Page 2 of 12
DR15.1-2 | Pyoderma Presentation and Antimicrobial Treatment — SDL Guide (Part 2)
Differential Diagnosis and Diagnostic Approach
Pyoderma: Mimics and When to Culture
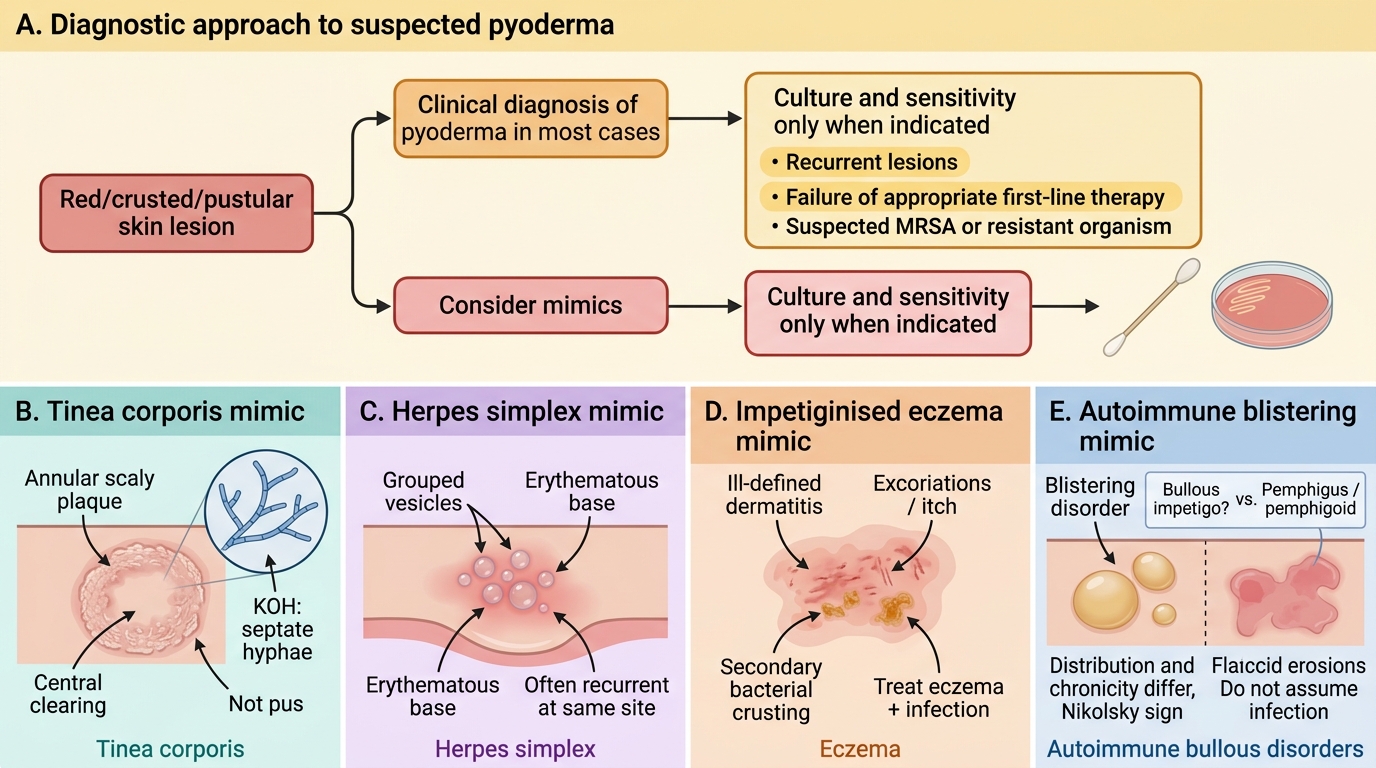
Because pyoderma is diagnosed clinically, the thoughtful clinician must hold a short differential in mind and also know the few specific situations in which a laboratory test genuinely changes management. Several common non-bacterial dermatoses can closely mimic pyoderma, and treating them with an antibiotic both fails the patient and needlessly wastes a drug while adding to resistance pressure. Equally, while the great majority of pyoderma needs no culture at all, certain high-risk situations — recurrence, failure of appropriate first-line therapy, or a reasonable suspicion of resistant organisms such as MRSA — do justify a swab for culture and sensitivity. The real skill, therefore, is knowing precisely when the test earns its place and changes what you will do, rather than ordering it reflexively for every red or crusted lesion you encounter. We will take the mimics first, then the indications to investigate.
Key mimics to consider and exclude:
- Tinea (dermatophyte): an annular scaly plaque with central clearing; KOH mount shows septate hyphae — not pus.
- Herpes simplex: grouped vesicles on an erythematous base, often recurrent at the same site.
- Eczema (impetiginised): itchy, ill-defined dermatitis that may become secondarily infected — treat the eczema as well as the infection.
- Pemphigus / bullous pemphigoid: blistering disorders that can resemble bullous impetigo; here the Nikolsky sign, distribution, and chronicity differ, and biopsy/immunofluorescence is diagnostic.
When to investigate (rather than treat empirically):
- Recurrent furunculosis or carbuncle → swab for culture and sensitivity; screen for nasal Staphylococcus aureus carriage.
- Treatment failure on appropriate first-line therapy → culture to detect resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA).
- Severe, systemic, or atypical disease → culture (and blood culture if toxic) before escalating therapy.
For MRSA, the laboratory should also perform a D-zone (induction) test before clindamycin is relied upon, because inducible clindamycin resistance can cause treatment failure even when the isolate appears clindamycin-susceptible on routine testing.
SELF-CHECK
A 30-year-old presents with a single annular, scaly plaque with raised edges and central clearing on the trunk; it itches and has slowly enlarged over weeks. The intern is about to prescribe oral cloxacillin for 'impetigo'. What is the most appropriate next step?
A. Start oral cloxacillin as planned for presumed pyoderma
B. Perform a KOH mount, because the annular scaly morphology suggests a dermatophyte (tinea), not a pyoderma
C. Start a systemic MRSA-active agent such as doxycycline empirically
D. Apply topical mupirocin and review in one week
Reveal Answer
Answer: B. Perform a KOH mount, because the annular scaly morphology suggests a dermatophyte (tinea), not a pyoderma
An annular, scaly plaque with central clearing and a raised active edge is the classic morphology of tinea (dermatophyte infection), not a pyoderma. A KOH mount showing septate hyphae confirms it. Treating tinea with an antibacterial — topical or systemic — fails the patient and contributes to antibiotic misuse; the correct management is an antifungal once KOH confirms the diagnosis.
Topical Antimicrobial Therapy: Indications and Adverse Reactions
Topical Antimicrobials in Superficial Pyoderma
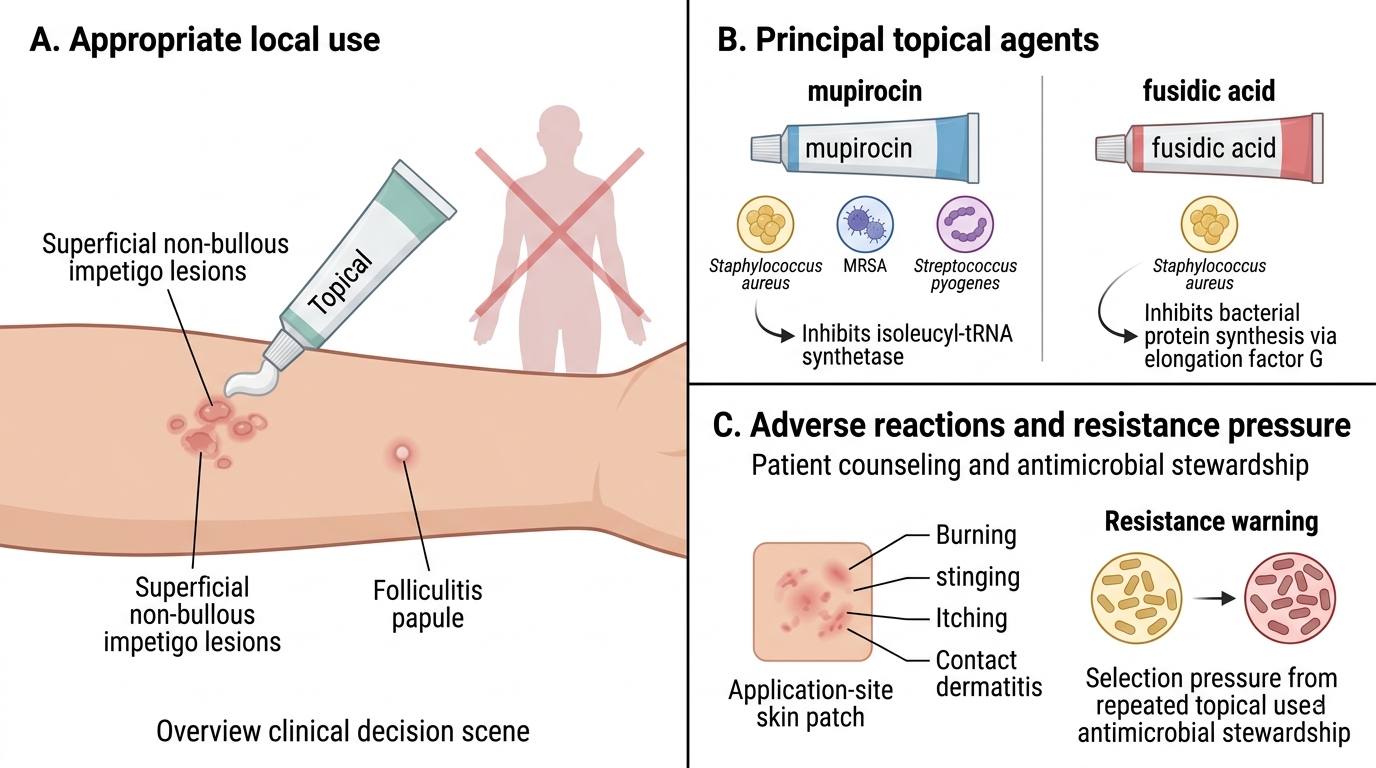
Topical antibiotics are the appropriate first-line treatment for localised, superficial pyoderma, where they deliver high local drug concentrations directly to the lesion while sparing the patient any systemic drug exposure. The two principal agents used in Indian practice are mupirocin and fusidic acid, and their place in therapy is limited but genuinely important. They are suited to a small number of superficial impetigo lesions, early localised folliculitis, and the eradication of nasal Staphylococcus aureus carriage in patients with recurrent disease. Beyond knowing their indications, the clinician must also know their adverse-reaction profile and the resistance pressures that limit their casual use, because the over-use of topical antibiotics is a recognised and increasingly important driver of resistance in skin flora. For each agent below, note both the situations in which it is appropriate and the harms you would counsel a patient to expect.
- Mupirocin — inhibits bacterial isoleucyl-tRNA synthetase; highly active against Staphylococcus aureus (including many MRSA strains) and Streptococcus pyogenes.
- Indications: localised non-bullous impetigo with few lesions; nasal decolonisation of Staphylococcus aureus in recurrent furunculosis.
- Adverse reactions: local burning, stinging, and itching at the application site; occasional contact sensitisation; emerging mupirocin resistance with widespread use limits empirical reliance.
- Fusidic acid — inhibits bacterial protein synthesis (elongation factor G); active mainly against Staphylococcus aureus.
- Indications: localised superficial staphylococcal pyoderma, including small impetigo and infected dermatitis.
- Adverse reactions: local irritation and contact dermatitis (a recognised risk with prolonged use); resistance develops readily, so courses should be short and combined with appropriate measures.
The governing rule is that topical therapy suits localised, superficial disease only; once lesions are numerous, deep, ulcerative, or accompanied by systemic features, you must switch to a systemic agent.
Systemic Antimicrobial Therapy: Drug Selection, Indications, and Adverse Reactions
Systemic Antimicrobial Therapy in Pyoderma
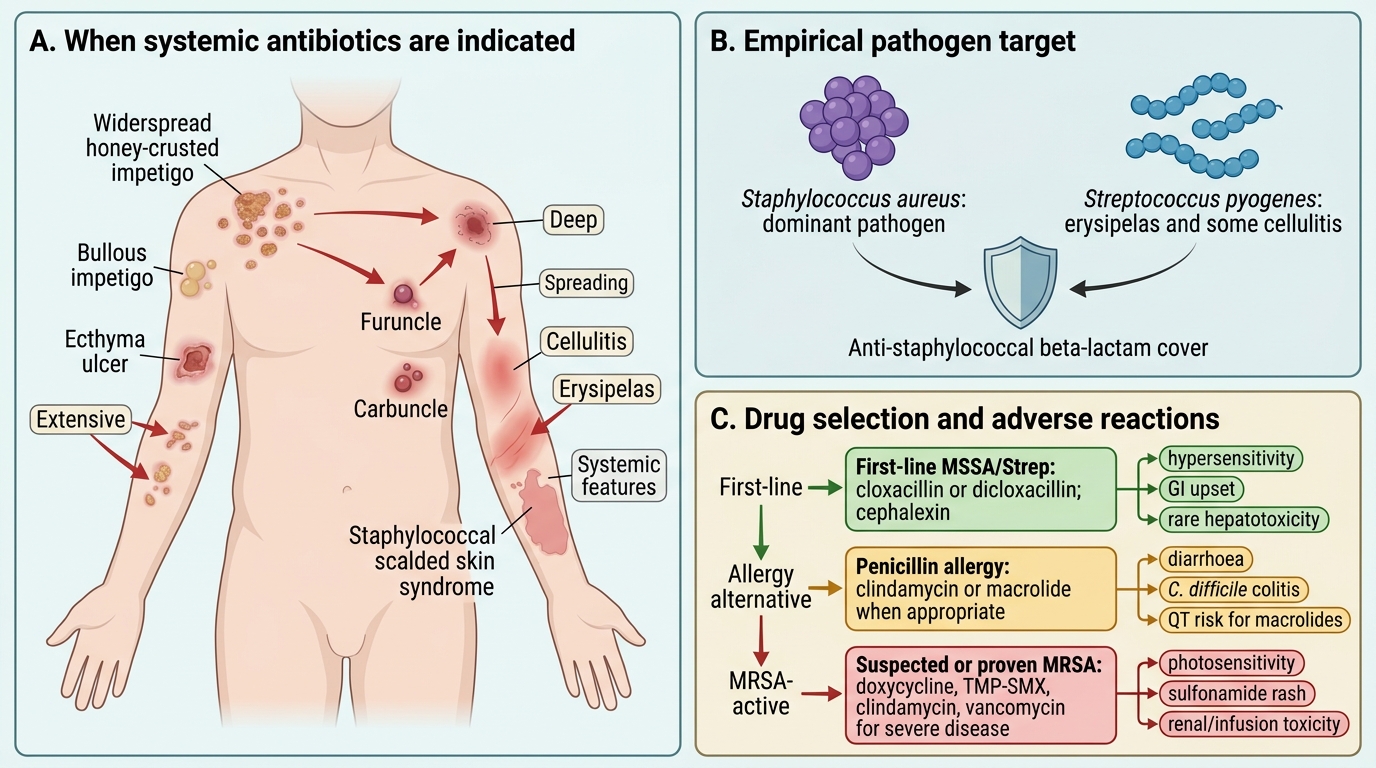
Systemic antibiotics are indicated whenever pyoderma is extensive, deep, spreading, or accompanied by systemic features — that is, for widespread or bullous impetigo, ecthyma, furuncle and carbuncle, all cellulitis and erysipelas, and staphylococcal scalded skin syndrome. Because Staphylococcus aureus is the dominant pathogen in most of these conditions (with Streptococcus pyogenes especially important in erysipelas and some cellulitis), empirical therapy centres firmly on anti-staphylococcal beta-lactams, with clearly defined alternatives reserved for penicillin allergy and for proven or suspected MRSA. The clinician must be able to enumerate, for each agent in turn, both its specific indication within pyoderma and its principal adverse reactions, because rational drug selection and properly informed consent both depend directly on holding this knowledge. The agents below are therefore grouped by the clinical situation that selects them — first-line, penicillin-allergic alternative, and MRSA-active — so that the list mirrors the decision you actually make.
First-line empirical agents (methicillin-susceptible Staphylococcus aureus and Streptococcus):
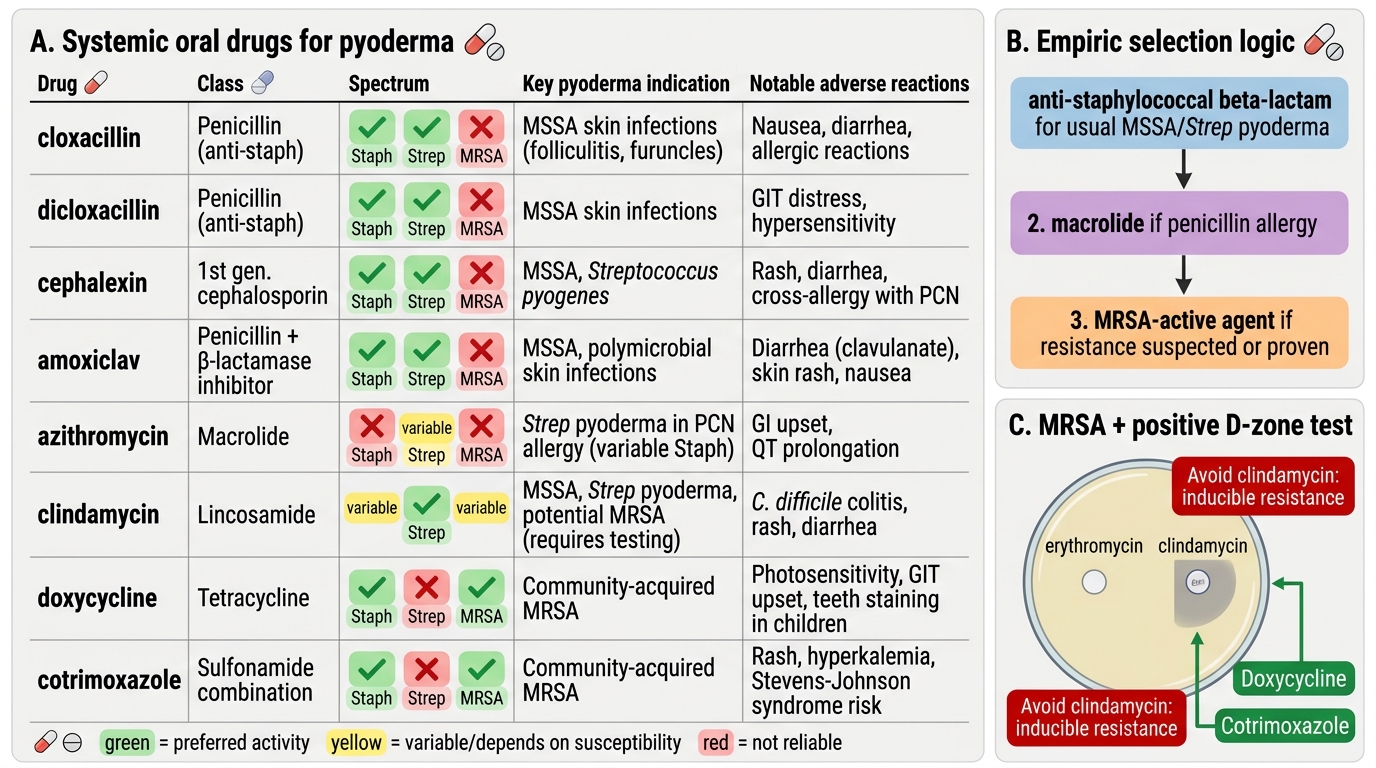
- Cloxacillin / dicloxacillin (penicillinase-resistant penicillins) — first-line for staphylococcal pyoderma. Adverse reactions: hypersensitivity (rash, and rarely anaphylaxis), gastrointestinal upset, and rare hepatotoxicity.
- Cephalexin (first-generation cephalosporin) — covers Staphylococcus and Streptococcus. Adverse reactions: hypersensitivity (with a small cross-reactivity risk in penicillin-allergic patients), gastrointestinal upset, and antibiotic-associated diarrhoea.
- Amoxicillin-clavulanate — broad spectrum including beta-lactamase-producing organisms, useful where mixed infection is likely. Adverse reactions: diarrhoea (notably from the clavulanate component), hypersensitivity, and hepatotoxicity.
For penicillin-allergic patients:
- Macrolides (erythromycin, azithromycin) — second-line alternatives. Adverse reactions: gastrointestinal intolerance (especially erythromycin), QT-interval prolongation, and hepatic enzyme interactions; rising macrolide resistance limits empirical use, so culture guidance is preferred where possible.
When MRSA is suspected or confirmed (recurrent disease, treatment failure, or local epidemiology), choose an MRSA-active oral agent:
- Clindamycin — active against many community-acquired MRSA strains. Adverse reactions: diarrhoea and, importantly, Clostridioides difficile colitis; confirm the D-zone test is negative before relying on it because of inducible resistance.
- Doxycycline — Adverse reactions: photosensitivity, gastrointestinal upset, and dental staining (contraindicated in young children and pregnancy).
- Cotrimoxazole (trimethoprim-sulfamethoxazole) — Adverse reactions: rash (including risk of severe cutaneous reactions), bone-marrow suppression, and hyperkalaemia; avoid in sulfonamide allergy.
Systemic Drugs for Pyoderma
The selection logic is therefore stepwise: anti-staphylococcal beta-lactam empirically; a macrolide if penicillin-allergic; and an MRSA-active agent (clindamycin, doxycycline, or cotrimoxazole) when resistance is suspected or proven.
SELF-CHECK
A young adult develops recurrent furunculosis. The most recent lesion was swabbed and grew Staphylococcus aureus reported as methicillin-resistant (MRSA), with the laboratory noting a positive D-zone test. Which oral agent should be avoided on the basis of that D-zone result, and what is the safer reasoning?
A. Avoid doxycycline, because the D-zone test predicts tetracycline resistance
B. Avoid clindamycin, because a positive D-zone test indicates inducible clindamycin resistance and treatment failure is likely; choose doxycycline or cotrimoxazole instead
C. Avoid cotrimoxazole, because the D-zone test indicates sulfonamide resistance
D. Avoid cloxacillin, but only because of penicillin allergy risk
Reveal Answer
Answer: B. Avoid clindamycin, because a positive D-zone test indicates inducible clindamycin resistance and treatment failure is likely; choose doxycycline or cotrimoxazole instead
A positive D-zone (induction) test signals inducible clindamycin resistance: the isolate may appear clindamycin-susceptible on routine testing but can develop resistance during therapy, leading to treatment failure. For community-acquired MRSA pyoderma with a positive D-zone, clindamycin should be avoided and an alternative MRSA-active oral agent — doxycycline or cotrimoxazole — selected, with attention to their own adverse-reaction profiles (photosensitivity/dental staining for doxycycline; rash and marrow suppression for cotrimoxazole).