Page 2 of 12
DR14.1-2 | Urticaria Angioedema Classification and Management — SDL Guide (Part 2)
Precipitating Factors and Triggers
Precipitating Factors and Triggers in Urticaria and Angioedema
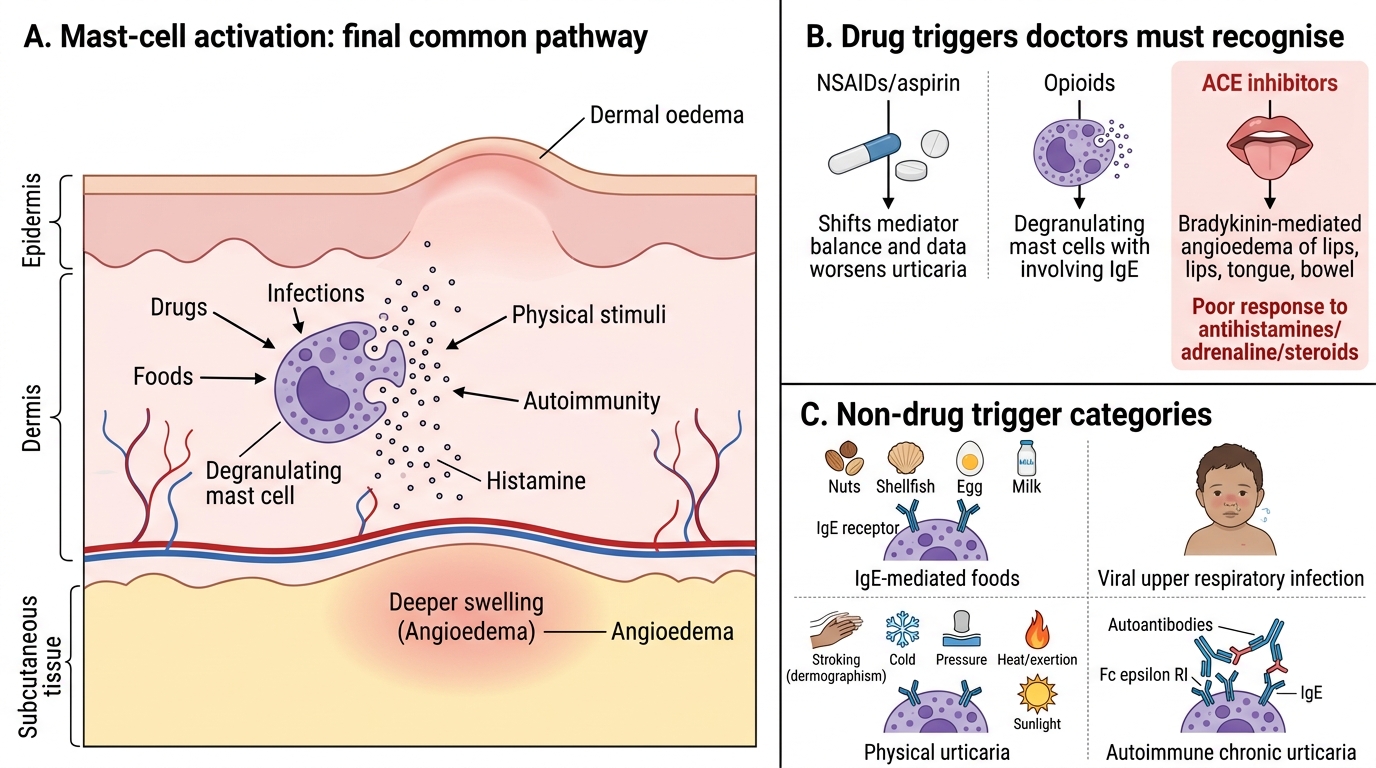
Because urticaria is a final common pathway of mast-cell activation, a wide and clinically important list of precipitants can set it off, and taking a careful trigger history is often more valuable than any blood test. The single most important group for a prescribing doctor is drugs, because these are both common and modifiable. Non-steroidal anti-inflammatory drugs (especially aspirin and other NSAIDs such as the ibuprofen our patient took) are a leading cause and can both trigger urticaria and worsen pre-existing chronic urticaria by altering mediator metabolism. Opioids cause urticaria by directly degranulating mast cells without any IgE involvement. ACE-inhibitors deserve special mention because they cause specifically bradykinin-mediated angioedema — often of the lips, tongue, or bowel — which may appear weeks to months after starting the drug and which will not respond to your usual treatment.
Beyond drugs, the major trigger categories are foods, infections, physical stimuli, and autoimmunity. Foods (and food additives) most often cause acute urticaria, classically nuts, shellfish, eggs, and milk through an IgE-mediated route. Infections — particularly viral upper respiratory infections in children, but also chronic infections — are among the commonest causes of acute urticaria and a recognised driver of chronic disease. Physical stimuli (stroking, cold, pressure, heat/exertion, sunlight) define the inducible urticarias described earlier. Finally, in chronic spontaneous urticaria an autoimmune mechanism is frequently at play, sometimes associated with autoimmune thyroid disease. Identifying and removing a modifiable trigger — stopping the NSAID, treating the infection — is frequently the most effective single intervention.
The key precipitants to commit to memory:
- Drugs: NSAIDs/aspirin and opioids (urticaria); ACE-inhibitors (bradykinin-mediated angioedema).
- Foods: nuts, shellfish, egg, milk (mainly acute, IgE-mediated).
- Infections: viral URTIs (especially in children); chronic infections.
- Physical stimuli: dermographism, cold, cholinergic, pressure, solar.
- Autoimmune: chronic spontaneous urticaria; association with autoimmune thyroid disease.
Clinical Features: History, Distribution, and Associated Signs
Clinical Features of Urticaria and Angioedema
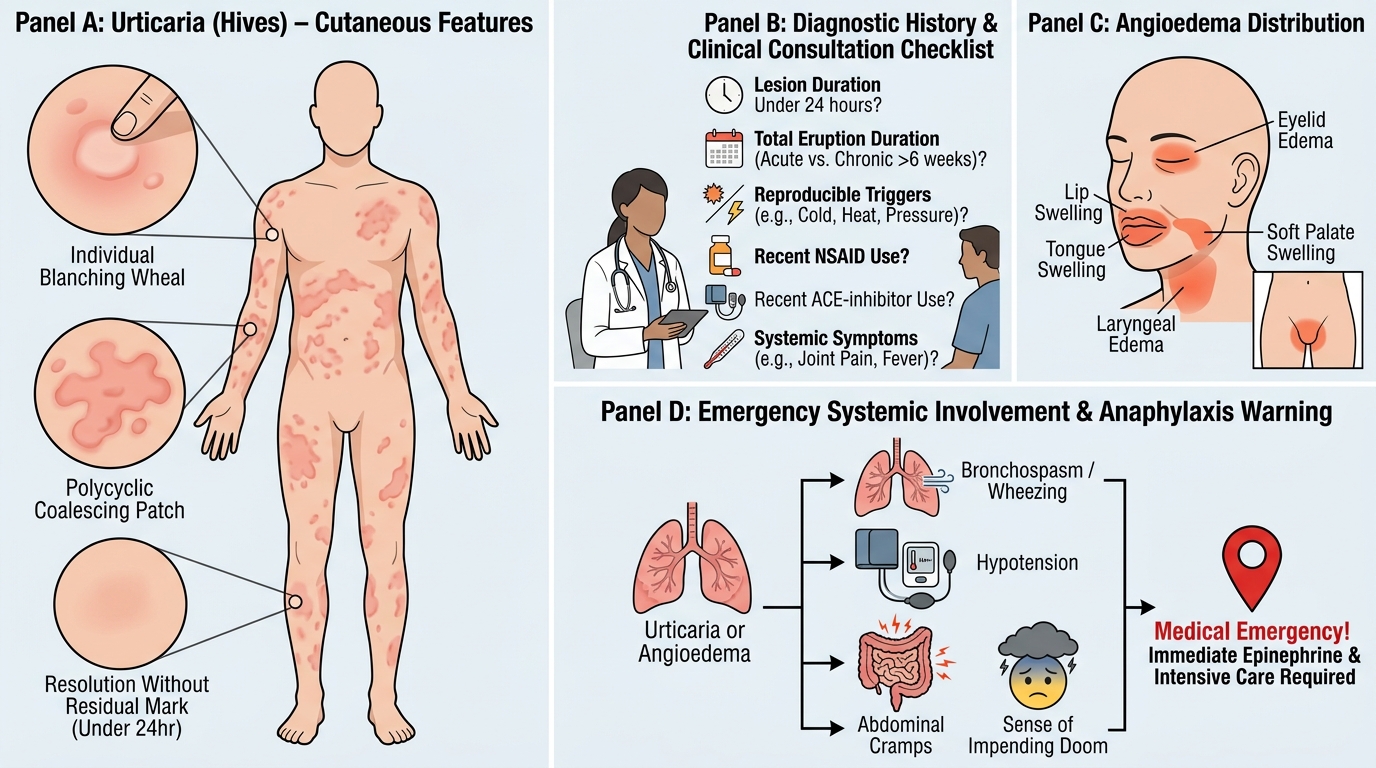
The diagnosis of urticaria and angioedema is essentially clinical, made from a focused history and examination rather than from investigations, so knowing what to ask and what to look for is the core skill. The history should establish the morphology and time-course of individual lesions (confirming that each wheal lasts under 24 hours and resolves without a mark), the total duration of the eruption (to classify it as acute or chronic), and any reproducible trigger (drugs, foods, infection, or a physical stimulus). You should specifically ask about recent drug intake — particularly NSAIDs and ACE-inhibitors — and about systemic symptoms that suggest a more serious reaction. On examination, urticarial wheals are raised, erythematous or pale, variable in size and shape, often coalescing into large polycyclic patches, and characteristically blanch on pressure; they may appear anywhere on the body.
The features that demand urgency relate to angioedema and systemic involvement. Angioedema favours loose tissues — the eyelids, lips, tongue, and genitalia — and when it involves the tongue, soft palate, or larynx it can compromise the airway, producing a change in voice, difficulty swallowing, or stridor. The combination of urticaria/angioedema with bronchospasm, hypotension, abdominal cramps, or a sense of impending doom indicates anaphylaxis, a systemic and potentially fatal reaction that is a medical emergency. Every patient with acute urticaria must therefore be assessed for these red-flag features before being reassured. Recognising the difference between a patient with itchy hives and a patient whose tongue is swelling is the most important clinical judgement in this topic.
The clinical checklist:
- Wheals: raised, itchy, blanching, variable size, each lasting <24 hours.
- Angioedema sites: eyelids, lips, tongue, larynx (airway risk), genitalia.
- Red flags (anaphylaxis): voice change/stridor, breathlessness/wheeze, hypotension, abdominal cramps — treat as an emergency.
Distinguishing Urticaria and Angioedema from Mimics
Distinguishing Urticaria and Angioedema from Mimics
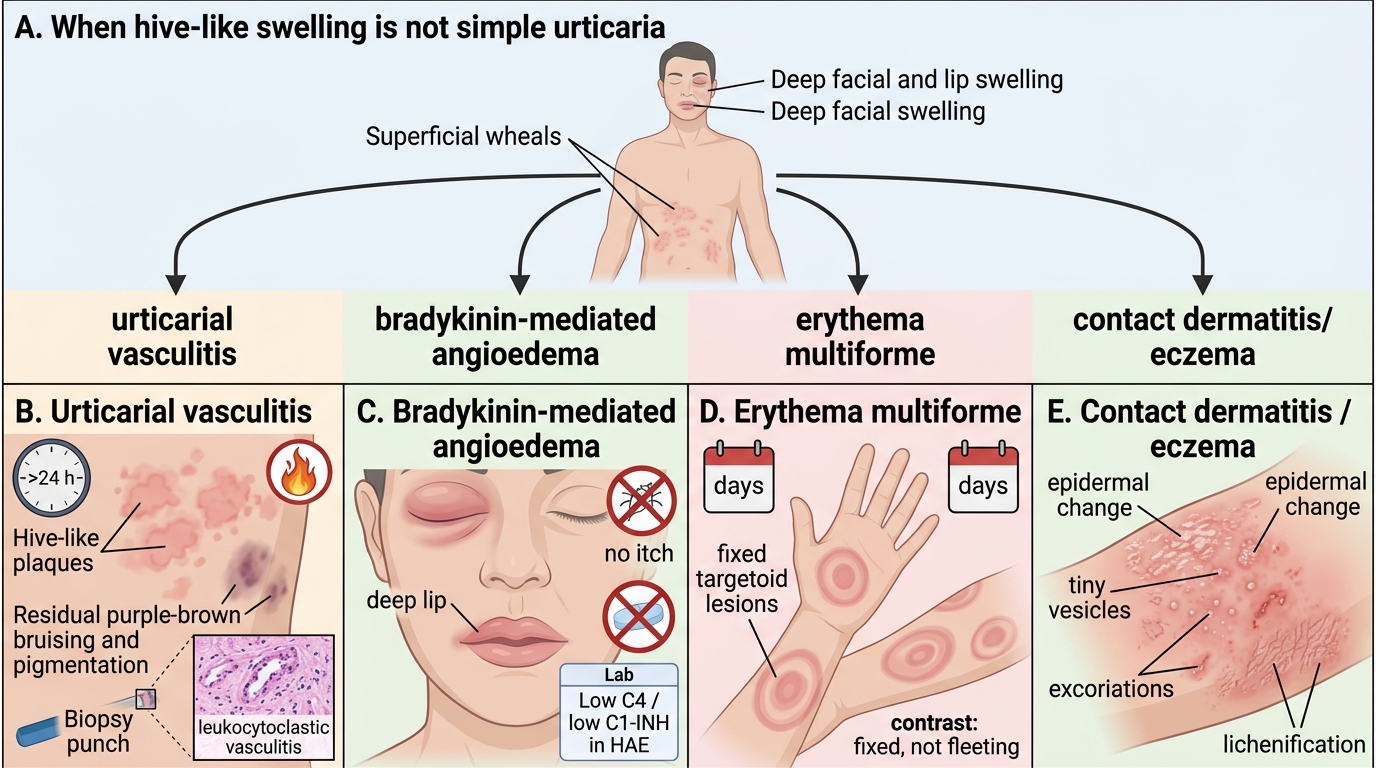
Several conditions can be mistaken for urticaria or angioedema, and distinguishing them is important because their management and prognosis differ substantially. The single most important mimic to exclude is urticarial vasculitis, a small-vessel vasculitis whose lesions look superficially like hives but behave quite differently: individual lesions persist for more than 24 hours, are often painful or burning rather than purely itchy, and resolve leaving bruising or post-inflammatory pigmentation. Any of these three features should prompt a skin biopsy to look for leukocytoclastic vasculitis, and investigation for an associated systemic disease (connective tissue disease, low complement). A second important mimic is bradykinin-mediated angioedema — ACE-inhibitor-induced or hereditary angioedema — which presents as recurrent deep swelling without any wheals or itch; the absence of urticaria and the failure to respond to antihistamines are the clues, and hereditary angioedema is confirmed by low C4 and C1-esterase inhibitor levels.
Other conditions occasionally enter the differential. Erythema multiforme produces fixed, targetoid lesions that, unlike wheals, persist in the same site for days. Contact dermatitis and eczema show epidermal changes (scaling, vesicles, lichenification) that are absent in pure urticaria, and they too remain fixed. Where chronic urticaria is suspected, a limited panel of investigations is reasonable — a full blood count, ESR/CRP (a raised inflammatory marker hints at vasculitis rather than simple urticaria), thyroid function and thyroid autoantibodies, and, if vasculitis is suspected, complement levels (C3/C4) and a biopsy. The guiding principle is that simple urticaria needs little or no investigation, while persistent, painful, or bruising lesions, or angioedema without wheals, are the signals that warrant a more thorough work-up.
Differential Diagnosis of Urticarial and Angioedema-Like Presentations
The discriminators to remember:
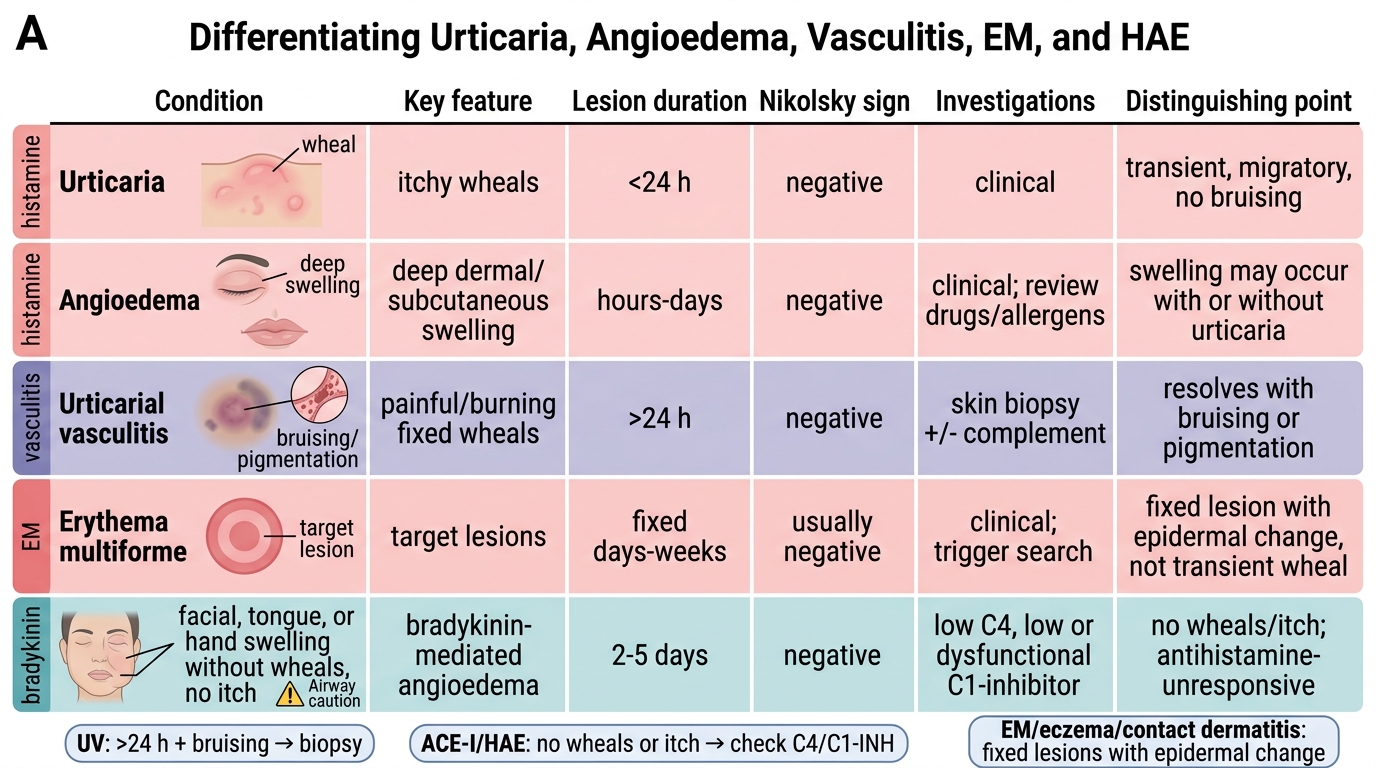
- Urticarial vasculitis: lesions >24 hours, painful, resolve with bruising/pigmentation → biopsy.
- Bradykinin angioedema (ACE-I/HAE): swelling without wheals or itch; antihistamine-unresponsive; HAE has low C4 and C1-inhibitor.
- Erythema multiforme / contact dermatitis / eczema: fixed lesions with epidermal change, not transient wheals.