Page 23 of 35
DR10.8-9 | Urethral Discharge Diagnosis and Syndromic Management — SDL Guide (Part 2)
Interpretation of Clinical and Laboratory Findings
Interpretation of Urethral Smear and STI Laboratory Findings
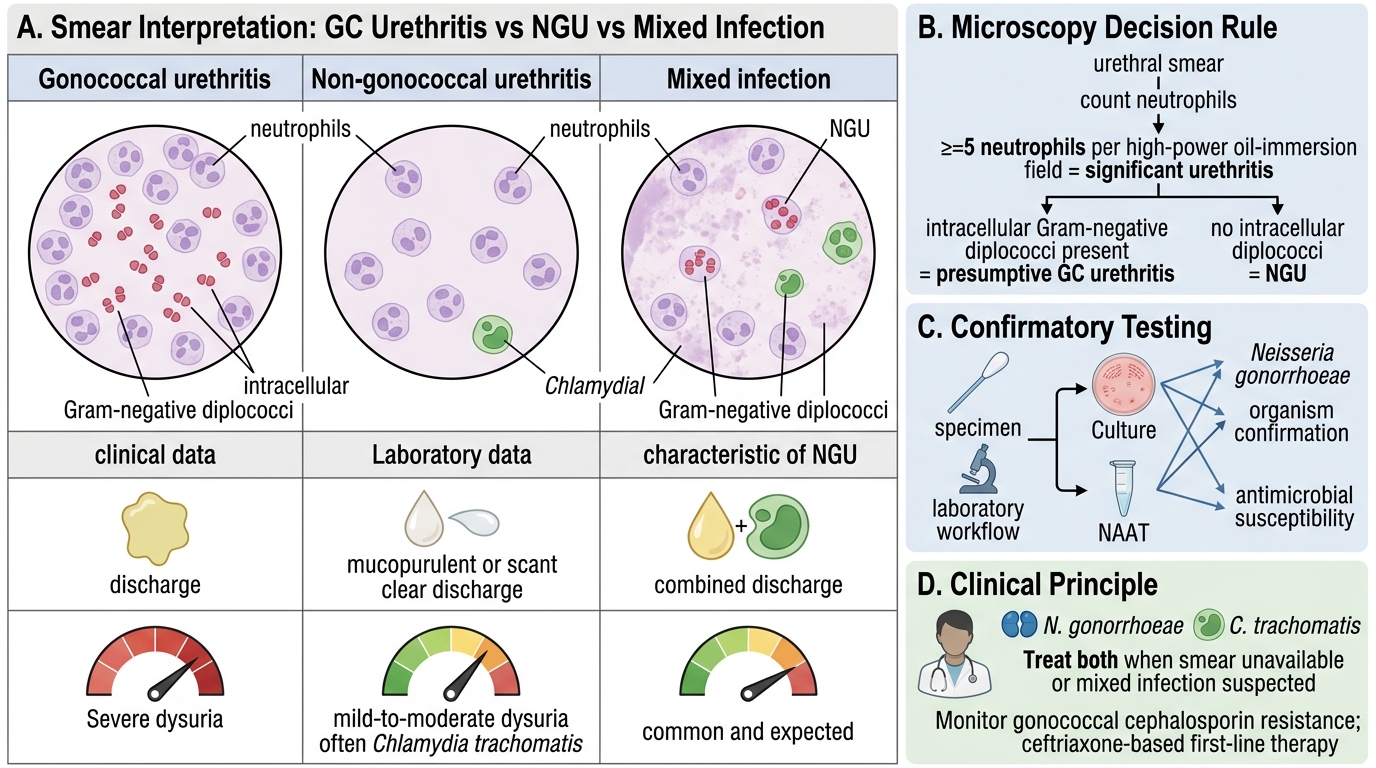
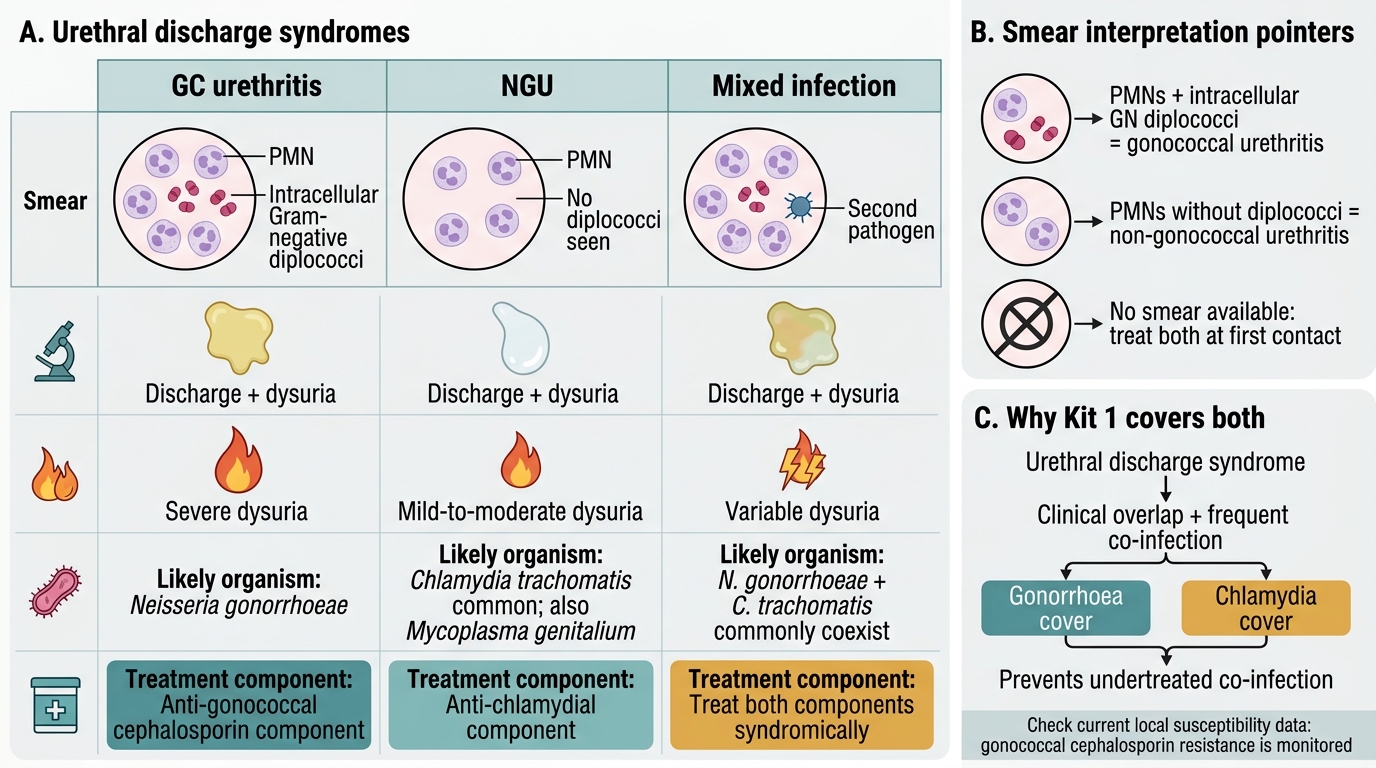
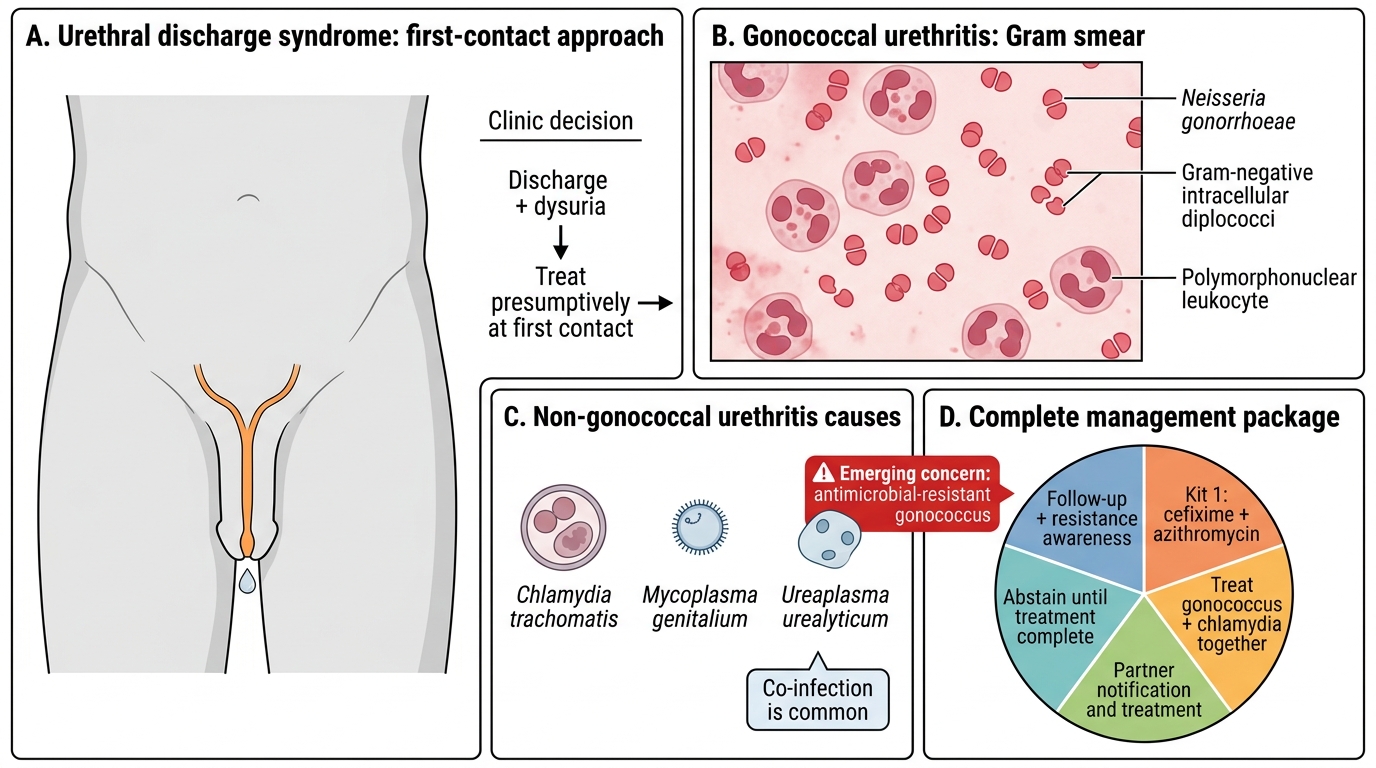
Interpreting the smear correctly tells you what you are dealing with, though it never changes the principle of treating both organisms. The presence of neutrophils with intracellular Gram-negative diplococci is a positive presumptive diagnosis of gonococcal urethritis; a threshold of about five or more neutrophils per high-power oil-immersion field supports significant urethritis. If you see neutrophils without intracellular diplococci, the picture is one of non-gonococcal urethritis, most often chlamydial. A mixed infection — both present — is common and expected. Where no smear is available, you treat syndromically for both. Culture or nucleic-acid amplification testing, where accessible, can confirm the organism and provide antimicrobial susceptibility, which matters because of the worsening trend of gonococcal resistance to cephalosporins documented by global surveillance (the WHO gonococcal antimicrobial surveillance programme); current first-line treatment remains ceftriaxone-based, but susceptibility must be monitored.
GC Urethritis vs NGU vs Mixed Infection
Interpretation pointers:
- PMNs + intracellular Gram-negative diplococci → gonococcal urethritis
- PMNs without diplococci → non-gonococcal (commonly chlamydial) urethritis
- Mixed infection common; no smear available → treat both syndromically
- Watch for rising gonococcal cephalosporin resistance (verify current susceptibility data)
SELF-CHECK
Why does NACO syndromic management of urethral discharge (Kit 1) routinely combine an agent against Neisseria gonorrhoeae with an agent against Chlamydia trachomatis?
A. Because the two drugs are cheaper when bought together
B. Because gonococcal and chlamydial infections frequently coexist and cannot be reliably separated clinically, so treating both at first contact prevents undertreated co-infection
C. Because chlamydia is resistant to all single agents
D. Because the gonococcus is always resistant to cephalosporins
Reveal Answer
Answer: B. Because gonococcal and chlamydial infections frequently coexist and cannot be reliably separated clinically, so treating both at first contact prevents undertreated co-infection
Gonococcal and chlamydial urethritis frequently coexist and overlap clinically, so syndromic management treats both at the first visit (e.g. cefixime or ceftriaxone for gonorrhoea plus azithromycin or doxycycline for chlamydia — per current NACO guidance). This prevents the common error of treating only the visible gonococcal infection and leaving chlamydia untreated.
Syndromic Management, Counselling, and Partner Treatment
Provided image
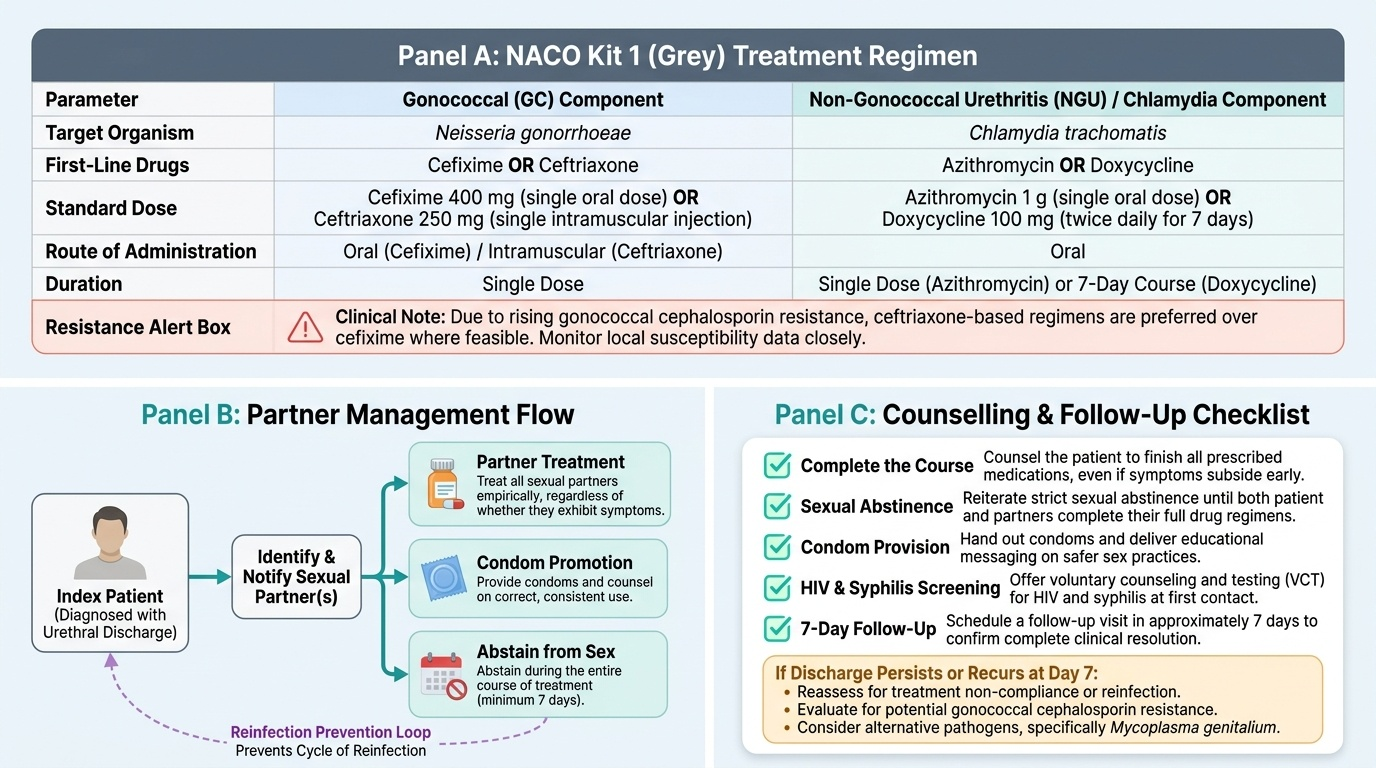
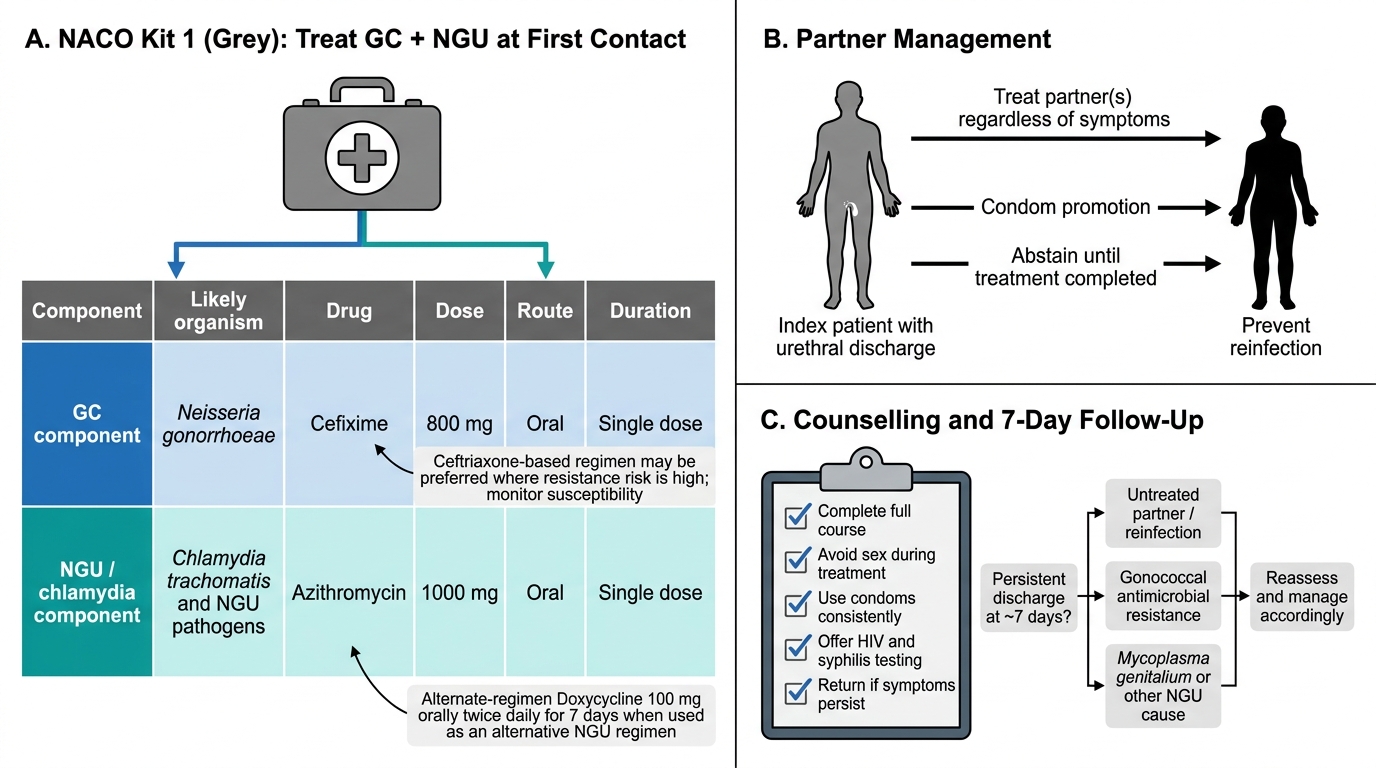
Applied management brings together drugs, partner treatment, and counselling into a single first-contact intervention, and under NACO this is Kit 1 (grey) — per current NACO guidance, with exact drugs and doses to be confirmed against the latest national protocol. The principle is to treat both organisms together at the first visit, without waiting for a smear result: an agent active against Neisseria gonorrhoeae (a cephalosporin such as cefixime or ceftriaxone) plus an agent active against Chlamydia trachomatis (azithromycin or doxycycline). Because gonococcal cephalosporin resistance is rising, ceftriaxone-based regimens are favoured and susceptibility should be monitored where data exist. Management is incomplete without the public-health package: treat the sexual partner(s) regardless of whether they have symptoms, promote and provide condoms, counsel the patient to complete the course and abstain from sex during treatment, offer HIV testing, and arrange follow-up (typically around 7 days) to confirm resolution. Persistent or recurrent discharge after correct treatment prompts reassessment for resistance, reinfection, or Mycoplasma genitalium.
NACO Kit 1 Grey: Urethral Discharge Management
Management essentials:
- NACO Kit 1 (grey): treat GC + chlamydia together at first contact (e.g. cefixime/ceftriaxone + azithromycin/doxycycline)
- Favour ceftriaxone-based regimens given rising gonococcal resistance; monitor susceptibility
- Treat partner(s) regardless of symptoms; promote condoms
- Counsel: complete course, abstain during treatment, offer HIV testing, follow up ~7 days
SELF-CHECK
A man treated for urethral discharge returns at 7 days with persistent symptoms despite confirming he completed his medication. Which considerations are most appropriate?
A. Reassure him it is psychological and discharge without action
B. Reassess for reinfection (untreated partner), gonococcal antimicrobial resistance, or Mycoplasma genitalium, and manage accordingly
C. Double the original antibiotic dose without any reassessment
D. Conclude the original diagnosis was wrong and stop all treatment
Reveal Answer
Answer: B. Reassess for reinfection (untreated partner), gonococcal antimicrobial resistance, or Mycoplasma genitalium, and manage accordingly
Persistent or recurrent discharge after correct treatment should prompt reassessment for reinfection from an untreated partner, rising gonococcal cephalosporin resistance, or Mycoplasma genitalium (which can resist standard NGU therapy). This is why partner treatment, counselling, and follow-up are integral to syndromic management.
Self-Assessment: Urethral Discharge Diagnosis and Management
Urethral Discharge: Diagnosis and Complete Management
Before finishing, assess your own command of both the knowledge and the skill, because urethral discharge is a syndrome where a single conceptual gap — forgetting the chlamydial co-infection — translates directly into undertreated patients and continued transmission. Work through the questions below as if you were running an STI clinic, articulating the organism, the smear finding, the kit, and the full counselling package for each. Give particular weight to the two ideas that learners most often drop under time pressure: that you treat both organisms together at first contact, and that partner treatment and follow-up are part of the treatment, not optional extras. Where an answer feels shaky, revisit the relevant section and rehearse it until the reasoning is automatic, because in a busy clinic you will fall back on whatever you have made second nature. Treat any uncertainty as a cue for revision, not a cause for concern.
Self-check questions:
- What organism causes gonococcal urethritis, and what is its appearance on a Gram smear?
- What are the common causes of non-gonococcal urethritis?
- Why does Kit 1 treat both organisms together?
- What is the public-health emerging concern about the gonococcus?
- What partner-treatment and counselling steps complete management?
CLINICAL PEARL
The most common avoidable error in urethral discharge is 'treating what you see' — giving a single shot for the obvious gonococcal discharge and never covering the silent chlamydial co-infection that recurs a week later. Always treat both. And when a patient returns with persistent discharge despite completing treatment, your first three thoughts should be reinfection from an untreated partner, rising gonococcal resistance, and Mycoplasma genitalium — in that order. Partner treatment is not an add-on; it is part of curing your patient.