Page 6 of 12
DR14.3 | Dermographism Demonstration — SDL Guide (Part 2)
Interpreting the Result: Positive, Negative, and Equivocal
Interpreting the Dermographism Test
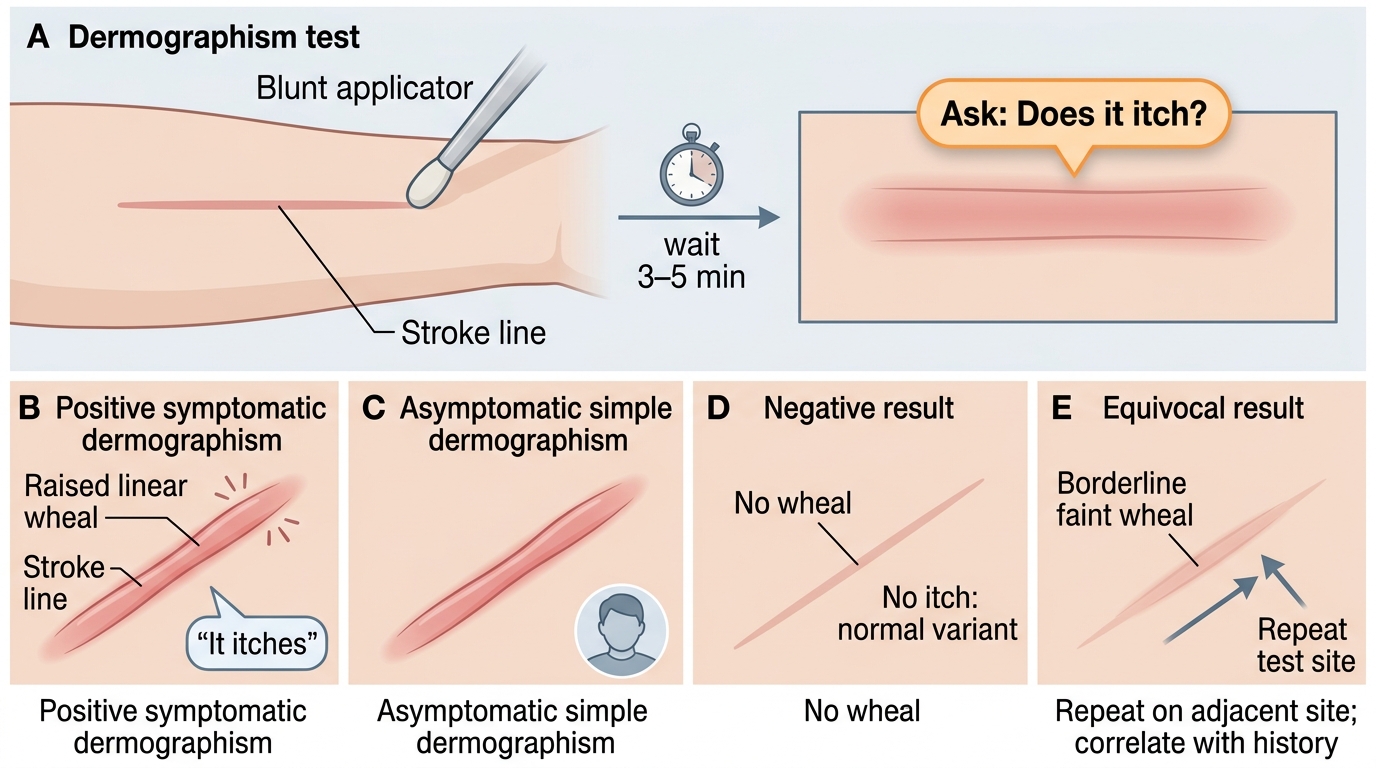
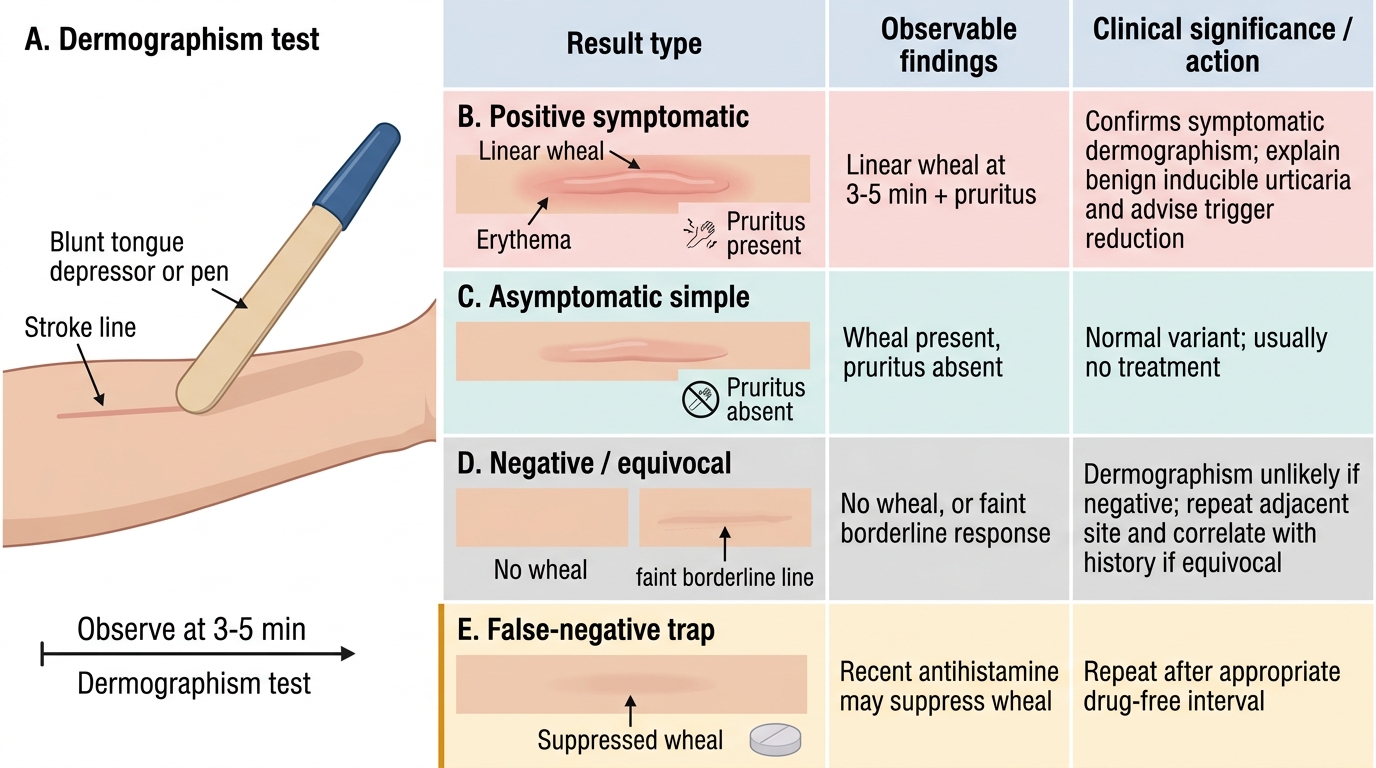
Interpreting the dermographism test correctly is as important as performing it, because the same physical sign can mean different things, and the interpretation drives what you do next. A positive symptomatic result — the finding that confirms clinically significant dermographism — is a raised, palpable, linear wheal developing along the line of the stroke within 3–5 minutes and accompanied by itch. This reproduces the patient's complaint and establishes the diagnosis of symptomatic dermographism. By contrast, asymptomatic (simple) dermographism is a wheal that forms in the same way but without any itch or symptom; because it occurs in about one in twenty healthy people, it is a normal variant and should not be labelled a disease or treated. The single observation that separates these two — the presence or absence of pruritus — is therefore the pivot of the entire interpretation, which is why you must specifically ask the patient whether the area itches.
Two further categories complete the picture. A negative result is no wheal along the stroke line at 3–5 minutes; this makes dermographism unlikely, though it does not exclude other inducible urticarias, which have their own provocation tests. An equivocal result is a faint or borderline response, or a wheal without clear symptoms; here it is reasonable to repeat the test on an adjacent site with consistent technique and to weigh the result against the patient's history. The most important pitfall to recognise is the false-negative caused by recent antihistamine use: because antihistamines suppress the histamine-driven wheal, a patient who has taken one may show no response despite truly having the condition. If antihistamine use is likely and the history is suggestive, the test should be repeated after an appropriate drug-free interval before concluding it is negative.
Interpreting the Dermographism Test
Interpretation summary:
- Positive symptomatic: linear wheal at 3–5 min with itch → confirms symptomatic dermographism.
- Asymptomatic (simple): wheal without itch → normal variant (~5%); no treatment.
- Negative: no wheal at 3–5 min → dermographism unlikely (other inducible urticarias still possible).
- Equivocal: faint/borderline → repeat on adjacent site, correlate with history.
- False-negative trap: recent antihistamine suppresses the wheal → repeat after a drug-free interval.
Applied Practice: Using the Result in Clinical Decision-Making
Using a Positive Dermographism Test in Clinical Management
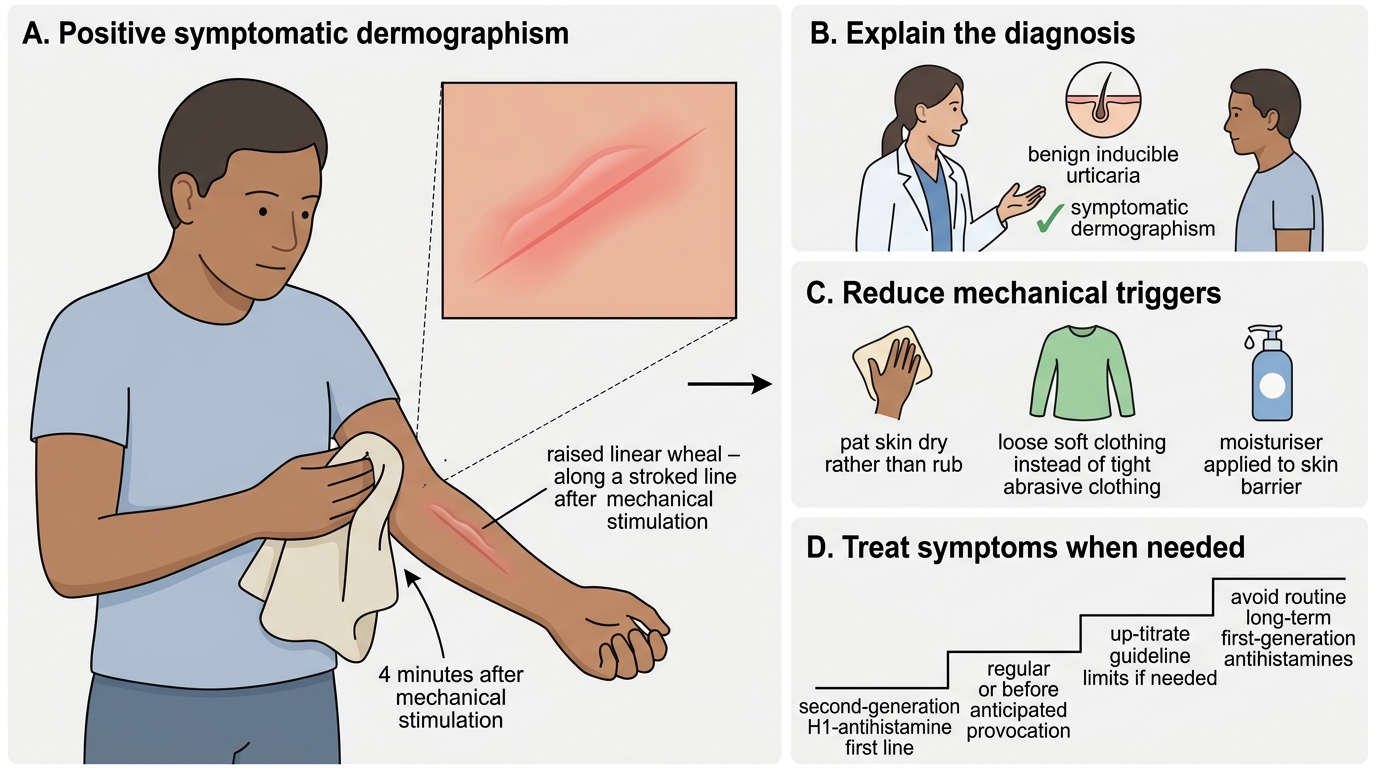
The value of the test lies in what you do with the result, so it helps to work through how a positive finding translates into a management plan using a realistic scenario. Consider a patient who reports itchy linear wheals after towelling dry vigorously or when tight clothing rubs the skin, in whom you perform the test and observe a clear, itchy wheal along the stroke line at four minutes — a positive symptomatic dermographism. The first step is simply to explain the diagnosis, reassuring the patient that this is a recognised, benign form of inducible urticaria and that their symptoms have a clear, understandable cause. The second step is trigger advice: because the wheals are provoked mechanically, practical measures such as patting rather than rubbing the skin dry, avoiding tight or abrasive clothing, and keeping the skin moisturised genuinely reduce symptoms.
The third step is pharmacological treatment where symptoms warrant it, and here the management mirrors that of urticaria generally: a second-generation, non-sedating H1-antihistamine (such as cetirizine, levocetirizine, or fexofenadine) is the first-line treatment, taken regularly or before anticipated provocation, and the dose may be up-titrated within guideline limits if standard dosing is insufficient. Sedating first-generation antihistamines are avoided for routine long-term control. By contrast, a patient in whom the test reproduces a wheal without any itch needs only reassurance that this is asymptomatic dermographism, a normal variant requiring no treatment — a deliberately different decision that flows directly from the interpretation. Finally, document the test, its result, and the plan, and arrange follow-up or referral if symptoms are severe, persistent, or atypical. This worked sequence — confirm, explain, advise, treat to symptom severity — is the applied core of the skill.
Dermographism: Result-to-Action Decision Table
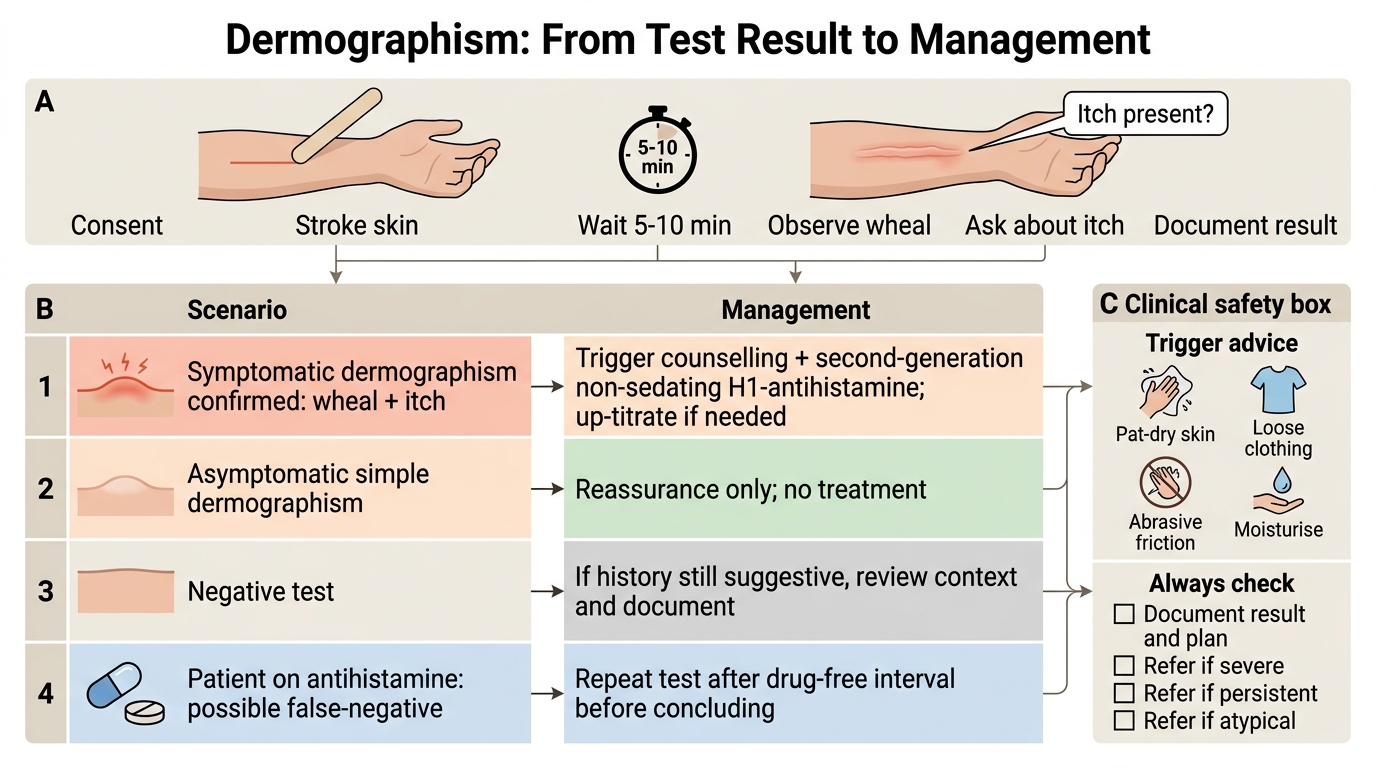
From result to action:
- Positive symptomatic: explain diagnosis → trigger advice (pat dry, avoid tight/abrasive clothing, moisturise) → second-generation non-sedating H1-antihistamine, up-titrated if needed.
- Asymptomatic (simple): reassurance only; no treatment.
- Negative but suggestive history on antihistamine: repeat after a drug-free interval before concluding.
- Always: document the result and plan; refer if severe, persistent, or atypical.
Self-Assessment
Before finishing, check whether you can now both perform and interpret the dermographism demonstration, because a skill is only learned when you can reproduce it reliably and act on what you see. Mentally rehearse the whole sequence on a cooperative patient — consent, site, stroke, wait, observe, ask about itch, document — and then test your interpretation against the scenarios below. The decisions that most often trip up learners are two: forgetting that the presence of itch (not merely the presence of a wheal) defines the symptomatic, treatable form, and forgetting that a recent antihistamine can produce a false-negative. If either of these feels uncertain, revisit the interpretation section before attempting the cluster quiz, and if possible practise the manoeuvre under supervision on a willing colleague.
Self-check questions to attempt:
1. List, in order, the steps of the dermographism demonstration from consent to documentation.
2. Name the three components of the triple response of Lewis and the interval at which you observe for the diagnostic wheal.
3. State the single observation that distinguishes symptomatic from asymptomatic dermographism, and the management implication of each.
4. Explain why a patient with a convincing history might have a negative test, and what you would do about it.
5. Outline the first-line drug treatment for symptomatic dermographism and the trigger advice you would give.
CLINICAL PEARL
A wheal is not a diagnosis until you have asked about itch. The whole clinical meaning of the dermographism test turns on a single question put to the patient while the wheal is rising: 'Does this itch?' A wheal with itch is symptomatic dermographism — a disease you treat with a second-generation antihistamine; a wheal without itch is the asymptomatic 'writing skin' of one in twenty healthy people, who needs reassurance, not medication. The second pearl guards against being fooled: if a patient with a classic history shows no wheal at all, ask when they last took an antihistamine — a recent dose suppresses the response and produces a false-negative, and the test should be repeated after a drug-free interval before you call it negative.