Page 26 of 35
DR10.10 | Vaginal Discharge Syndromic Management — SDL Guide (Part 2)
Interpreting Microscopy and Clinical Findings

Microscopy and Clinical Clues in Vaginal Discharge Syndromes
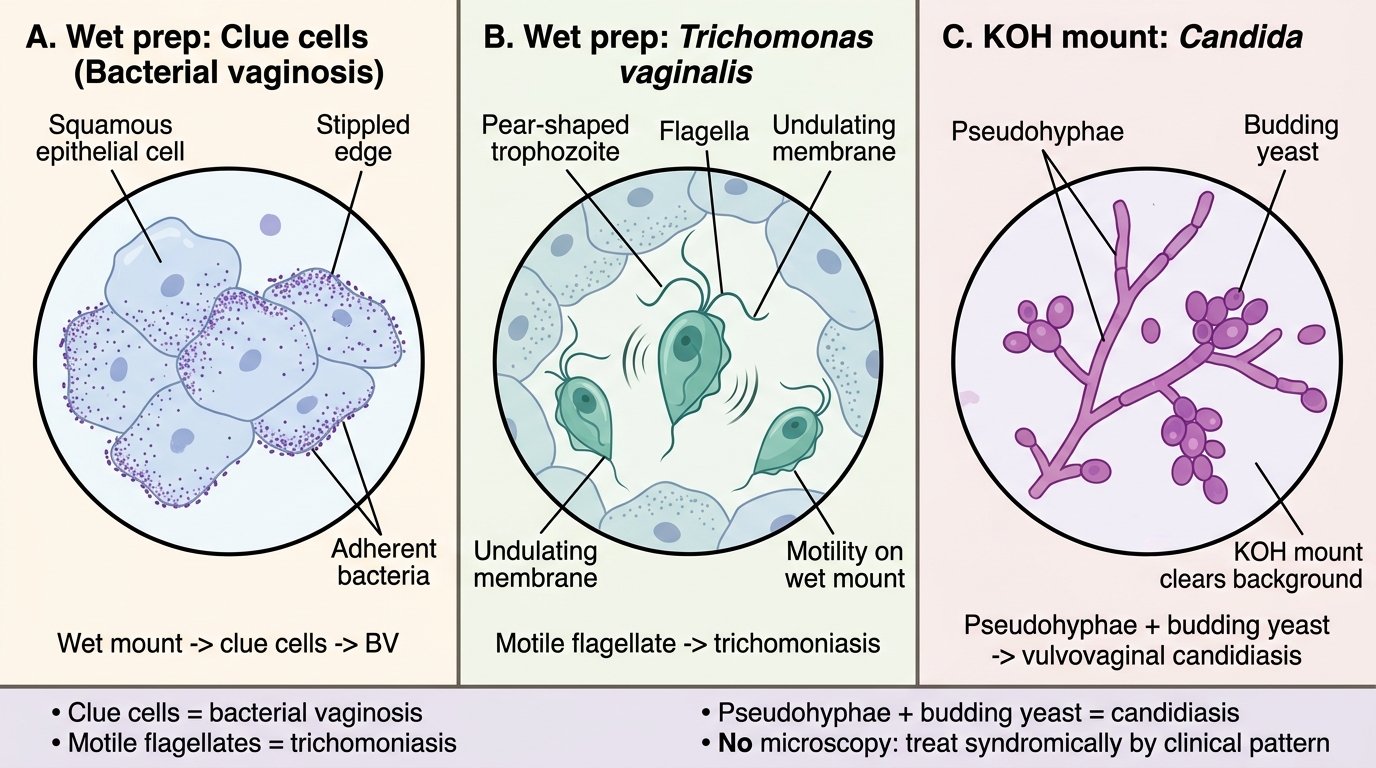
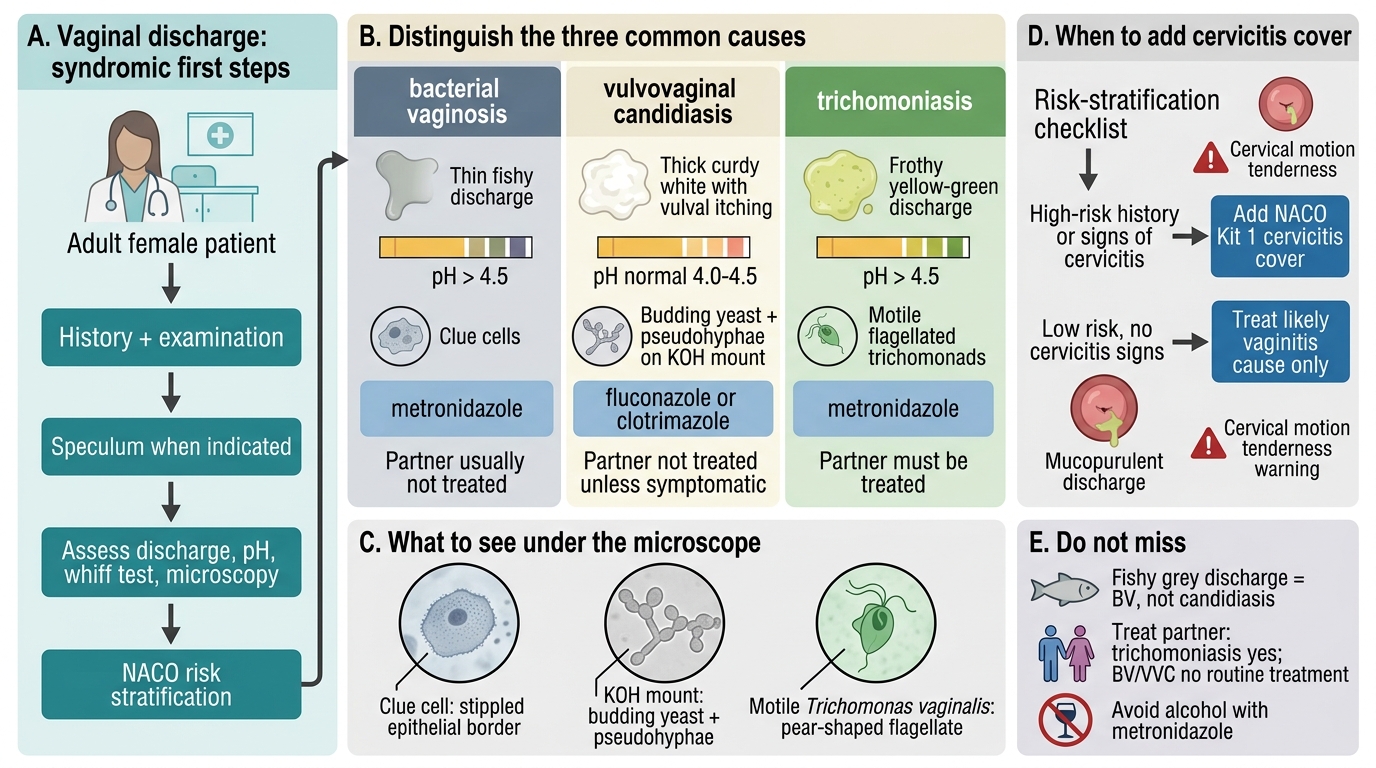
Interpreting the bedside findings pulls the diagnosis together and confirms which treatment branch to follow. On the saline wet mount, clue cells (vaginal epithelial cells studded with coccobacilli so that their borders look stippled and indistinct) point to bacterial vaginosis, while motile pear-shaped flagellates confirm trichomoniasis; an excess of neutrophils without a clear pathogen should raise suspicion of cervicitis. On the KOH mount, pseudohyphae with budding yeast confirm vulvovaginal candidiasis. The strawberry cervix (colpitis macularis — punctate haemorrhages on the cervix) is pathognomonic of trichomoniasis but is seen clinically in only a small minority of cases, so its absence does not exclude the diagnosis. Where microscopy is unavailable, you treat syndromically on the clinical pattern. Always integrate the discharge character, pH, and whiff result with the microscopy rather than relying on any single finding.
Microscopy Findings in Vaginal Discharge Syndromes
Interpretation pointers:
- Clue cells on wet mount → bacterial vaginosis
- Motile flagellates on wet mount → trichomoniasis (strawberry cervix, when present, is pathognomonic)
- Pseudohyphae + budding yeast on KOH → vulvovaginal candidiasis
- No microscopy available → treat syndromically on the clinical pattern
SELF-CHECK
During risk stratification of a woman with vaginal discharge, you find her partner has urethral discharge and she has mucopurulent cervical discharge. What does NACO syndromic management direct you to do?
A. Treat for vaginal discharge alone (Kit 2), since the discharge is vaginal
B. Treat for vaginal discharge AND add cervicitis cover (Kit 1) because cervicitis risk factors are present
C. Give an antifungal only and review in one month
D. Withhold all treatment until culture results return
Reveal Answer
Answer: B. Treat for vaginal discharge AND add cervicitis cover (Kit 1) because cervicitis risk factors are present
When cervicitis risk factors are present (e.g. a partner with urethral discharge, mucopurulent cervical discharge, multiple partners), NACO directs you to add cervicitis cover (Kit 1, for gonorrhoea/chlamydia) to the vaginal-discharge treatment (Kit 2). Treating the vaginal discharge alone would leave a cervicitis to ascend toward pelvic inflammatory disease.
Syndromic Management With NACO Kit 2 and Partner Counselling
Provided image
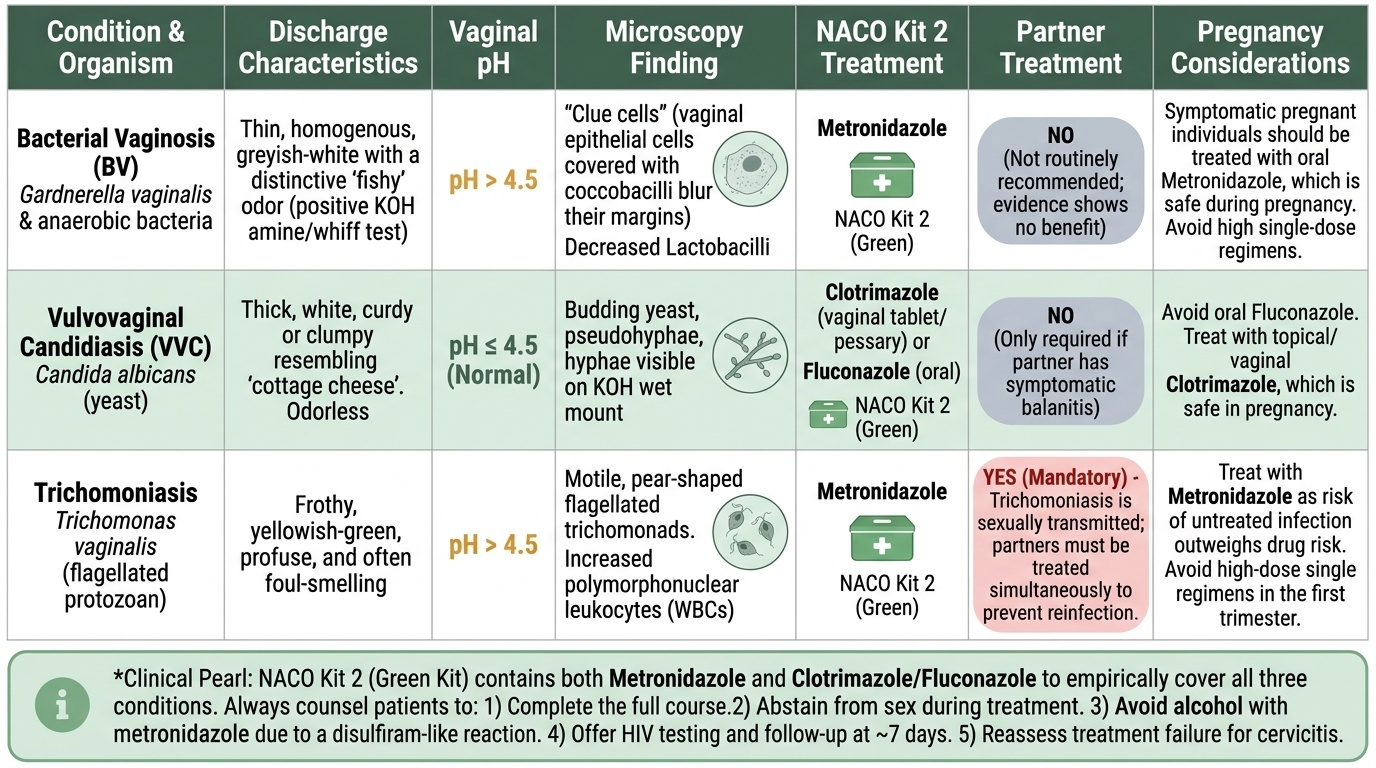
Applied management of vaginal discharge under NACO uses Kit 2 (green) — per current NACO guidance, exact drugs to be confirmed against the latest protocol — and the key skill is matching treatment and partner-management to the cause. Metronidazole covers both bacterial vaginosis and trichomoniasis, while clotrimazole (or fluconazole) covers the candidiasis component. The partner-treatment rule is critical and often confused: trichomoniasis requires treatment of the sexual partner (it is sexually transmitted and partners reinfect each other), whereas bacterial vaginosis does NOT routinely require partner treatment (the evidence shows no benefit). Counsel every patient to complete the course, abstain from sex during treatment, and — importantly with metronidazole — avoid alcohol because of a disulfiram-like reaction. Offer HIV testing, arrange follow-up at about 7 days, and address pregnancy considerations (BV and candidiasis are treated in pregnancy with appropriate agents). Treatment failure or recurrence prompts reassessment, including for a missed cervicitis.
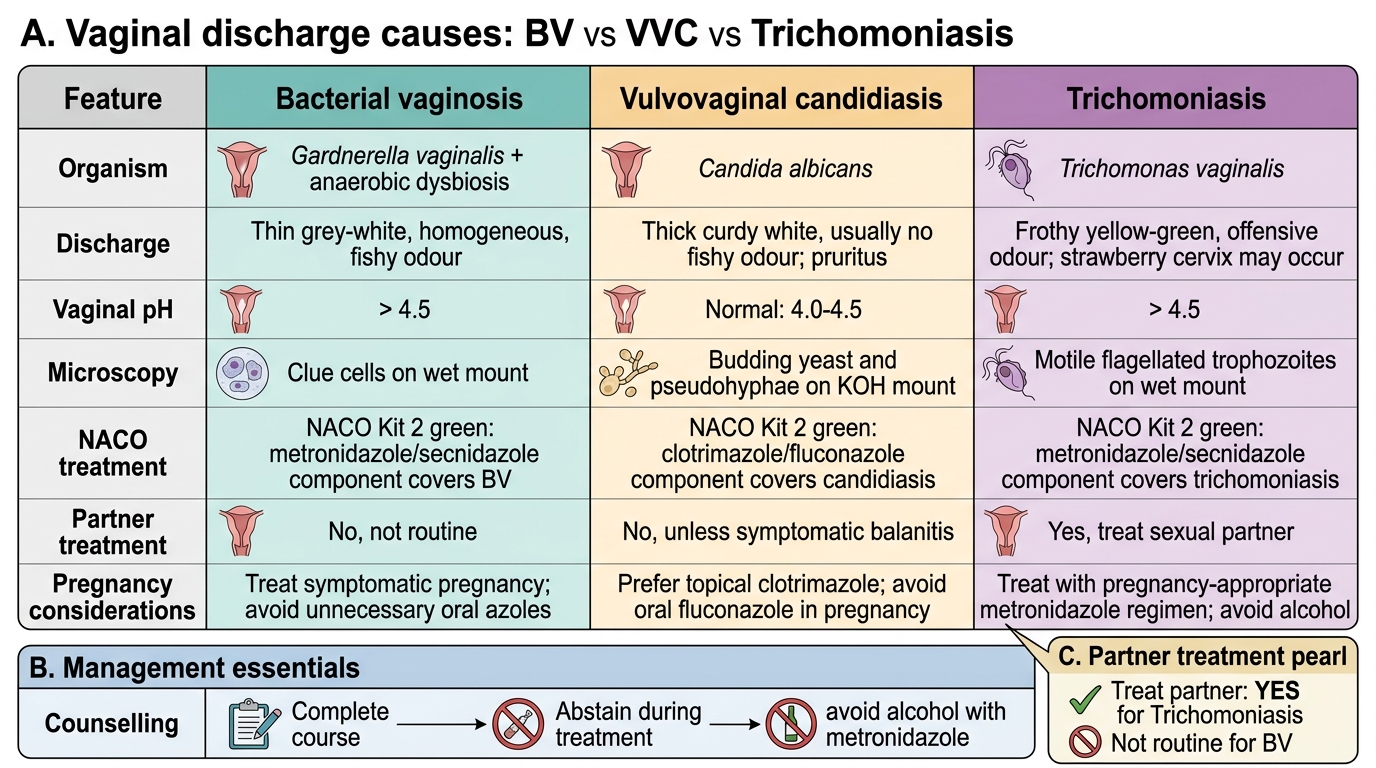
Vaginal Discharge Causes: BV vs VVC vs Trichomoniasis
Management essentials:
- NACO Kit 2 (green): metronidazole (covers BV + trichomoniasis) + clotrimazole/fluconazole (candidiasis)
- Partner treatment: YES for trichomoniasis; NOT routine for bacterial vaginosis
- Counsel: complete course, abstain during treatment, avoid alcohol with metronidazole
- Offer HIV testing, follow up ~7 days, manage pregnancy appropriately; reassess failure for cervicitis
SELF-CHECK
Which statement about partner treatment in vaginal discharge syndromes is correct?
A. Partner treatment is required for bacterial vaginosis but not for trichomoniasis
B. Partner treatment is required for trichomoniasis but is NOT routinely recommended for bacterial vaginosis
C. Partner treatment is required for all three causes equally
D. Partner treatment is never needed for any vaginal discharge syndrome
Reveal Answer
Answer: B. Partner treatment is required for trichomoniasis but is NOT routinely recommended for bacterial vaginosis
Trichomoniasis is sexually transmitted and requires treatment of the partner to prevent reinfection. Bacterial vaginosis is a dysbiosis rather than a classically transmitted infection, and partner treatment is NOT routinely recommended because evidence shows no benefit. This distinction is a frequent point of confusion and is clinically important.
Self-Assessment: Vaginal Discharge Syndromic Management
Vaginal Discharge Syndromic Management
Consolidate your command of this syndrome before moving on, because vaginal discharge is the presentation where similar-looking conditions demand genuinely different actions, and where a confident clinician saves a patient repeated, futile clinic visits. Work through the self-check below as if a woman were in front of you, naming the cause, the pH, the microscopy finding, the kit, and — every time — the partner-treatment rule, since that is the single point learners most often get wrong. Give special attention to two ideas: that a fishy grey discharge is bacterial vaginosis and not candidiasis, and that the NACO risk-stratification step decides whether you must add cervicitis cover. Where any answer feels uncertain, return to the relevant section and rehearse the distinction until it is automatic, because in a busy clinic you default to whatever you have practised. Treat each gap as a prompt for revision, not a reason for doubt.
Self-check questions:
- What are the four Amsel criteria, and how many are needed to diagnose BV?
- What does the KOH mount show in vulvovaginal candidiasis?
- Which drug covers both BV and trichomoniasis, and which covers candidiasis?
- For which cause(s) must you treat the partner, and for which not?
- When does NACO direct you to add cervicitis cover (Kit 1)?
- Why must patients avoid alcohol while taking metronidazole?
CLINICAL PEARL
The fishiest pitfall in vaginal discharge is mislabelling bacterial vaginosis as 'a fungal infection' and prescribing an antifungal — a grey, fishy, pH-elevated discharge with clue cells is BV, and it needs metronidazole, not clotrimazole. Two reflexes will keep you safe: pair every metronidazole prescription with a clear 'no alcohol' warning to avoid the disulfiram-like reaction, and remember the partner rule as a single phrase — 'treat the partner for trichomoniasis, not for BV'. And never let a 'simple discharge' distract you from the cervicitis risk-stratification step that protects future fertility.