Page 3 of 12
DR15.1-2 | Pyoderma Presentation and Antimicrobial Treatment — SDL Guide (Part 3)
Self-Assessment: Clinical Reasoning in Pyoderma
Clinical Reasoning in Pyoderma
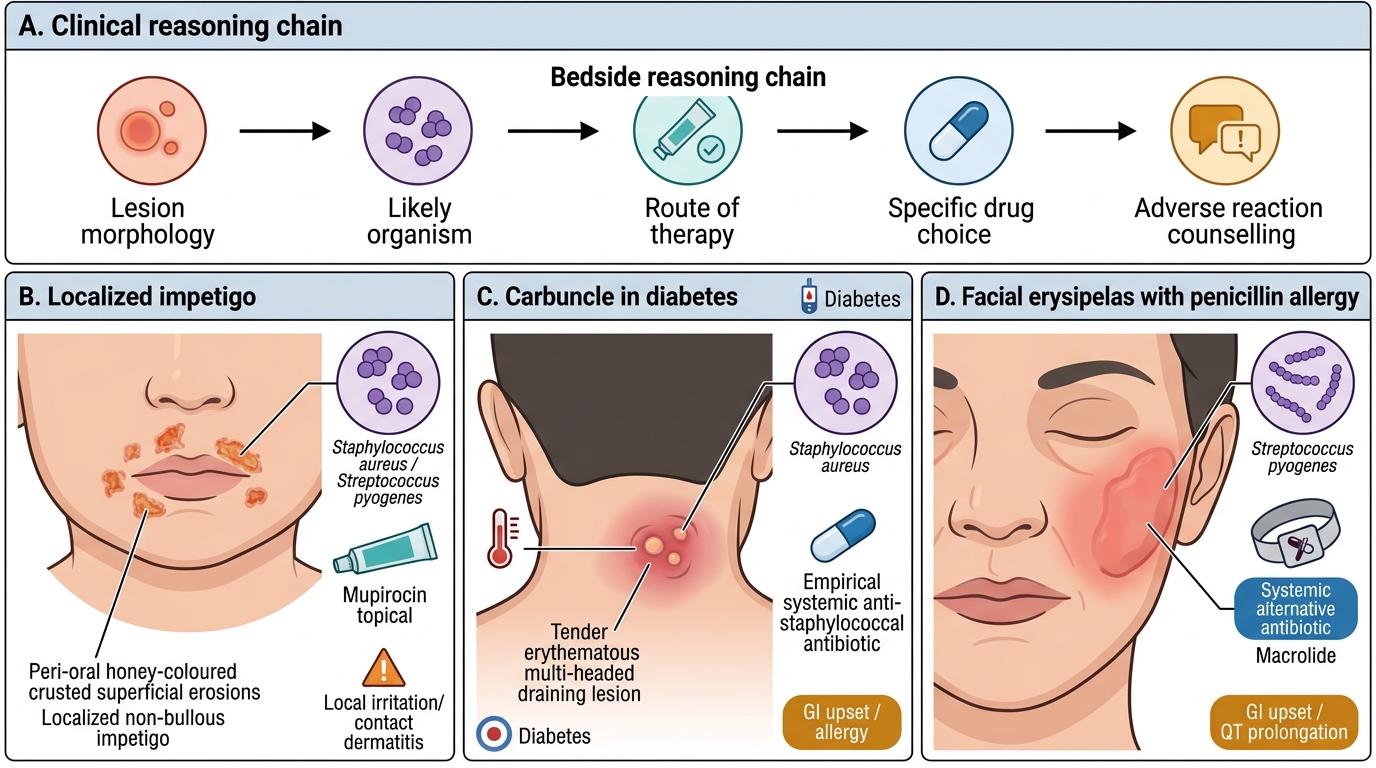
Consolidate your learning now by reasoning through the everyday decisions of pyoderma management, integrating morphology, likely organism, and rational drug choice into a single chain. The competency you are building here is deliberately twofold: first, to identify the clinical presentation of the various cutaneous bacterial infections accurately at the bedside, and second, to enumerate the indications and adverse reactions of the topical and systemic drugs used to treat them. Work through the prompts below as if a real patient were sitting in front of you, naming in turn the lesion, the most likely organism, the appropriate route of therapy, the specific drug you would choose, and the adverse reactions you would counsel the patient about. It is that integrated reasoning chain, rather than any list of isolated facts, that genuine clinical practice demands of you, and these prompts are designed to rehearse exactly that chain.
Use these self-check prompts:
- Given a child with peri-oral honey-coloured crusts and few lesions, what is the diagnosis, the likely organism, the appropriate route of therapy, and one adverse reaction of your chosen topical agent?
- Given a diabetic with a tender multi-headed lesion on the nape and fever, what is the diagnosis, and which systemic agent would you start empirically with what key adverse reaction?
- Given a penicillin-allergic patient with sharply-demarcated facial erysipelas, which systemic class is preferred and what adverse reaction must you watch for?
- Given recurrent furunculosis that fails cloxacillin, what organism do you now suspect, and which oral agents are appropriate — with their adverse reactions?
If you can answer all four fluently, linking what you see to what you prescribe and the harms you must counsel, you have met the learning objectives of this module.
CLINICAL PEARL
Margin and depth solve most spreading-infection dilemmas at the bedside. A sharply-demarcated, raised, hot red plaque on the face or leg with fever is erysipelas (Streptococcus pyogenes, upper dermis); an ill-defined, flat, deeper spreading erythema is cellulitis. The practical consequence: both need systemic therapy, but the streptococcal slant of erysipelas means a beta-lactam is excellent first-line, while cellulitis (more often staphylococcal) keeps anti-staphylococcal cover central. And whenever a 'cellulitis' is associated with pain out of proportion to the visible signs, crepitus, or rapid progression, stop and think necrotising infection — that is a surgical emergency, covered in the companion SDL on surgical referral.