means translating index values into the same decisions you will make repeatedly: classify, treat, monitor, and detect relapse. At diagnosis, a baseline BI is recorded; a patient with, say, a BI of 4+ is unequivocally multibacillary and starts the 12-month rifampicin-dapsone-clofazimine regimen, while a patient with BI 0 at all sites and five or fewer lesions is paucibacillary and starts the 6-month rifampicin-dapsone regimen. During treatment, the expected trajectory is a gradual fall in the BI — conventionally on the order of about one unit (1+) per year of adequate therapy — so a high baseline BI may still be positive at the end of a 12-month course and that alone, with clinical improvement, is acceptable.
The smear is most powerful in surveillance after release from treatment. Because the BI falls slowly and predictably with cure, a BI that is rising on serial smears after a patient has completed and been released from treatment is a hallmark of relapse and prompts re-evaluation and re-treatment. A paucibacillary patient, by contrast, is expected to remain smear-negative throughout, so any positive smear during follow-up of a 'PB' patient should make you question the original classification. Throughout, results are documented and reported within the NLEP framework so that programme-level monitoring and relapse surveillance are possible.
Applied decisions from BI values:
- BI 0 (all sites) + ≤5 lesions → PB, rifampicin + dapsone × 6 months; expected to stay smear-negative.
- Any positive BI → MB, rifampicin + dapsone + clofazimine × 12 months; baseline BI recorded.
- BI falls ~1+ per year on adequate treatment; a rising BI after release from treatment suggests relapse.
Self-Assessment — Slit-Skin Smear
Consolidate this skill by reasoning from smear reports to clinical decisions, because the value of a slit-skin smear lies entirely in how you interpret and act on it. For each scenario below, move through a consistent chain of reasoning: what does the index value mean numerically, what WHO operational class does it imply, what treatment regimen and duration follow, and — if this is a follow-up smear — is the trajectory of the bacterial load reassuring or alarming? Keep separate in your mind the two questions the indices answer — the BI tells you how many bacilli are present, the MI how many are alive — and remember the single overriding rule that any positive smear means multibacillary disease.
Work through these checkpoints:
- A smear shows 10-100 acid-fast bacilli per oil-immersion field — state the BI grade and the WHO class it mandates, with the treatment regimen and duration.
- A patient who completed MB-MDT two years ago now has a BI that has risen from 1+ to 3+ on serial smears — what does this indicate and what is the next step?
- A patient clinically thought to be paucibacillary has a smear positive at the ear lobe — how does this change the classification and why?
- During treatment a patient's MI has fallen to near 0% while the BI is still 3+ — explain why both findings can be true at once and what it tells you about treatment response.
If you can convert each smear report into the correct classification, regimen, and follow-up judgement, you have met the objective of this module.
CLINICAL PEARL
One positive slit-skin smear at any site makes the patient multibacillary — full stop. No matter how few lesions a patient has, a positive smear commits them to the 12-month three-drug regimen; classifying on lesion count alone risks under-treatment and relapse. Take the ear lobes every time (they are almost always involved in MB disease) plus an active lesion, and squeeze the site bloodless before incising — blood dilutes the specimen and produces a falsely low or negative result, the commonest technical error. When reading reports, keep the two indices straight: the Bacteriological Index (Ridley 0-6+ log scale) tells you how many bacilli are present, while the Morphological Index (% solid-staining bacilli) tells you how many are alive. And in a treated, released patient, a rising BI on serial smears is the alarm bell for relapse.