Page 1 of 12
DR14.1-2 | Urticaria Angioedema Classification and Management — SDL Guide
Learning Objectives
- Classify urticaria by duration (acute vs chronic) and by trigger pattern (spontaneous vs inducible), and classify angioedema by underlying mechanism (histamine-mediated vs bradykinin-mediated)
- Describe the etio-pathogenesis of urticaria and angioedema, centred on mast-cell mediator release, and list the major precipitating factors
- Identify the clinical features of urticaria and angioedema and distinguish them from important mimics, particularly urticarial vasculitis
- Outline the stepwise, antihistamine-first management of urticaria and recognise angioedema with airway compromise as a medical emergency requiring adrenaline
INSTRUCTIONS
Urticaria is one of the commonest reasons a patient presents to a dermatology or general clinic, and most cases are benign and self-limiting. Yet within this common complaint hide a few patterns you must never miss: the deeper swelling of angioedema that can threaten the airway, the bradykinin-mediated angioedema of an ACE-inhibitor that will not respond to your antihistamine, and the urticaria-like rash of urticarial vasculitis that signals a different disease altogether. This module gives you a clean classification framework, the pathogenesis that explains why antihistamines work (and when they will not), and a stepwise management approach aligned with current guidelines — so you can treat the common case confidently and recognise the dangerous one early.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Urticaria and Angioedema (textbook)
- Sacchidanand S, et al. (eds). IADVL Textbook of Dermatology, 4th ed. Section: Urticaria, Angioedema and Anaphylaxis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old woman arrives at the clinic distressed, holding up her forearms. Over the last three days, raised, intensely itchy pink swellings have been appearing and disappearing — a patch on her arm in the morning is gone by evening, only for new ones to erupt on her trunk and thighs. None of the individual lesions, she insists, lasts more than a few hours. This morning, something new and more frightening happened: her lower lip and one eyelid swelled grotesquely, without much itch, and the swelling has persisted. She has been taking ibuprofen for a sprained ankle. This single patient illustrates the two faces of the same disease process — the fleeting, superficial wheal of urticaria and the deeper, longer-lasting swelling of angioedema — and raises the question every clinician must answer: which of these is harmless, and which could obstruct an airway?
WHY THIS MATTERS
Urticaria affects up to one in five people at some point in life, so you will meet it in every clinical setting — the medicine OPD, the casualty, the dermatology clinic, and the ward where a patient reacts to a drug you prescribed. Knowing how to classify it tells you whether to reassure and treat empirically (the common acute case) or to investigate and escalate (the refractory chronic case). Knowing the pathogenesis tells you why a second-generation antihistamine is your first move — and, crucially, why that same antihistamine will fail the patient whose angioedema is caused by an ACE-inhibitor. Recognising angioedema of the airway as an emergency, and reaching for adrenaline rather than an antihistamine, is a decision that can save a life within minutes. These are not specialist skills; they are core competencies for any doctor who prescribes drugs and sees acutely unwell patients.
RECALL
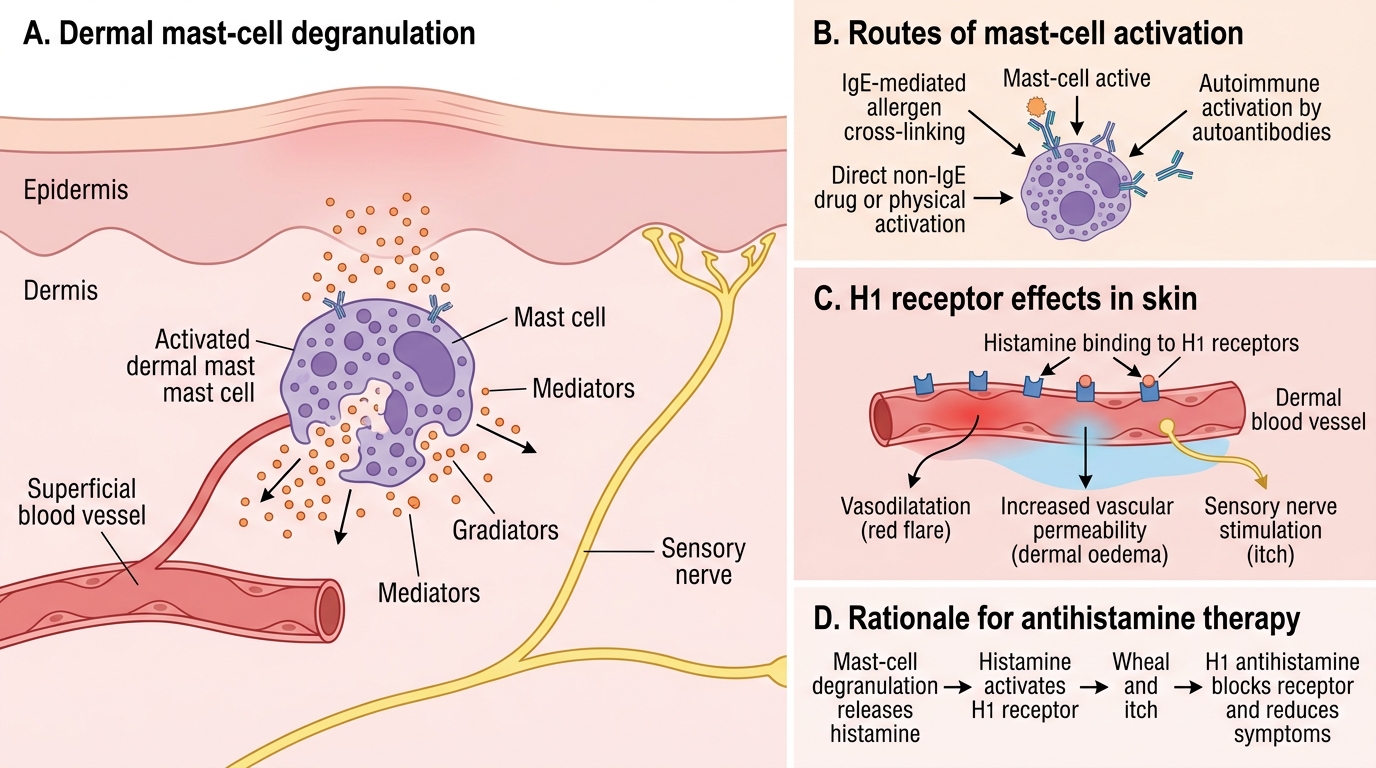
Before we begin, recall from your physiology and pharmacology of inflammation the role of the mast cell — a tissue-resident cell whose cytoplasmic granules are packed with preformed histamine and which, on degranulation, releases histamine, prostaglandins, and leukotrienes. Recall that histamine acting on H1 receptors on dermal blood vessels causes vasodilatation (redness), increased vascular permeability (oedema/swelling), and stimulation of sensory nerve endings (itch) — the exact triad you see in a wheal. Recall too the concept of anaphylaxis as a systemic, IgE-mediated hypersensitivity reaction, and that its definitive treatment is intramuscular adrenaline. These prior concepts are the foundation on which the entire logic of urticaria and angioedema — and its treatment — is built.
The Wheal and the Swell — Recognising Urticaria and Angioedema
Recognising Urticaria and Angioedema
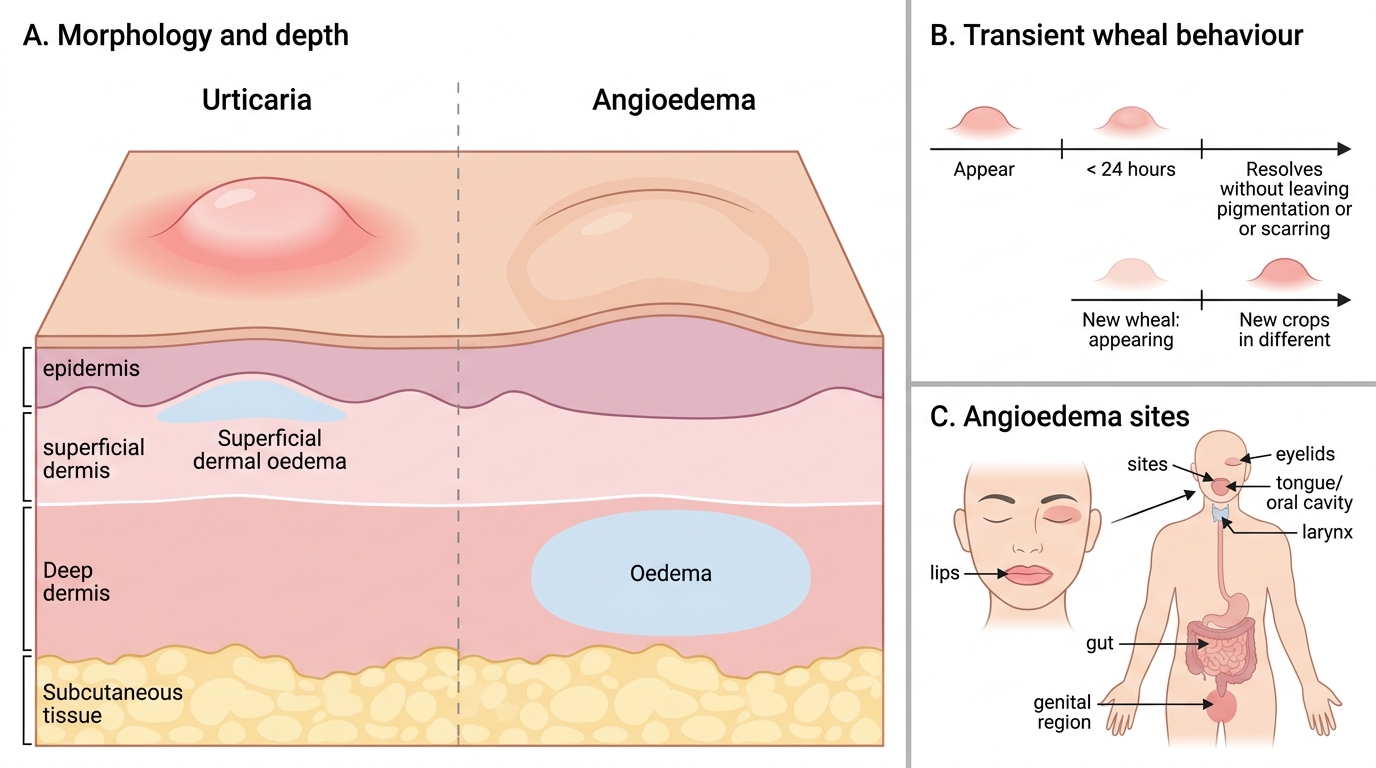
The starting point in any patient with intermittent skin swellings is to decide what you are actually looking at, because urticaria and angioedema are distinguished not by laboratory tests but by the morphology and behaviour of the lesions themselves. The defining lesion of urticaria is the wheal (hive): a raised, well-demarcated, pink-to-pale swelling surrounded by a red flare, caused by oedema of the superficial dermis. Two features are diagnostic and must be sought in the history. First, wheals are intensely pruritic. Second — and this is the single most important fact in the whole topic — any individual wheal is transient, lasting less than 24 hours before resolving completely without leaving a mark. The eruption as a whole may persist for days or weeks because fresh crops keep appearing, but each lesion is fleeting. If a patient tells you a particular swelling has stayed in the same place for two days, you are no longer dealing with simple urticaria.
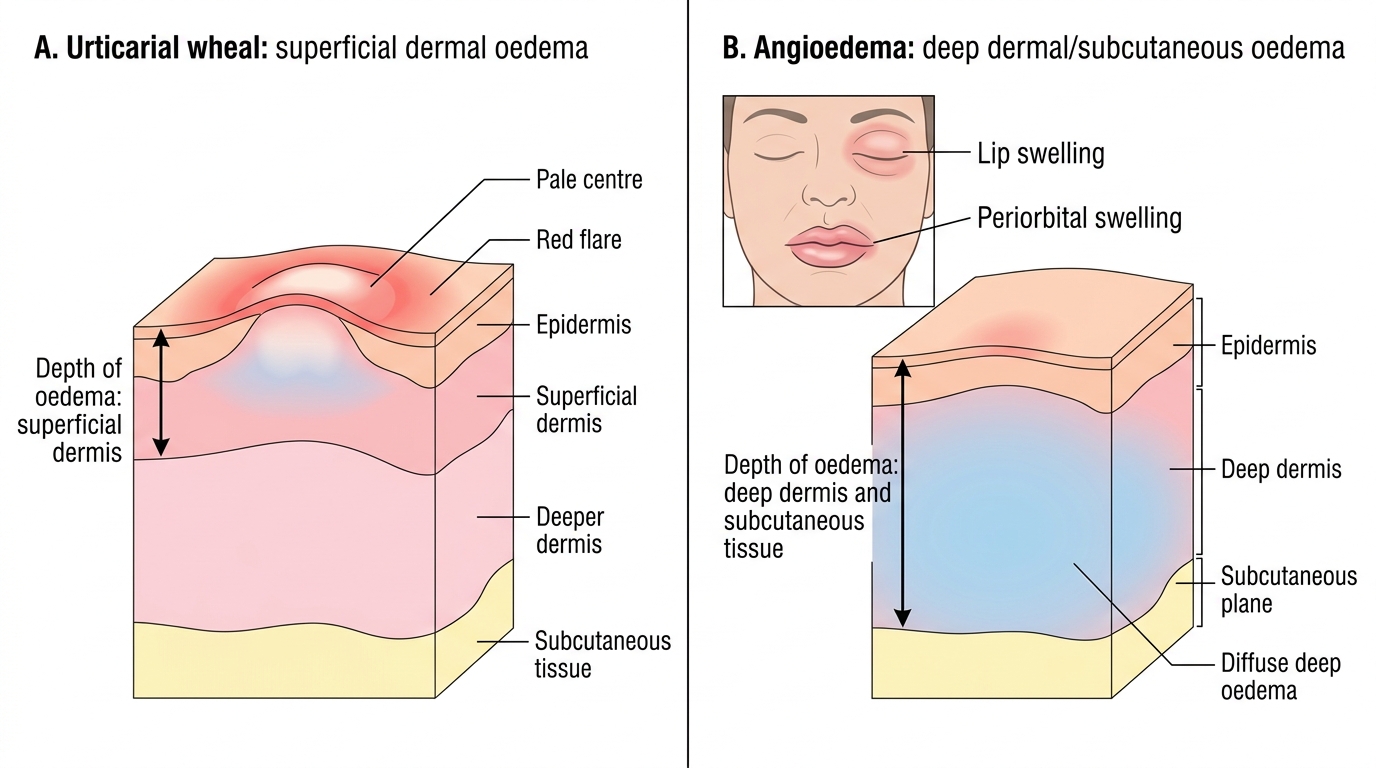
Angioedema is the same pathological process occurring at a deeper level: oedema of the deep dermis and subcutaneous or submucosal tissue. Because the swelling is deeper, it is less well-defined, often skin-coloured rather than red, and characteristically affects loose tissues — the lips, eyelids, tongue, genitalia, and the lining of the larynx and gut. Compared with wheals, angioedema is less pruritic (the itch nerves are more superficial), more often painful or tense, and lasts longer, typically resolving over hours to a couple of days rather than minutes to hours. Urticaria and angioedema frequently coexist — as in our patient — but either can occur alone. The clinical reason this distinction matters is depth and site: a wheal is never dangerous in itself, whereas angioedema of the tongue or larynx can obstruct the airway.
Urticaria Versus Angioedema: Depth of Oedema
In summary, the key discriminators are:
- Wheal (urticaria): superficial dermal oedema; raised, red/pale, very itchy; each lesion lasts <24 hours.
- Angioedema: deep dermal/subcutaneous oedema; diffuse, skin-coloured, less itchy, often painful; lasts hours to days; predilection for lips, eyelids, tongue, larynx.
Classification: Acute vs Chronic, Spontaneous vs Inducible
Classification of Urticaria
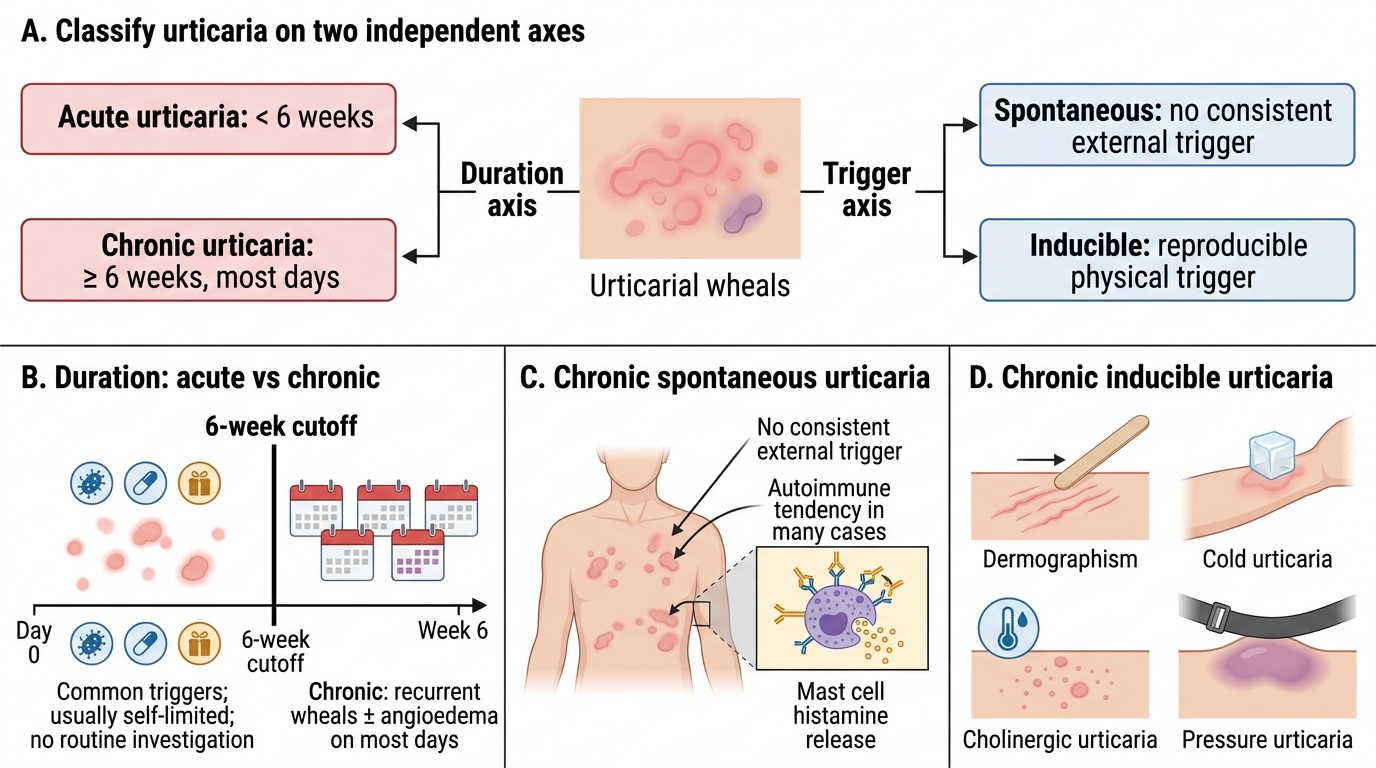
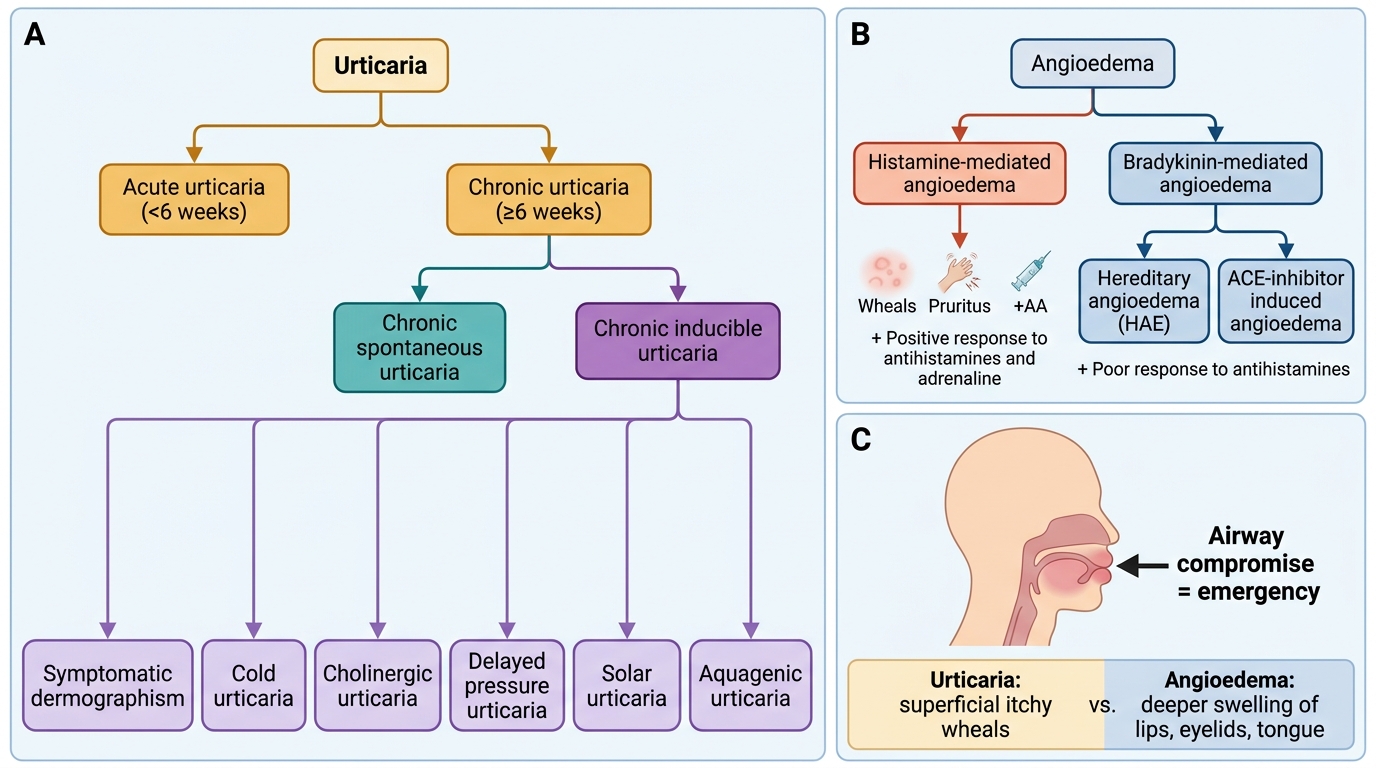
Once you have identified urticaria, the next clinical task is to classify it, because the classification directly determines how aggressively you investigate and treat. Urticaria is classified along two independent axes, and a complete diagnosis names both. The first axis is duration, which separates urticaria into acute and chronic forms using a clean, memorisable cut-off. Acute urticaria is defined as an eruption lasting less than 6 weeks; it is by far the commonest form, is frequently triggered by an infection, drug, or food, and usually settles spontaneously without ever needing investigation. Chronic urticaria is defined as wheals (with or without angioedema) recurring on most days for 6 weeks or longer; this form warrants a more considered approach because an ongoing trigger or an underlying autoimmune tendency is more likely.
The second axis applies mainly to chronic disease and asks whether a trigger can be identified. Chronic spontaneous urticaria occurs without any consistent external trigger — wheals simply appear, and in many cases an autoimmune mechanism (autoantibodies against the IgE receptor) underlies the disease. Chronic inducible urticaria is the opposite: wheals are reproducibly provoked by a specific physical stimulus, and the type is named after that stimulus. The inducible subtypes you should recognise are dermographism (wheals where the skin is stroked or scratched), cold urticaria, cholinergic urticaria (small wheals on sweating, heat, or exertion), delayed pressure urticaria, and solar urticaria. Distinguishing spontaneous from inducible disease is practically useful: an inducible urticaria can often be confirmed at the bedside with a simple provocation test and managed largely by avoiding the trigger.
Classification of Urticaria and Angioedema
A practical way to hold the framework:
- By duration: acute (<6 weeks) vs chronic (≥6 weeks).
- Chronic by trigger: spontaneous (no consistent trigger; often autoimmune) vs inducible (reproducibly provoked).
- Inducible subtypes: dermographism, cold, cholinergic, pressure, solar, aquagenic.
SELF-CHECK
A patient reports that individual itchy swellings on her skin each persist for about 36 hours, are painful rather than itchy, and leave a brownish stain when they fade. Why should this NOT be diagnosed as simple urticaria?
A. Because urticaria is always painless and never itchy
B. Because individual urticarial wheals last less than 24 hours and resolve without a mark; lesions persisting >24 hours that are painful and resolve with bruising/pigmentation suggest urticarial vasculitis
C. Because urticaria only occurs in patients over the age of 60
D. Because urticaria cannot be associated with any systemic symptoms
Reveal Answer
Answer: B. Because individual urticarial wheals last less than 24 hours and resolve without a mark; lesions persisting >24 hours that are painful and resolve with bruising/pigmentation suggest urticarial vasculitis
The cardinal rule of urticaria is that any individual wheal is transient, lasting less than 24 hours, and resolves completely without leaving a mark. Lesions that persist beyond 24 hours, are painful or burning rather than purely itchy, and fade leaving bruising or post-inflammatory pigmentation point away from ordinary urticaria and towards urticarial vasculitis — a small-vessel vasculitis that requires a skin biopsy to confirm and a different management approach. Recognising this distinction at the bedside, simply from the duration and behaviour of the individual lesion, prevents the common error of treating a vasculitis as benign hives.
Pathogenesis: Mast Cell, Histamine, and Beyond
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Pathogenesis of Urticaria: Mast Cell, Histamine, and H1 Blockade
The clinical features of urticaria flow directly from a single cellular event: the activation and degranulation of the dermal mast cell. When the mast cell degranulates it releases preformed histamine together with newly synthesised mediators such as prostaglandins and leukotrienes. Histamine acting on H1 receptors on the local blood vessels produces exactly the three features of a wheal — vasodilatation (the red flare), increased vascular permeability with fluid leaking into the dermis (the raised, oedematous wheal), and stimulation of cutaneous sensory nerves (the itch). Understanding that histamine is the central mediator is what makes the entire treatment strategy logical: if histamine acting on H1 receptors causes the lesion, then a drug that blocks the H1 receptor should suppress it. This is the rationale for the antihistamine-first approach you will meet later.
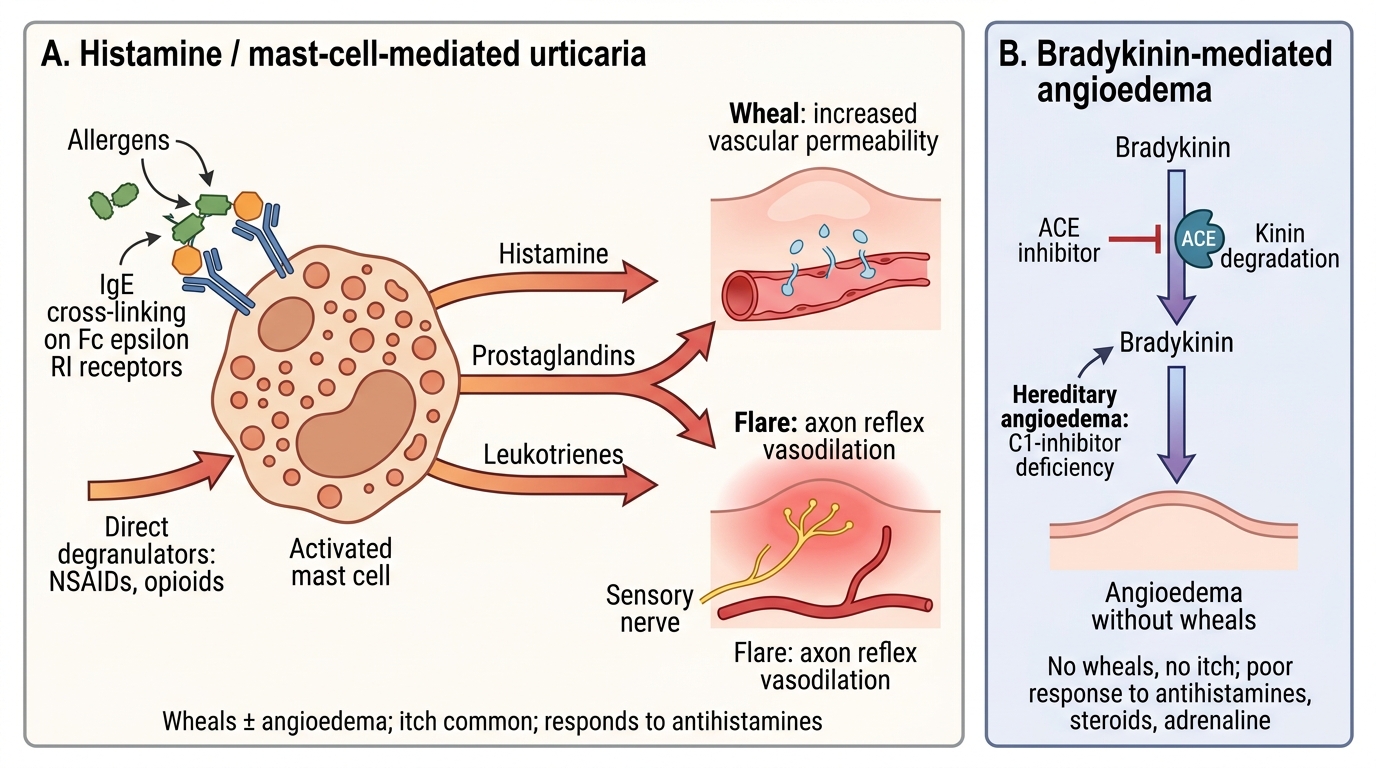
Mast cells can be triggered to degranulate by several distinct routes, and this explains why urticaria has so many causes. The classical route is IgE-mediated (type I) hypersensitivity, in which an allergen cross-links specific IgE bound to the mast-cell surface — the mechanism behind many food and drug allergies. Mast cells can also be activated directly, without IgE, by certain drugs (opioids, vancomycin) and by physical stimuli, and in chronic spontaneous urticaria by autoantibodies directed against IgE or its receptor (an autoimmune mechanism). Crucially, not all swelling is mast-cell driven. Angioedema can also be bradykinin-mediated, and this pathway involves no histamine and no mast cell at all. Bradykinin is a potent vasoactive peptide normally broken down by the enzyme that ACE-inhibitors block; when bradykinin accumulates (as in ACE-inhibitor-induced angioedema, or in hereditary angioedema from C1-esterase inhibitor deficiency), it causes deep swelling that does not itch and — vitally — does not respond to antihistamines or steroids. Recognising the two mechanistic pathways is the key to not wasting time on an ineffective drug.
Mechanisms of Urticaria and Angioedema
The two pathways to remember:
- Histamine/mast-cell-mediated: IgE-mediated, direct degranulation, or autoimmune; causes wheals ± angioedema; responds to antihistamines.
- Bradykinin-mediated: ACE-inhibitor-induced angioedema and hereditary angioedema (C1-inhibitor deficiency); no wheals, no itch; does NOT respond to antihistamines, steroids, or adrenaline in the usual way — needs specific therapy.