Page 25 of 35
DR10.10 | Vaginal Discharge Syndromic Management — SDL Guide
Learning Objectives
- Distinguish pathological vaginal discharge from normal physiological discharge and recognise the clinical relevance of the three common causes.
- Apply the diagnostic principles — Amsel criteria, KOH mount, and saline wet preparation — to bacterial vaginosis, vulvovaginal candidiasis, and trichomoniasis.
- Perform the examination and the NACO risk-stratification step that decides between vaginal-discharge treatment alone and the addition of cervicitis cover.
- Apply NACO syndromic case management (Kit 2) and counsel correctly, including the differing partner-treatment rules for trichomoniasis and bacterial vaginosis.
INSTRUCTIONS
Vaginal discharge is a frequent reason women attend a clinic, and it is the syndrome where careful reasoning pays off most: three common causes — bacterial vaginosis, vulvovaginal candidiasis, and trichomoniasis — look superficially similar but differ in discharge character, pH, microscopy, treatment, and crucially in whether the partner must be treated. This module teaches you to diagnose and manage a woman presenting with vaginal discharge as per NACO syndromic guidelines (competency DR10.10), including the risk-stratification step that decides whether you must also cover cervicitis. Get the partner-treatment rule right: trichomoniasis needs partner treatment, bacterial vaginosis does not.
References
- NACO National Guidelines on Prevention, Management and Control of STI/RTI (Syndromic Case Management, Vaginal Discharge) (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, Vaginal Discharge syndromes (textbook)
- IADVL Textbook of Dermatology, chapter on Vaginal Discharge and Reproductive Tract Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old woman comes to the OPD distressed by a thin, greyish discharge with a fishy smell that worsens after intercourse. Her friend had something similar, was told it was a 'fungal infection', took an antifungal, and got no better. The friend's mistake is the lesson of this module: a fishy-smelling grey discharge is not candidiasis at all but bacterial vaginosis, and an antifungal will do nothing for it. Three common conditions produce vaginal discharge, they look deceptively alike at first glance, and they demand different treatments — and different decisions about whether to treat the partner. Reading the discharge, the pH, and the microscopy correctly is what separates a cure from a frustrated patient who keeps coming back.
WHY THIS MATTERS
Vaginal discharge is among the commonest presentations in women's health and a core NACO syndromic category you will manage independently. Beyond the immediate discomfort, the stakes are real: bacterial vaginosis is associated with preterm labour and increased HIV susceptibility, trichomoniasis facilitates HIV transmission and requires partner treatment to prevent ping-pong reinfection, and an underlying cervicitis from gonorrhoea or chlamydia — easily masked as 'just discharge' — can ascend to cause pelvic inflammatory disease and infertility. Competency DR10.10 asks you to diagnose and manage a woman with vaginal discharge per syndromic guidelines, which means not only treating the three vaginal causes but also performing the risk-stratification step that decides whether to add cervicitis cover. This is reasoning with direct fertility and public-health consequences.
RECALL
Recall from Year-1 Physiology that the normal vagina is colonised by Lactobacillus species, which ferment glycogen to lactic acid and keep the vaginal pH acidic (about 3.8-4.5), suppressing the overgrowth of other organisms. A rise in pH above 4.5 therefore signals a disturbed flora. Recall too that normal physiological discharge (leucorrhoea) is clear-to-white, non-malodorous, and varies with the menstrual cycle. You will also build on the consent-and-chaperone discipline from DR10.4, which is mandatory before any per-speculum vaginal examination.
Vaginal Discharge as a Clinical Indicator: When to Act
Vaginal Discharge: Clinical Indicators for Action
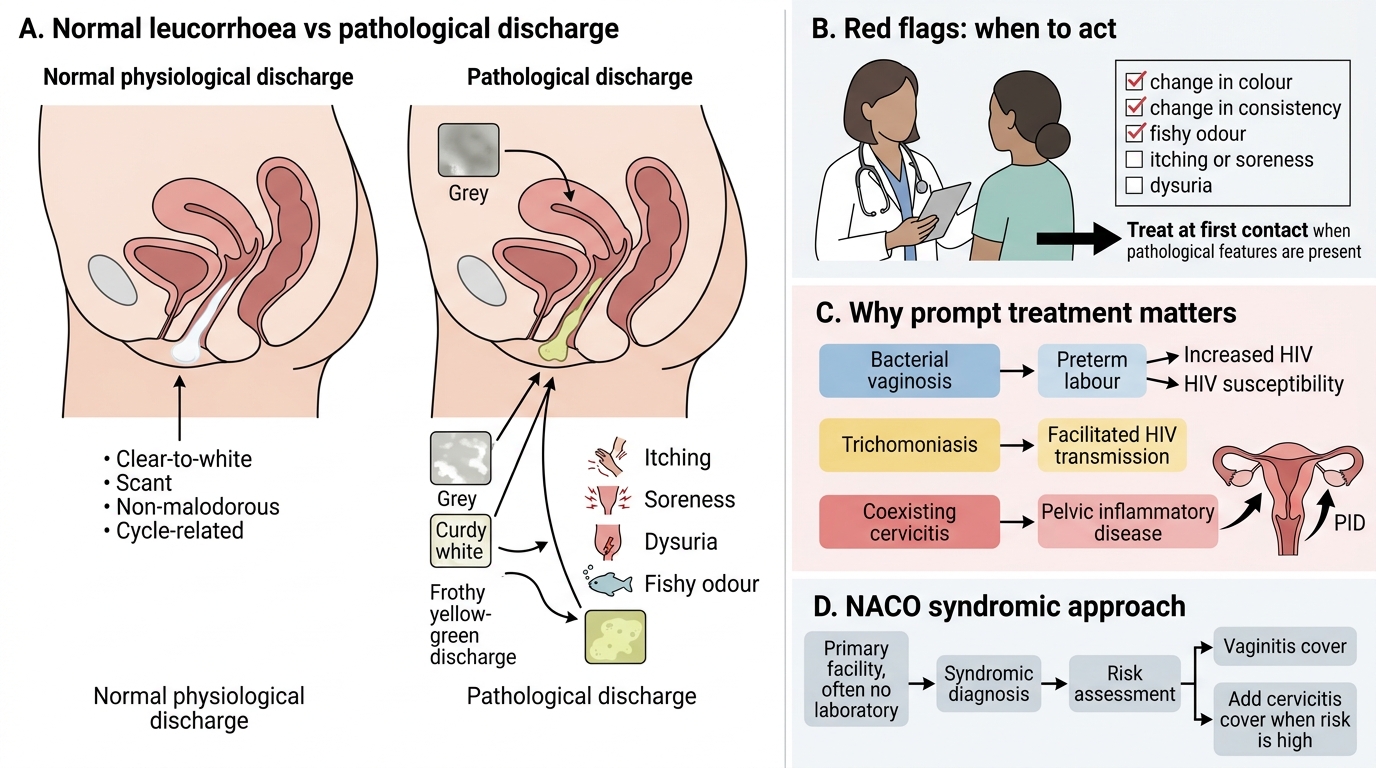
The first skill is distinguishing pathological discharge from normal leucorrhoea and recognising when to act. Pathological discharge is suggested by a change in colour (grey, curdy white, or frothy yellow-green), consistency, odour (especially fishy), or by associated symptoms such as itching, soreness, or dysuria. Normal physiological discharge, by contrast, is clear-to-white, non-malodorous, and fluctuates with the cycle. Acting promptly matters because the three common causes carry consequences beyond discomfort: bacterial vaginosis is linked to preterm labour and greater HIV susceptibility, trichomoniasis facilitates HIV transmission, and a coexisting cervicitis can ascend silently to pelvic inflammatory disease. The NACO syndromic approach exists precisely so that a clinician at a primary facility — often without a laboratory — can diagnose and treat effectively at first contact, while applying a structured risk assessment to decide how much cover the patient needs.
Features that flag pathological discharge:
- Change in colour, consistency, or odour (fishy odour is notable)
- Itching, soreness, dysuria
- Normal leucorrhoea is clear-to-white, non-malodorous, cycle-related
Diagnostic Principles: Amsel Criteria, KOH Mount, and Wet Preparation
Bedside Diagnosis of Vaginal Discharge
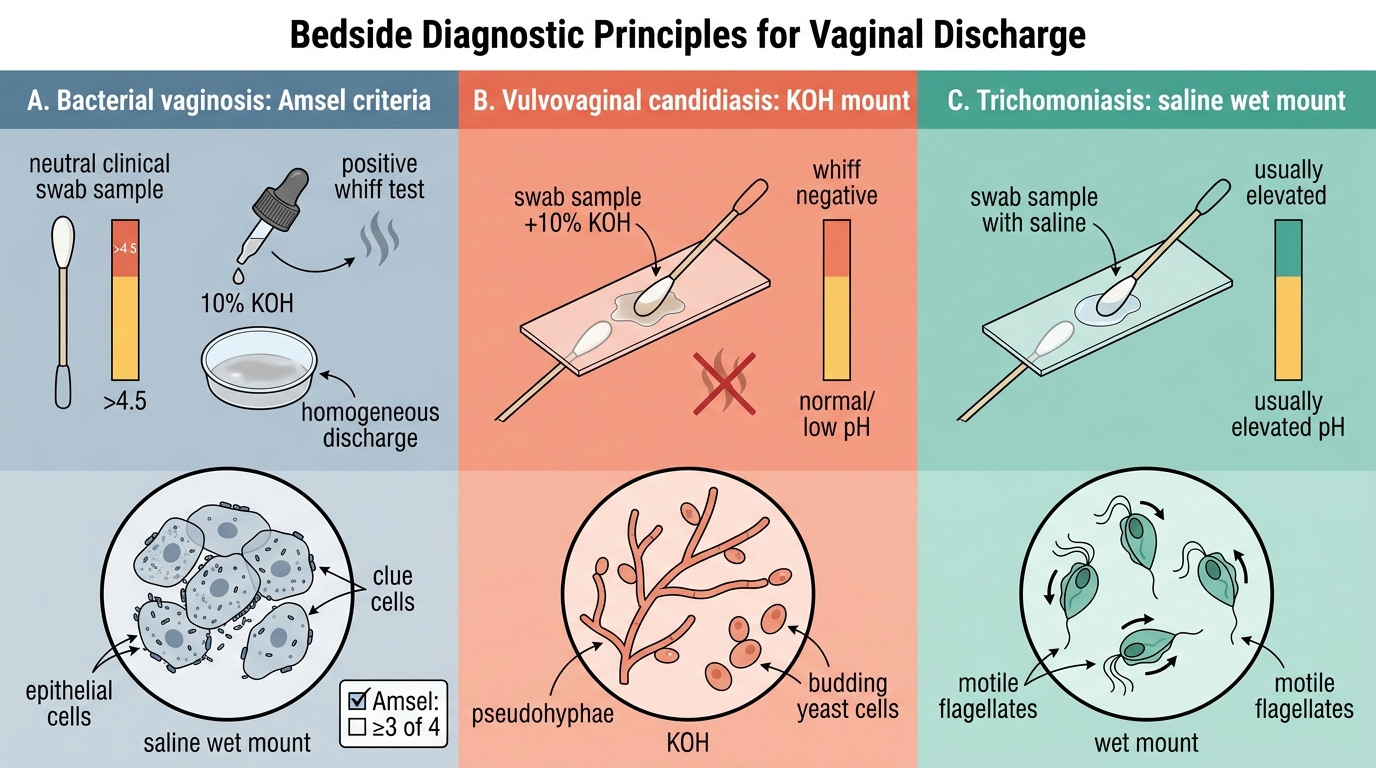
The principles that let you separate the three causes are a small set of bedside tests, each grounded in the underlying pathology. Bacterial vaginosis is a polymicrobial dysbiosis in which Lactobacillus is replaced by Gardnerella and anaerobes; it is diagnosed by the Amsel criteria — at least three of four: a thin grey homogeneous discharge, vaginal pH above 4.5, a positive amine (whiff) test (a fishy odour, classically on adding 10% KOH, from the polyamines produced by the altered flora), and clue cells on a saline wet mount. Vulvovaginal candidiasis is an overgrowth of Candida albicans; a KOH mount dissolves host cells and reveals pseudohyphae and budding yeast, with a normal or low pH and a negative whiff test. Trichomoniasis is caused by the flagellated protozoan Trichomonas vaginalis; a saline wet mount shows motile, pear-shaped flagellates, usually with an elevated pH. Knowing which test answers which question is the core diagnostic skill.
Diagnostic toolkit:
- BV: Amsel criteria (≥3 of 4) — grey discharge, pH >4.5, positive whiff test, clue cells
- Candidiasis: KOH mount → pseudohyphae + budding yeast; normal/low pH; whiff negative
- Trichomoniasis: saline wet mount → motile flagellates; usually elevated pH
SELF-CHECK
A woman has a thin grey homogeneous discharge, vaginal pH of 5.0, a positive whiff test, and clue cells on wet mount. What is the diagnosis, and is partner treatment routinely required?
A. Vulvovaginal candidiasis; treat the partner routinely
B. Bacterial vaginosis; partner treatment is NOT routinely recommended
C. Trichomoniasis; partner treatment is required
D. Normal physiological discharge; no treatment at all
Reveal Answer
Answer: B. Bacterial vaginosis; partner treatment is NOT routinely recommended
Thin grey discharge, pH >4.5, positive whiff test, and clue cells (three or more Amsel criteria) diagnose bacterial vaginosis. BV is treated with metronidazole, and partner treatment is NOT routinely recommended (unlike trichomoniasis, where partner treatment is required). Candidiasis shows pseudohyphae on KOH with a normal pH and negative whiff test.
Examination Technique, Specimen Collection, and NACO Risk Stratification
NACO Vaginal Discharge Examination and Risk Stratification Algorithm
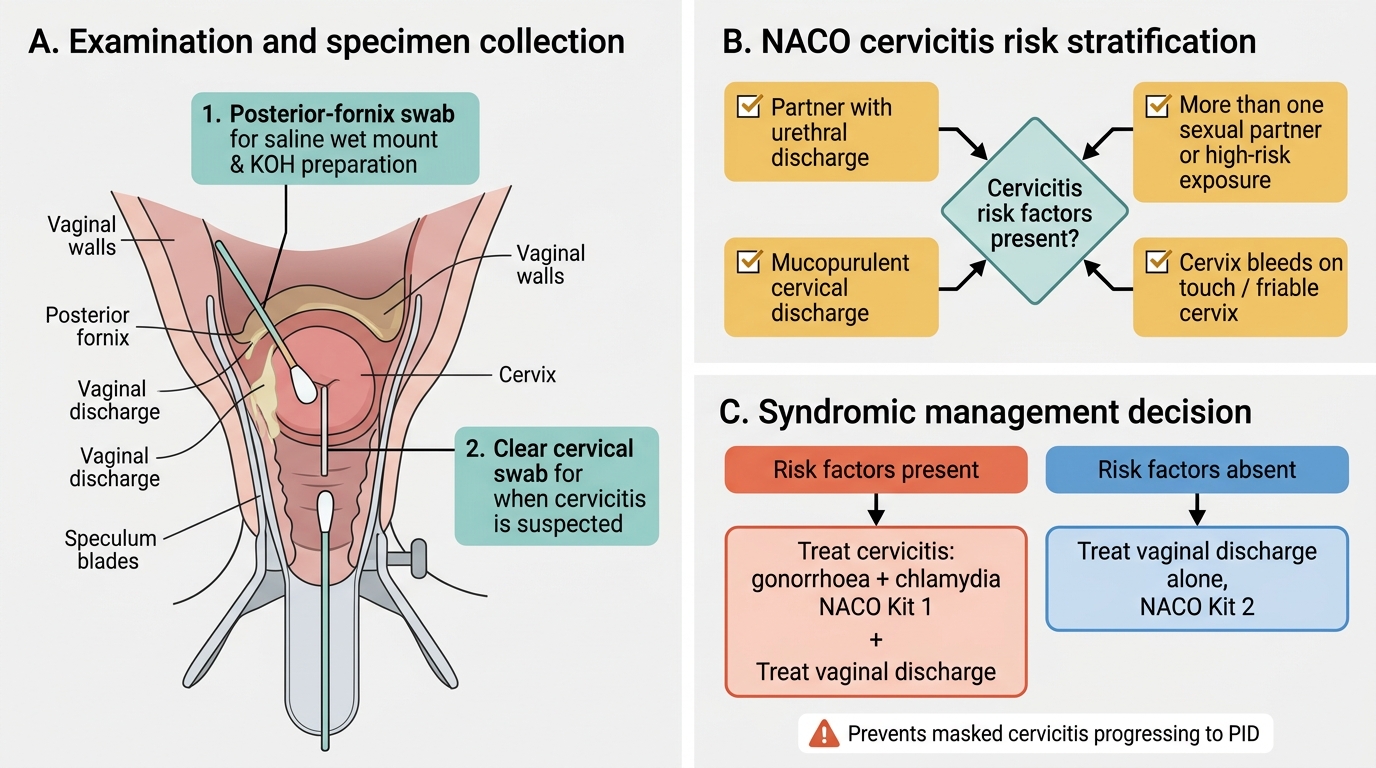
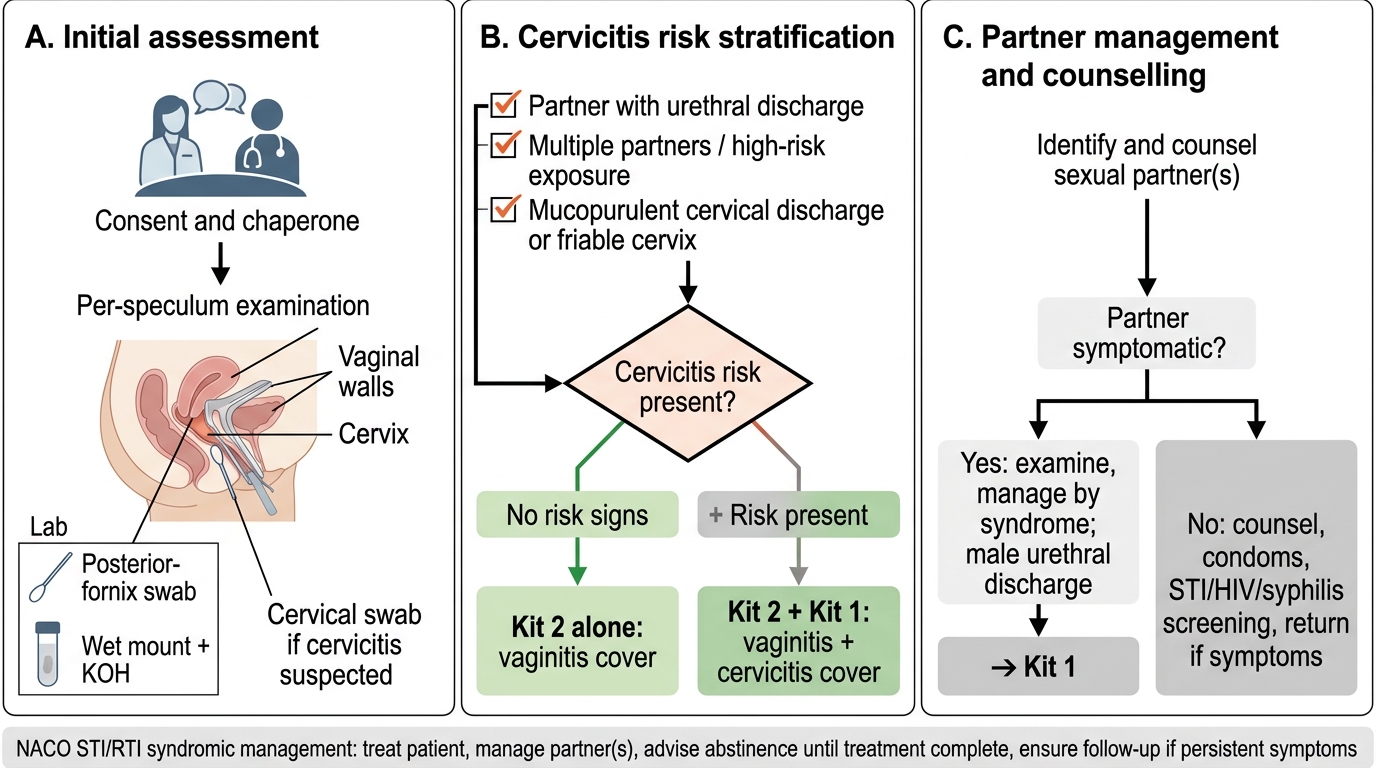
The procedural skill combines a careful examination with the NACO risk-stratification step that defines syndromic management of vaginal discharge. After consent and with a chaperone, perform a per-speculum examination, inspecting the vaginal walls, the cervix, and the character of the discharge, and collect specimens — a swab from the posterior fornix for the saline wet mount and KOH preparation, and a cervical swab if cervicitis is suspected. The decisive NACO step is risk stratification for cervicitis: assess for risk factors such as a partner with urethral discharge, more than one sexual partner, mucopurulent cervical discharge, or a cervix that bleeds on touch. If cervicitis risk factors are present, you treat for cervicitis (gonorrhoea/chlamydia, NACO Kit 1) in addition to the vaginal discharge; if they are absent, vaginal-discharge treatment alone (Kit 2) suffices. This single algorithmic decision is what prevents a masked cervicitis from progressing to pelvic inflammatory disease.
NACO Vaginal Discharge Syndromic Management Algorithm
Examination and stratification:
1. Consent and chaperone; per-speculum examination of walls, cervix, discharge
2. Posterior-fornix swab for wet mount and KOH; cervical swab if cervicitis suspected
3. Assess cervicitis risk factors (partner with discharge, multiple partners, mucopurulent cervical discharge)
4. Risk present → add Kit 1 (cervicitis cover); risk absent → Kit 2 alone