Page 5 of 12
DR14.3 | Dermographism Demonstration — SDL Guide
Learning Objectives
- State the clinical indications for eliciting dermographism and place the test within the diagnostic pathway for inducible urticaria
- Explain the underlying principle of the test — the triple response of Lewis — and assemble the materials required
- Demonstrate the correct technique for eliciting symptomatic dermographism by stroking the skin
- Interpret the dermographic response, distinguishing a positive symptomatic result from asymptomatic simple dermographism, and translate the result into a management decision
INSTRUCTIONS
Dermographism — literally 'skin writing' — is the commonest of the inducible urticarias, and it can be confirmed at the bedside in under five minutes with nothing more than a blunt object and a watch. This is a skills module, not a disease lecture: the aim is for you to perform the elicitation technique correctly, observe the wheal-and-flare response it produces, and interpret what you see, distinguishing the asymptomatic 'writing skin' present in a fifth of healthy people from the symptomatic disease that warrants treatment. Mastering this simple manoeuvre lets you turn a vague history of 'itchy lines after scratching' into a confirmed diagnosis and a clear management plan, without referring the patient for any laboratory test.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Urticaria and Angioedema (Physical/Inducible Urticarias) (textbook)
- Sacchidanand S, et al. (eds). IADVL Textbook of Dermatology, 4th ed. Section: Physical Urticarias and Bedside Diagnostic Tests (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old medical intern mentions, almost in passing, that whenever she scratches an itch or her bag strap rubs her shoulder, a raised itchy line springs up exactly where the skin was touched and fades within the hour. She has no rash otherwise and feels perfectly well. Rather than ordering a panel of allergy tests, her tutor simply takes the wooden end of a cotton swab, draws a firm line across her forearm, and asks her to watch. Within a couple of minutes a pink, slightly raised line — itchy, following the exact path of the stroke — rises out of the skin: she has, in effect, written on herself. In that one painless manoeuvre the diagnosis of symptomatic dermographism has been made. This module teaches you to perform and interpret that manoeuvre.
WHY THIS MATTERS
Patients who describe wheals appearing wherever they scratch, rub, or are pressed are common, and the temptation is to investigate them broadly or to dismiss the complaint. The dermographism demonstration replaces both errors with a definitive bedside answer: a positive test confirms an inducible urticaria, explains the patient's symptoms, and points straight to a simple management plan, while a negative test redirects your thinking. Because the technique needs no equipment beyond a blunt object and costs nothing, it is a skill every clinician — not just the dermatologist — can and should use. Just as importantly, performing the test correctly and interpreting it honestly stops you from over-diagnosing the one-in-twenty healthy people whose skin writes without any symptoms at all. This is bedside medicine at its most economical: a single, safe manoeuvre that converts an uncertain history into a confident diagnosis.
RECALL
Before performing the test, recall from SDL 1 of this cluster the classification of urticaria: that chronic inducible urticaria is the subset in which wheals are reproducibly provoked by a specific physical stimulus, and that dermographism — provoked by stroking or scratching the skin — is its commonest form. Recall, too, the underlying pathology you learned there: a wheal is superficial dermal oedema produced when mast cells release histamine, which dilates local vessels (redness), increases their permeability (the raised wheal), and stimulates sensory nerves (itch). The dermographism test is simply a controlled way of triggering that mast-cell response along a line you choose, so that you can watch the wheal form. These prior concepts are the foundation for understanding both why the test works and what a positive result means.
When the Skin Writes: Clinical Relevance of Dermographism
Clinical Relevance of Dermographism
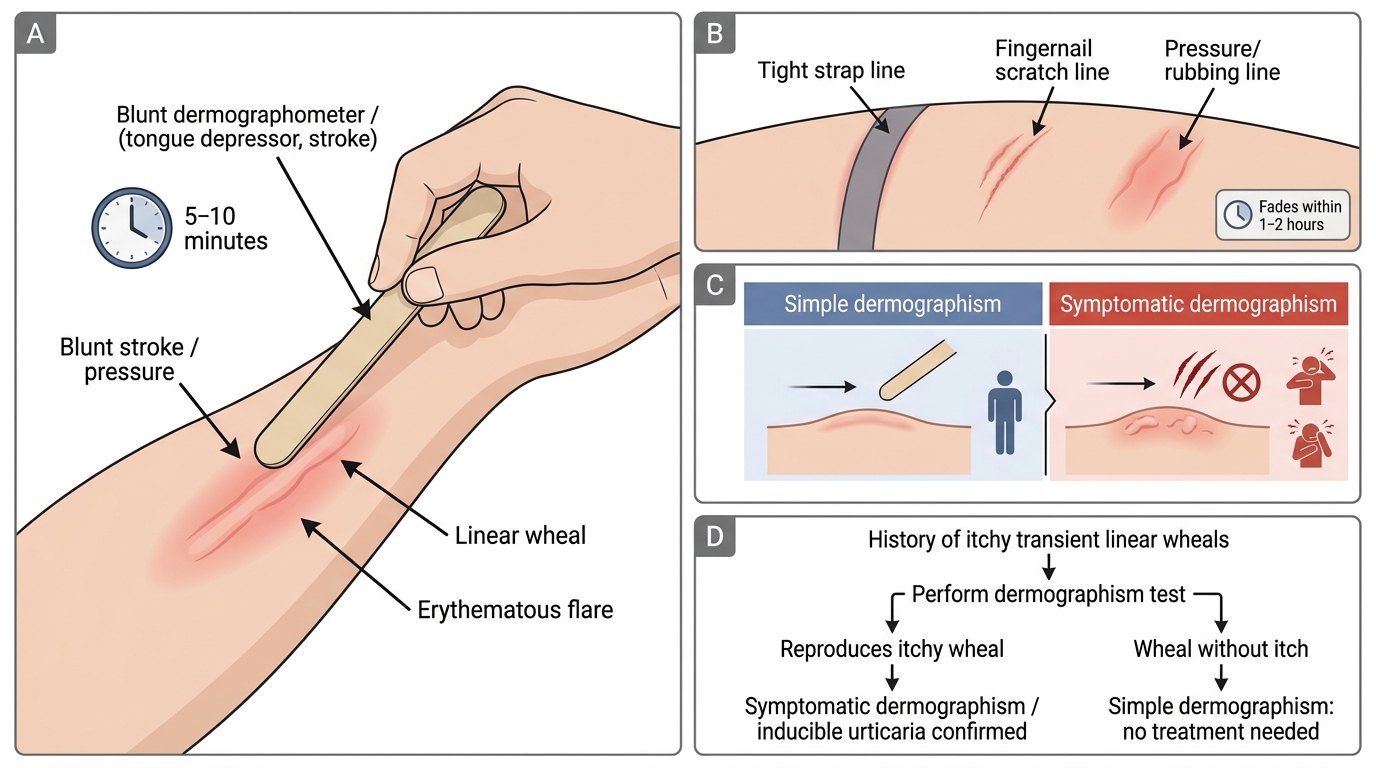
The first thing to establish is when you should reach for this test at all, because performing it on the right patient is what makes the result meaningful. The classic indication is a patient who gives a history of transient, itchy, linear wheals that appear wherever the skin is stroked, scratched, rubbed, or pressed — for example along the line of a tight strap, a scratch, or a fingernail mark — and which fade within an hour or two. Such a history strongly suggests an inducible urticaria, and dermographism is its commonest cause; the demonstration confirms it on the spot. The test is also valuable in any patient being worked up for chronic urticaria, where confirming an inducible component changes both the explanation you give the patient and the advice you offer about avoiding provocation.
A crucial clinical caveat shapes the whole interpretation of the test: dermographism exists in two forms, and only one is a disease. Simple (asymptomatic) dermographism is present in roughly one in twenty healthy people — their skin produces a wheal when stroked, but they have no itch and no symptoms, and they need no treatment. Symptomatic dermographism is the clinically significant form, in which the provoked wheals are itchy and troublesome. The purpose of doing the test in a symptomatic patient is therefore not merely to see whether the skin writes, but to reproduce the patient's actual symptom — the itchy wheal — and so confirm that their complaint has an inducible-urticaria basis. Keeping this distinction in view prevents the common error of labelling a healthy person with asymptomatic 'writing skin' as having a disease.
The indications and key distinction:
- Perform the test when: the patient reports transient itchy linear wheals at sites of stroking, scratching, rubbing, or pressure.
- Also useful in: any chronic-urticaria work-up, to confirm an inducible component.
- Simple (asymptomatic) dermographism: wheal present, no itch; ~5% of healthy people; no treatment.
- Symptomatic dermographism: itchy, troublesome wheals; the clinically significant form that the test aims to reproduce.
Underlying Principle and Required Materials
Triple Response of Lewis in Dermographism Testing
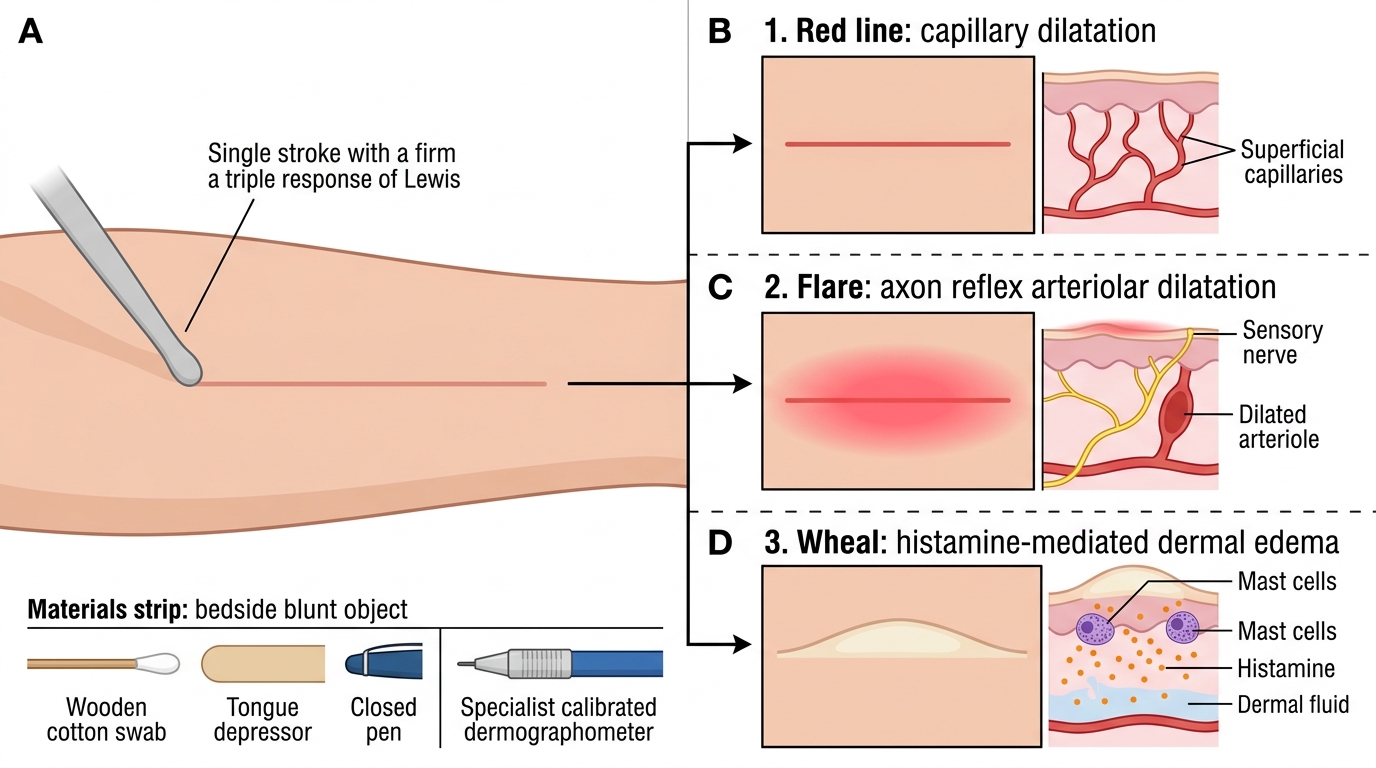
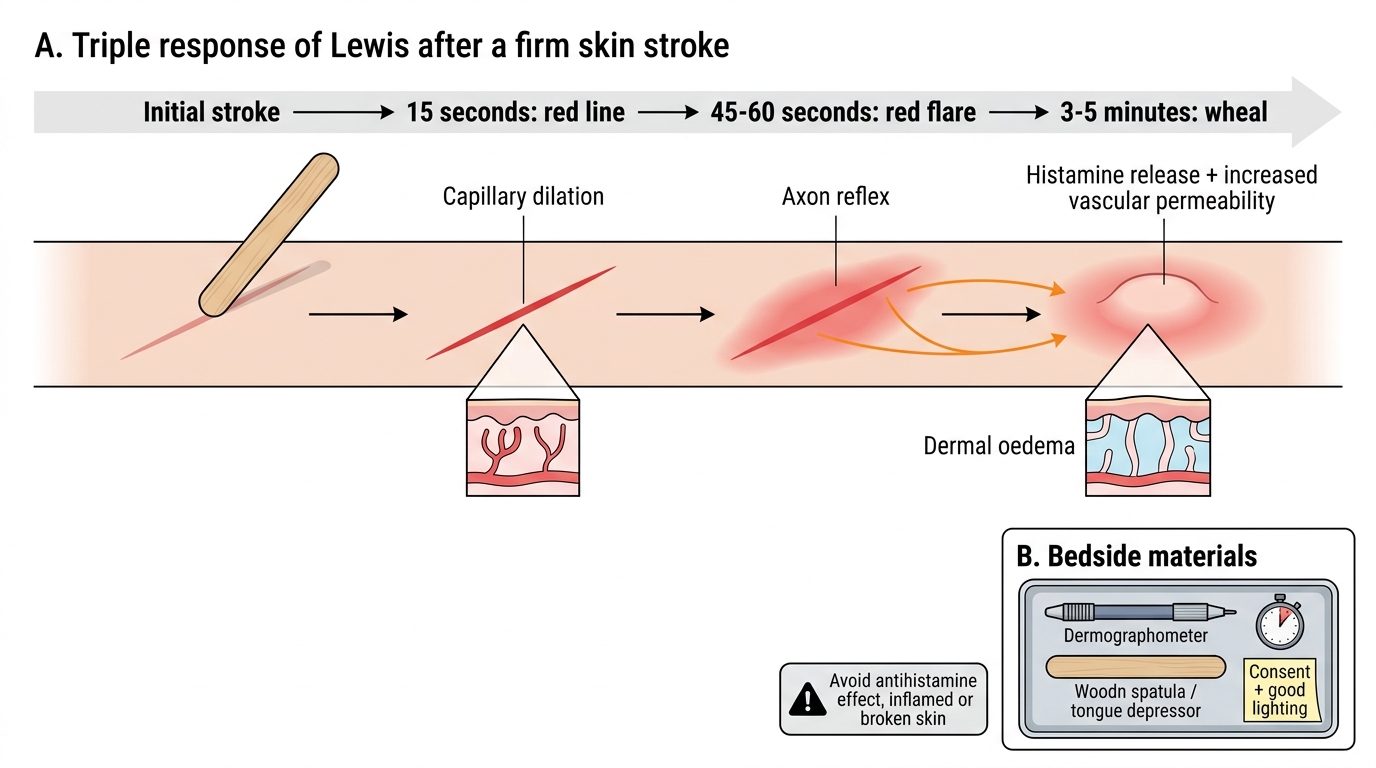
To perform and interpret the test confidently you must understand the physiological response it elicits, known as the triple response of Lewis — the sequence of skin changes that follows a firm stroke and which underlies the wheal you are trying to produce. When the skin is stroked firmly, the local trauma triggers mast-cell mediator release, and three events unfold in order. First, within seconds, a red line appears along the stroke as the smallest blood vessels (capillaries) dilate. Second, over the next minute or so, a brighter red flare spreads outward on either side of the line, produced by an axon reflex that dilates nearby arterioles. Third, after a few minutes, a raised, pale wheal forms along the original line as histamine increases vascular permeability and fluid leaks into the dermis. It is this third component — the wheal — that constitutes a positive dermographism, and recognising the orderly red line → flare → wheal sequence reassures you that you are observing a genuine response rather than simple mechanical reddening.
The materials required are deliberately minimal, which is part of the test's value, but each should be prepared before you begin. You will need a firm blunt object to apply a controlled linear stroke; in a specialist setting a calibrated dermographometer delivers a defined, reproducible pressure, but at the bedside the wooden end of a cotton swab, a tongue depressor edge, or the edge of a closed pen are entirely acceptable. You also need a timer or watch to observe the response at the correct interval, good lighting to see the often-subtle wheal, and the patient's consent and cooperation, having explained that you will draw a firm line on the skin and watch for a reaction. One important pre-condition affects validity: recent antihistamine use can suppress the response and cause a false-negative, so ask about and, where feasible, withhold antihistamines before testing. Avoid testing over actively inflamed or broken skin.
Triple Response of Lewis in Dermographism
Principle and kit at a glance:
- Triple response of Lewis: red line (capillary dilation) → red flare (axon reflex) → wheal (histamine-mediated oedema).
- Materials: firm blunt object (dermographometer, or wooden swab end/tongue depressor/pen edge), timer, good lighting, consent.
- Validity caveat: recent antihistamines cause false-negatives; avoid inflamed or broken skin.
Step-by-Step Procedure: Eliciting the Dermographic Response
Eliciting the Dermographic Response
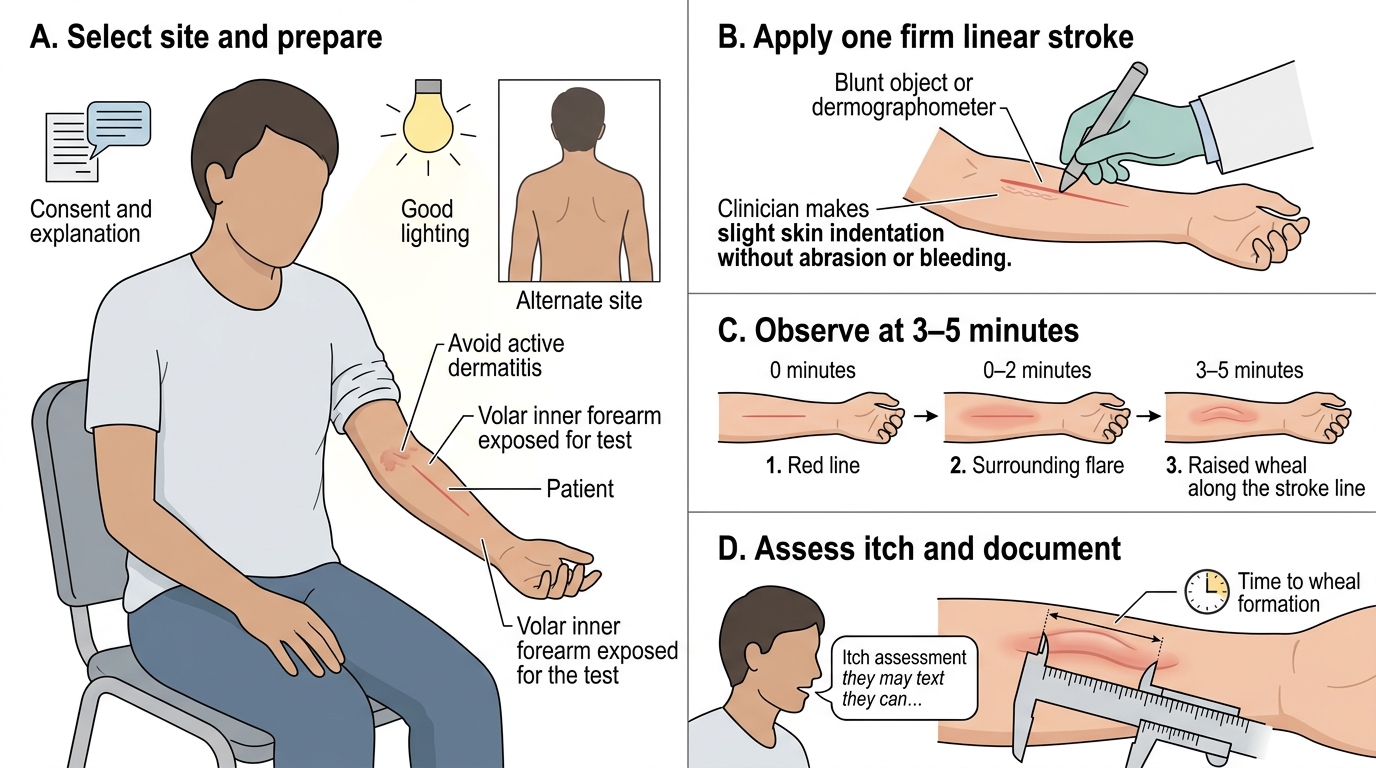
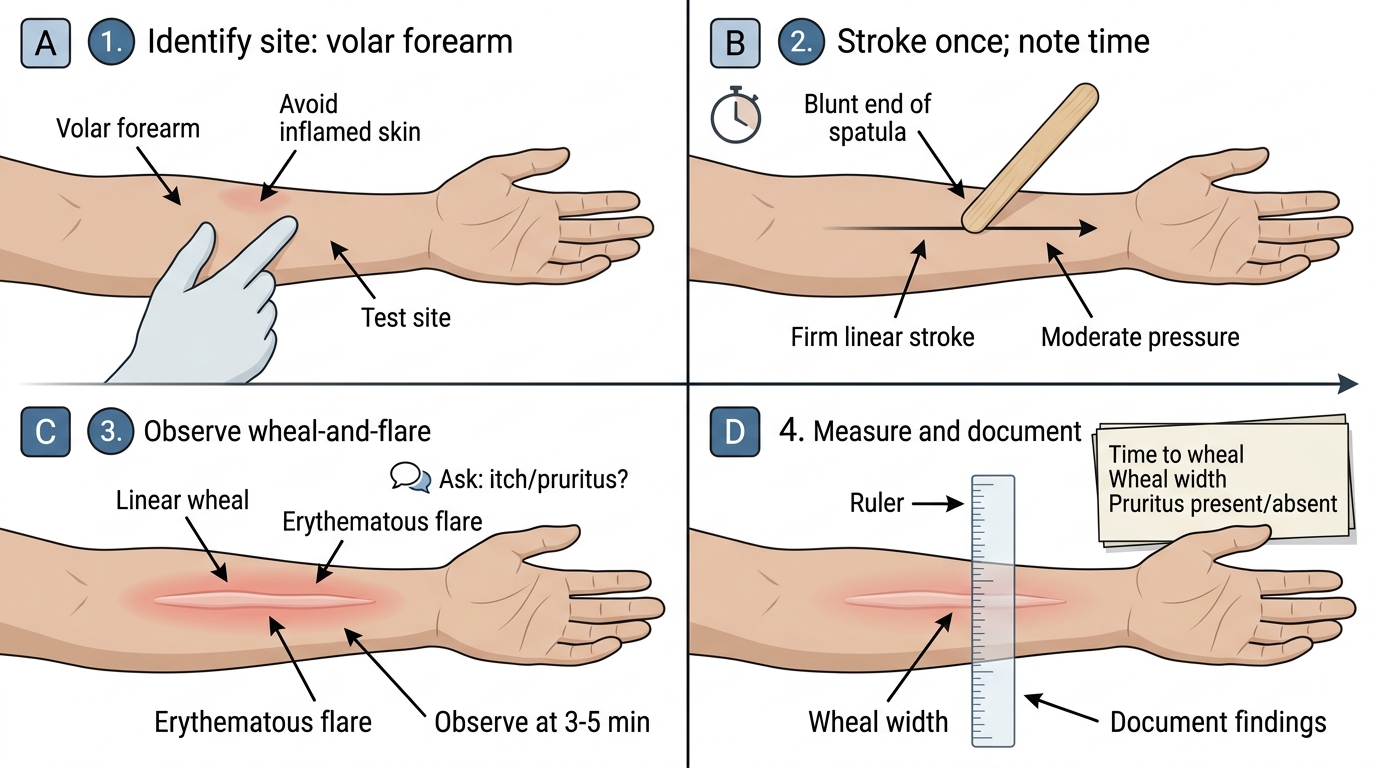
With the principle understood and the kit ready, the procedure itself is short but must be done with consistent technique so that the result is reliable and reproducible. Begin by explaining the test and obtaining consent, reassuring the patient that it is painless and that any reaction will settle on its own. Choose an appropriate test site — the volar (inner) forearm or the upper back are ideal because the skin is accessible, relatively hairless, and easy to observe; avoid areas of active dermatitis. Hold the blunt object and apply a single, firm, linear stroke of moderate and even pressure across the chosen site, perhaps 5–10 cm long; if you are using a dermographometer, apply the defined pressure it is calibrated for. The pressure should be firm enough to indent the skin slightly but not enough to break it or cause pain. Note the time at which you make the stroke.
Now wait and observe, because the diagnostic component takes a few minutes to appear. Watch the stroke line over the next 3 to 5 minutes in good light: you should first see the red line, then the flare, and finally — if the test is positive — a raised wheal rising along the line of contact. Ask the patient at this point whether the area itches, since the presence of itch is what separates symptomatic from asymptomatic dermographism. Document what you find: the time to wheal formation, the dimensions of the wheal (a measurable width along the stroke), and whether pruritus was present. If the first stroke is equivocal, it is reasonable to repeat on an adjacent site or with slightly firmer pressure, but never to the point of injuring the skin. Consistent site selection, pressure, and timing are what make your result trustworthy and repeatable.
Dermographism Demonstration on the Volar Forearm
The procedure in sequence:
1. Explain the test and obtain consent.
2. Select the site (volar forearm or upper back; avoid inflamed skin).
3. Apply a single firm, even linear stroke of moderate pressure; note the time.
4. Wait and observe the stroke line over 3–5 minutes in good light.
5. Ask the patient whether the area itches.
6. Document time to wheal, wheal width, and presence of pruritus; repeat on an adjacent site if equivocal.
SELF-CHECK
After firmly stroking a patient's volar forearm with the blunt end of a swab, at what interval should you principally observe the line for the diagnostic wheal, and which additional observation distinguishes symptomatic from asymptomatic dermographism?
A. Observe within 5 seconds; the colour of the line distinguishes the two forms
B. Observe at 3–5 minutes for a raised wheal; the presence of itch (pruritus) distinguishes symptomatic from asymptomatic dermographism
C. Observe after 24 hours; the persistence of the wheal distinguishes the two forms
D. Observe immediately; only the width of the red line matters, not any symptom
Reveal Answer
Answer: B. Observe at 3–5 minutes for a raised wheal; the presence of itch (pruritus) distinguishes symptomatic from asymptomatic dermographism
The diagnostic component of the dermographic response — the raised wheal along the line of the stroke — develops over a few minutes, so the line should be observed principally at 3 to 5 minutes after stroking, in good light. Seeing a wheal confirms dermographism, but it does not by itself tell you whether the patient has the clinically significant disease. The crucial additional observation is whether the wheal itches: a wheal accompanied by pruritus indicates symptomatic dermographism (the form that warrants treatment), whereas a wheal without any itch is simple, asymptomatic dermographism — present in about one in twenty healthy people and requiring no treatment. Both the timing of observation and the assessment of itch are therefore essential to a correctly performed and interpreted test.