Page 22 of 35
DR10.8-9 | Urethral Discharge Diagnosis and Syndromic Management — SDL Guide
Learning Objectives
- Recognise the clinical presentation of urethral discharge and the relevance of treating it promptly for STI control.
- Describe the etiology of gonococcal and non-gonococcal urethritis, including the causative organisms and their key microbiological features.
- Perform and interpret a urethral smear, distinguishing gonococcal from non-gonococcal urethritis.
- Apply NACO syndromic case management (Kit 1) to treat both organisms together, and counsel the patient and partner on prevention as per syndromic guidelines.
INSTRUCTIONS
Urethral discharge is one of the most common STI presentations you will meet, and its management embodies the core logic of syndromic care: because gonococcal and non-gonococcal urethritis frequently coexist and cannot be reliably separated on clinical grounds alone, NACO syndromic management treats both at the same first visit. This module combines the knowledge competency (etiology, diagnosis, and management of gonococcal and non-gonococcal urethritis, DR10.8) with the clinical skill of effectively managing and counselling a patient with urethral discharge (DR10.9). It also flags a growing public-health concern — rising gonococcal resistance to cephalosporins — that you will carry through your career.
References
- NACO National Guidelines on Prevention, Management and Control of STI/RTI (Syndromic Case Management, Urethral Discharge) (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, Gonococcal and Non-gonococcal Urethritis (textbook)
- IADVL Textbook of Dermatology, chapter on Gonococcal and Non-gonococcal Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 20-year-old man comes to the clinic embarrassed by a thick yellow discharge from his penis and a burning sensation when he passes urine. He is convinced a single tablet will fix it, and he wants to leave quickly. The temptation is to treat only what you can see — the purulent discharge that screams gonorrhoea. But if you treat the gonococcus alone, you will very likely undertreat a silent chlamydial co-infection riding alongside it, and the burning will persist or recur. This is the central lesson of urethral discharge management: you treat the syndrome, not the single organism you happen to suspect, because gonococcal and non-gonococcal urethritis travel together far more often than apart.
WHY THIS MATTERS
Urethral discharge is a high-frequency presentation in every STI clinic, and as a medical officer you will manage it independently and repeatedly. The two organisms behind it — Neisseria gonorrhoeae and Chlamydia trachomatis — are the two commonest bacterial STIs worldwide and a leading cause of preventable infertility, epididymo-orchitis, and onward transmission. Treating them correctly at the first visit, treating the partner, and counselling on prevention interrupts a transmission chain that otherwise propagates silently. Competency DR10.8 asks you to know the etiology, features, and management of gonococcal and non-gonococcal urethritis, and DR10.9 asks you to effectively manage and counsel a patient with urethral discharge per syndromic guidelines — together they define the complete knowledge-plus-skill package this module delivers.
RECALL
Recall from Year-1 Microbiology that Neisseria gonorrhoeae is a Gram-negative diplococcus and that Chlamydia trachomatis is an obligate intracellular bacterium with a biphasic life cycle (elementary and reticulate bodies) that does not Gram-stain. Recall the structure of the male and female lower urogenital tract, since urethral discharge in men has a counterpart in cervicitis in women — both covered by the same syndromic kit. You will also draw on the consent-and-chaperone discipline from DR10.4 before performing any urethral examination or smear.
Clinical Indication: Recognising Urethral Discharge in Practice
Recognising Urethral Discharge in Practice
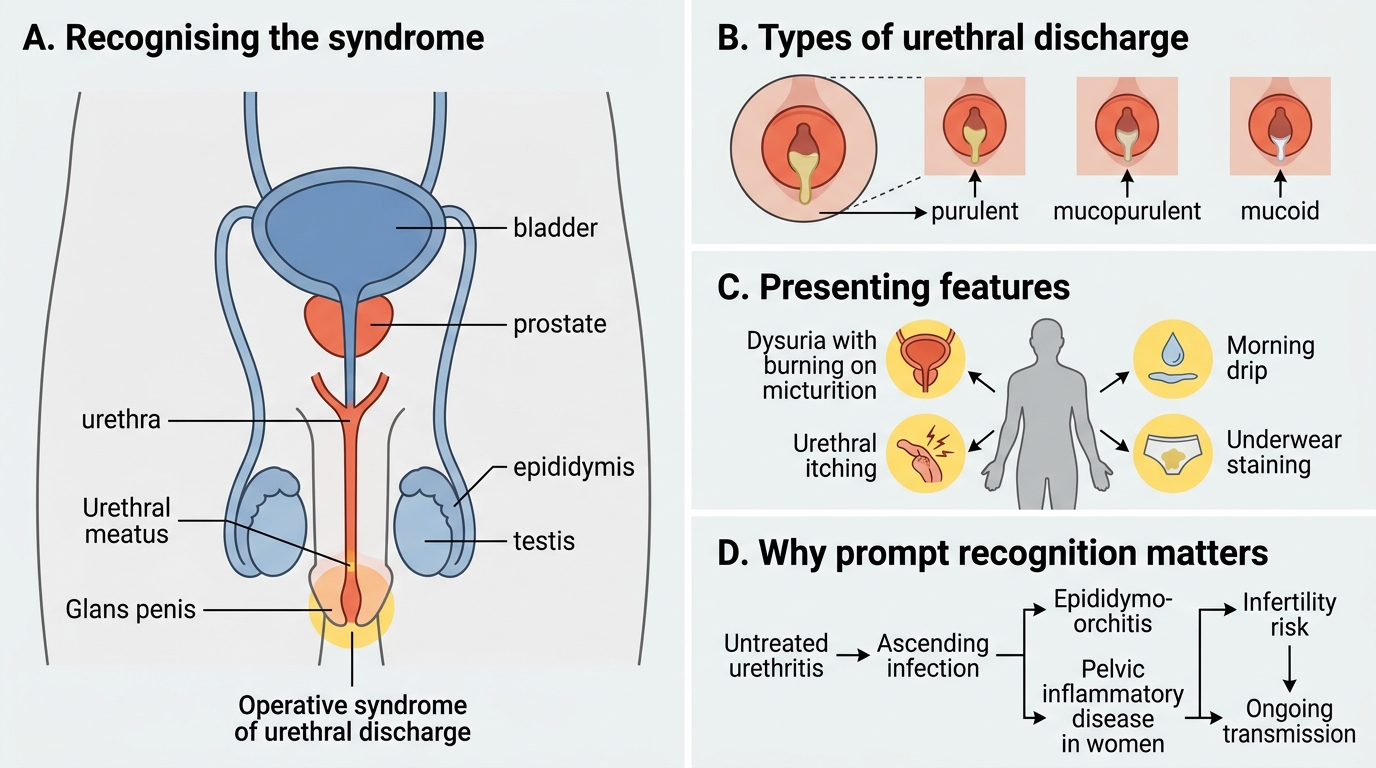
The first skill is recognising when urethral discharge is the operative syndrome, because patients describe it in many ways and some present obliquely. Typical presentations include a visible discharge from the urethral meatus (purulent, mucopurulent, or mucoid), staining of the underwear, dysuria (burning on micturition), and sometimes urethral itching or a 'morning drip'. The syndrome is common: gonococcal and chlamydial infections are the two most prevalent bacterial STIs globally, and in the Indian clinic context they constitute a major share of STI-clinic attendances. Recognising the syndrome promptly matters because untreated urethritis can ascend to cause epididymo-orchitis in men and pelvic inflammatory disease in women, both of which threaten fertility, and because every day of delay is a day of potential transmission. Approaching the patient without judgement — with the privacy and confidentiality framework already covered in DR10.4 — is what allows an honest history.
Presenting features to recognise:
- Visible urethral discharge (purulent, mucopurulent, or mucoid)
- Dysuria and urethral itching; 'morning drip' or underwear staining
- Common syndrome; complications include epididymo-orchitis and, in women, PID and infertility
Etiology and Pathophysiology of GC and NGU
Mechanisms of Gonococcal and Non-Gonococcal Urethritis
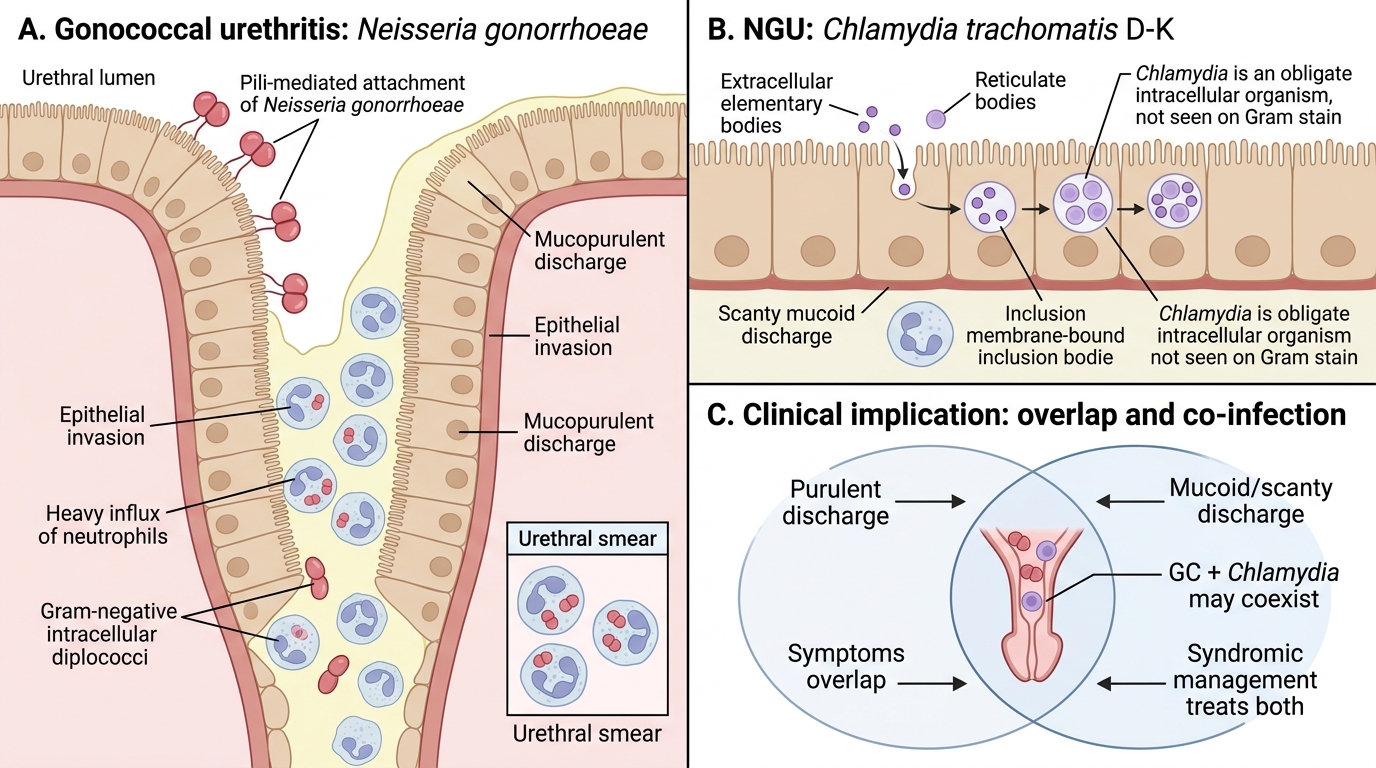
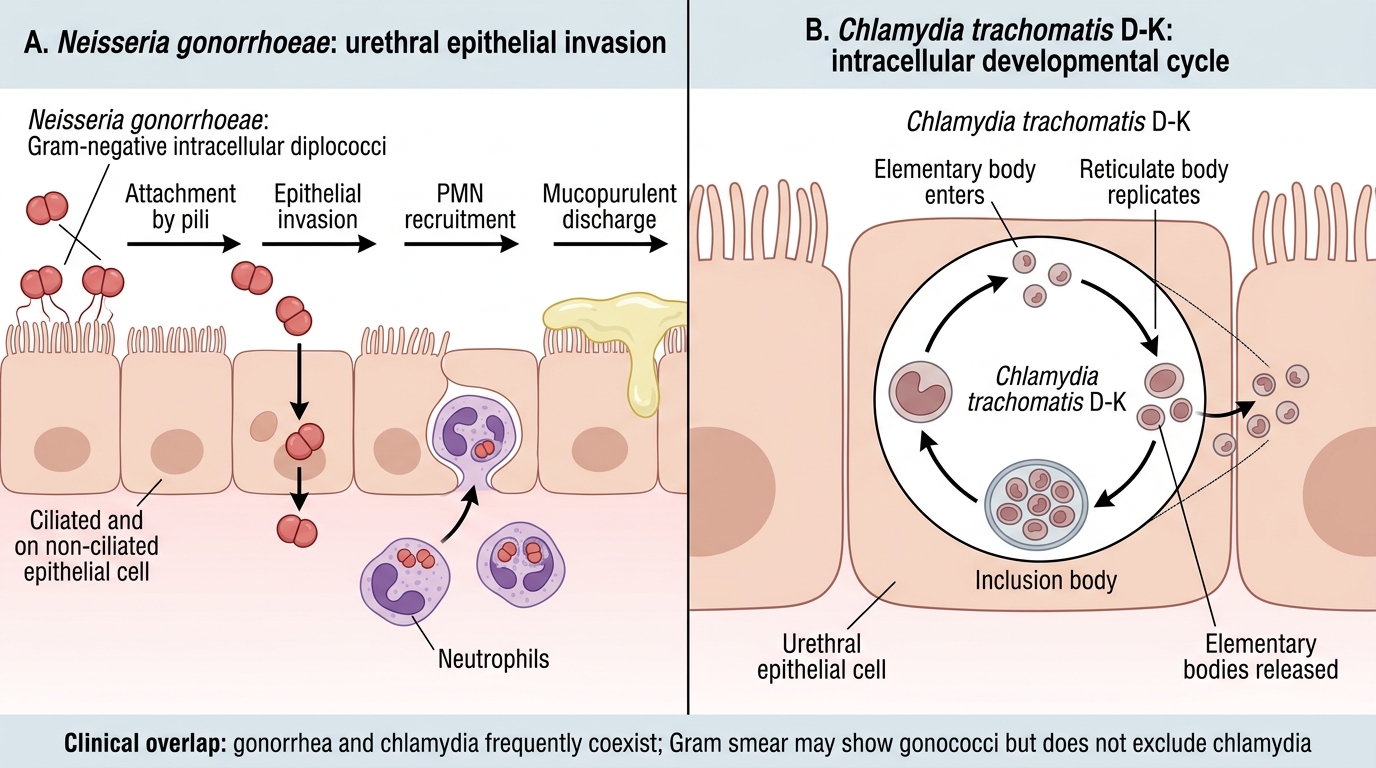
Understanding which organisms cause urethritis and how they injure the urethra is the principle that underpins both diagnosis and treatment. Gonococcal urethritis is caused by Neisseria gonorrhoeae, a Gram-negative organism classically seen as intracellular diplococci inside neutrophils on a urethral smear; it adheres to and invades the columnar epithelium of the urethra, provoking a brisk neutrophil response and the characteristic copious purulent discharge. Non-gonococcal urethritis (NGU) is caused predominantly by Chlamydia trachomatis serovars D-K — an obligate intracellular organism that cannot be Gram-stained — with Mycoplasma genitalium and Ureaplasma as further causes; NGU typically produces a more mucoid or scanty discharge with milder symptoms. Crucially, the two infections frequently coexist in the same patient, and clinical features overlap enough that you cannot reliably exclude chlamydial co-infection by looking at the discharge alone. This biological reality is precisely why syndromic management treats both together.
Mechanisms of Gonococcal and Chlamydial Urethritis
Etiology summary:
- Gonococcal: Neisseria gonorrhoeae — Gram-negative intracellular diplococci; copious purulent discharge
- NGU: Chlamydia trachomatis D-K (commonest), Mycoplasma genitalium, Ureaplasma; mucoid/scanty discharge
- GC and chlamydia frequently coexist; clinical features overlap
SELF-CHECK
On a Gram-stained urethral smear from a man with purulent discharge, you see Gram-negative diplococci inside neutrophils. What does this indicate, and why must you still treat for non-gonococcal urethritis as well?
A. Chlamydia trachomatis; no further cover is needed
B. Gonococcal urethritis (Neisseria gonorrhoeae); chlamydial co-infection is common and not excluded by the smear, so syndromic management treats both
C. Trichomonas vaginalis; treat with a single antifungal
D. A contaminant; reassure and discharge without treatment
Reveal Answer
Answer: B. Gonococcal urethritis (Neisseria gonorrhoeae); chlamydial co-infection is common and not excluded by the smear, so syndromic management treats both
Intracellular Gram-negative diplococci within neutrophils indicate gonococcal urethritis (Neisseria gonorrhoeae). Because Chlamydia trachomatis frequently co-infects and is not detectable on a Gram smear, NACO syndromic management (Kit 1) covers both organisms simultaneously rather than treating gonorrhoea alone.
History, Examination, and Smear Technique for Urethral Discharge
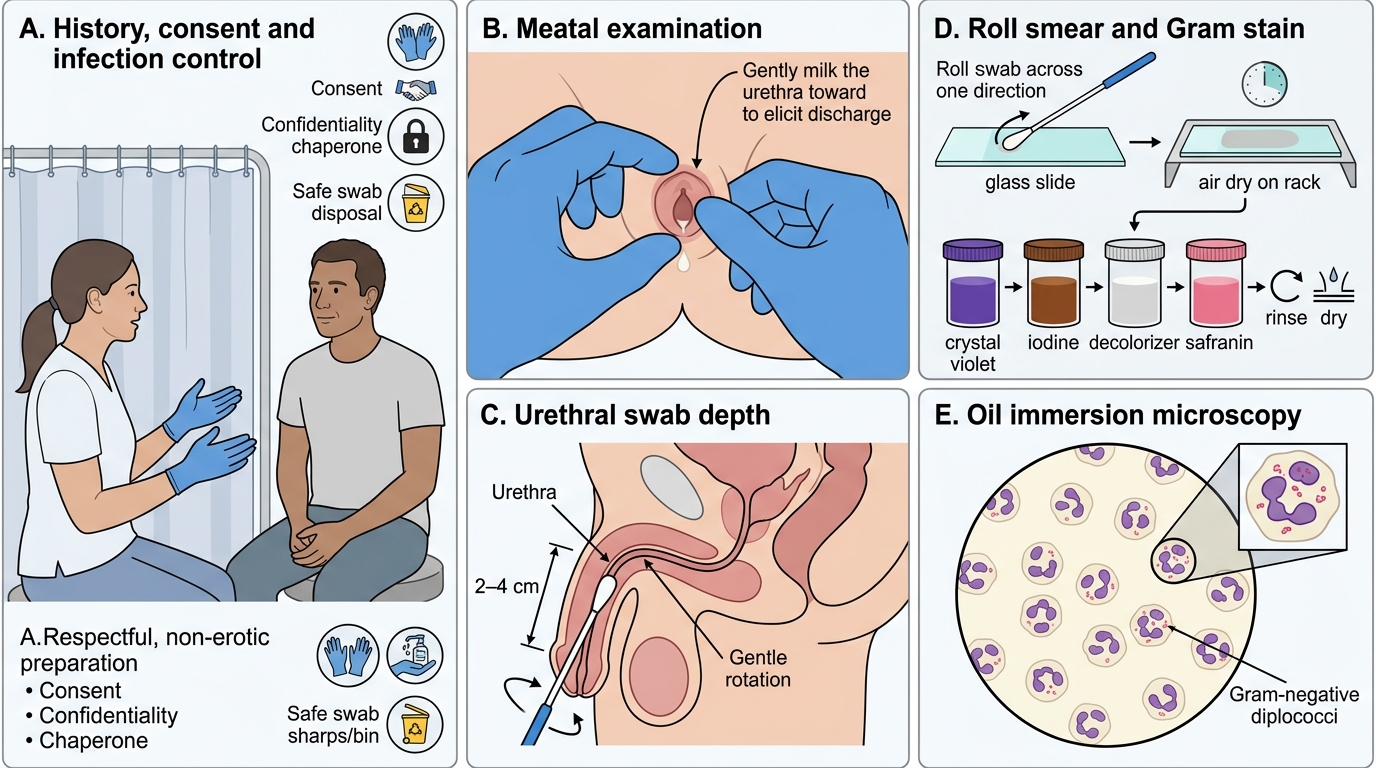
Urethral Discharge: History, Examination, Smear Technique, and Microscopy
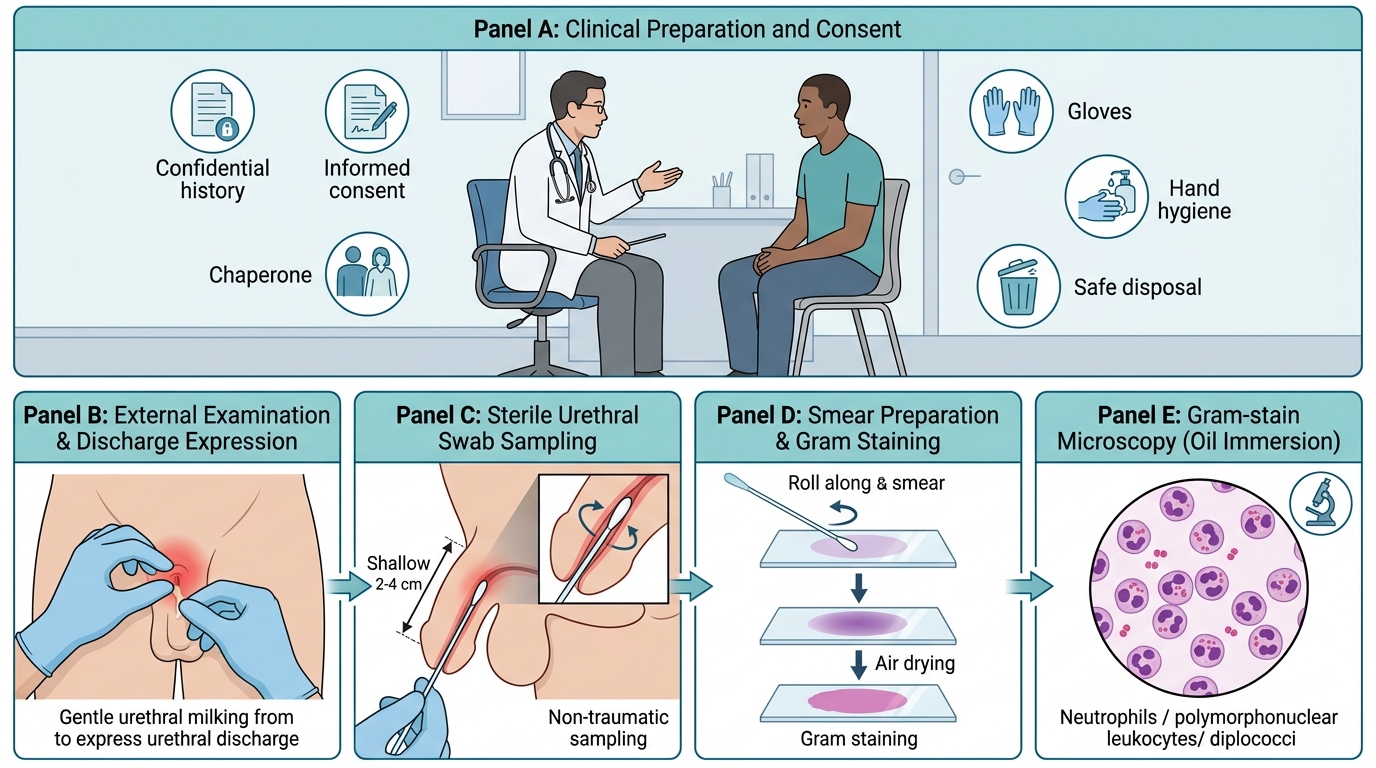
The procedural skill at the heart of this module is taking a focused history, examining correctly, and — where the facility allows — preparing and reading a urethral smear. Take a history of the discharge (onset, colour, amount), associated dysuria, recent sexual contacts and condom use, and any partner symptoms, all within the confidentiality framework. With consent and a chaperone, examine the urethral meatus and, if there is no spontaneous discharge, gently milk the urethra from base to tip to express a sample. To prepare the urethral smear, insert a fine swab a short distance into the anterior urethra, roll it onto a slide, allow it to air-dry, and Gram-stain it; under oil immersion you look for neutrophils (polymorphonuclear leukocytes) and for intracellular Gram-negative diplococci. Maintain infection control throughout — gloves, hand hygiene before and after, and safe disposal of the swab. Where smear facilities are unavailable, the syndromic approach proceeds on the clinical picture alone.
Urethral Smear Technique and Gram-Stain Microscopy
Technique steps:
1. Focused, confidential history; consent and chaperone
2. Examine meatus; milk the urethra if no spontaneous discharge
3. Roll swab onto slide, air-dry, Gram-stain, read under oil immersion
4. Infection control: gloves, hand hygiene, safe swab disposal