Page 2 of 22
DR8.1 | Common Viral Skin Infection Foundations — SDL Guide (Part 2)
Clinical Presentations: Family-Level Morphological Signatures
Morphological Signatures of Common Viral Skin Infections
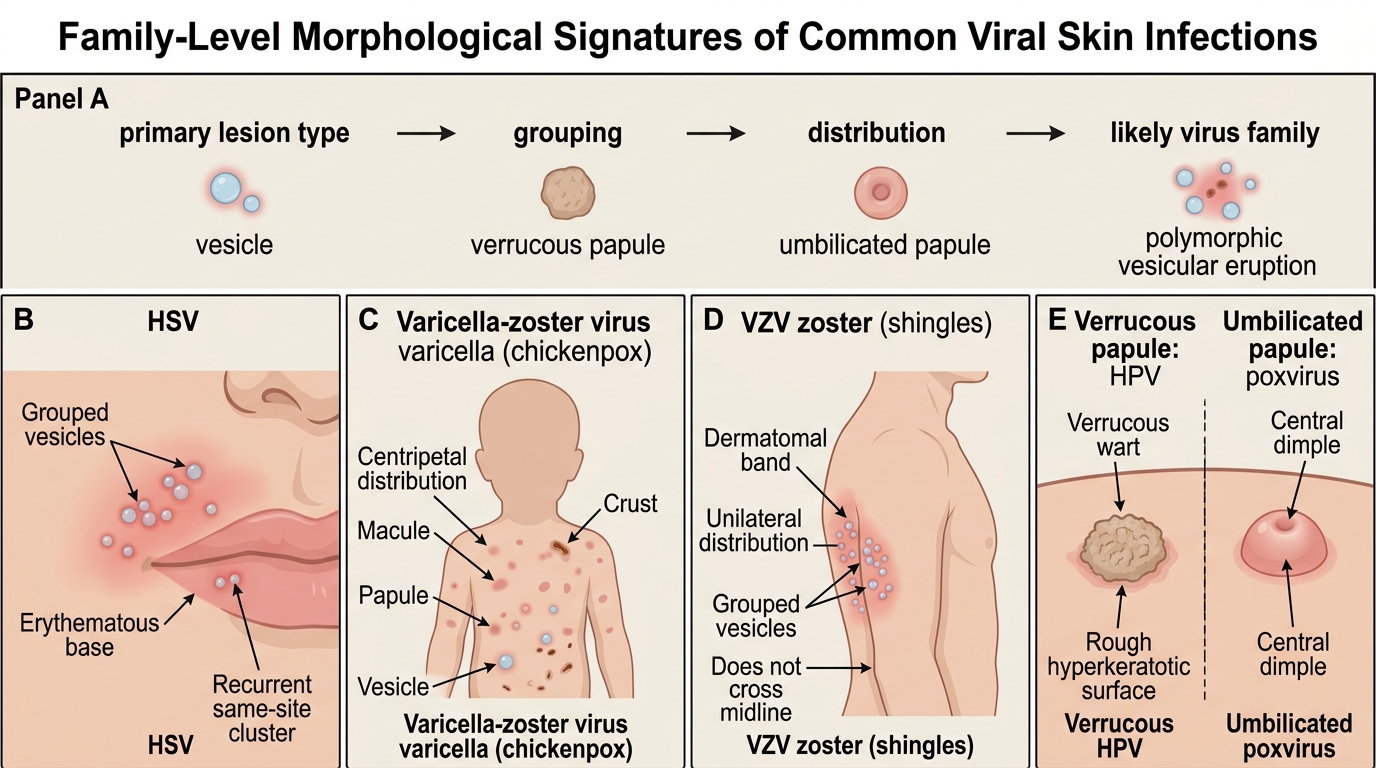
Each virus family announces itself with a morphological signature that, once learned, allows rapid bedside recognition. The diagnostic discipline at this foundational level is to read the primary lesion type, its grouping and its distribution, and to ask which family that pattern fits — before reaching for any investigation. A vesicle is not the same as a verrucous papule, and a papule with a central dimple is not the same as one with a rough warty surface; these distinctions are visible to the naked eye and carry most of the diagnostic weight. Distribution adds a second, equally powerful layer of information: a localised cluster, a dermatomal band, a centripetal trunk-predominant eruption, and scattered crops each point toward a different family. The signatures below cover the overwhelming majority of cutaneous viral infections in adults and children, and learning to name them on sight is the foundation on which the focused recognition SDLs build.
- Grouped vesicles on an erythematous base (HSV): clusters of small, tense, fluid-filled vesicles sitting on a red base, typically perioral (HSV-1, herpes labialis) or genital (HSV-2), often preceded by tingling and recurring at the same site.
- Polymorphic vesicular eruption in different stages (varicella): a centripetal eruption (trunk more than limbs) in which macules, papules, vesicles and crusts are all present at the same time — the classic 'dewdrop on a rose petal' vesicle — distinguishing it from smallpox, where lesions are all at the same stage.
- Dermatomal grouped vesicles (herpes zoster): a band of grouped vesicles confined to a single dermatome, unilateral, that does not cross the midline, often with preceding dermatomal pain.
- Verrucous papule with black dots (HPV warts): a firm, rough, hyperkeratotic papule with the skin lines interrupted and tiny black dots (thrombosed capillaries) on the surface.
- Pearly umbilicated papule (molluscum contagiosum): a dome-shaped, flesh-coloured or pearly papule with a central dimple (umbilication), often in crops.
Reading these signatures correctly is the heart of recognition; the specific recognition SDLs that follow refine each one.
Differentiating Cutaneous Viral Infections: A Framework
Framework for Differentiating Cutaneous Viral Infections
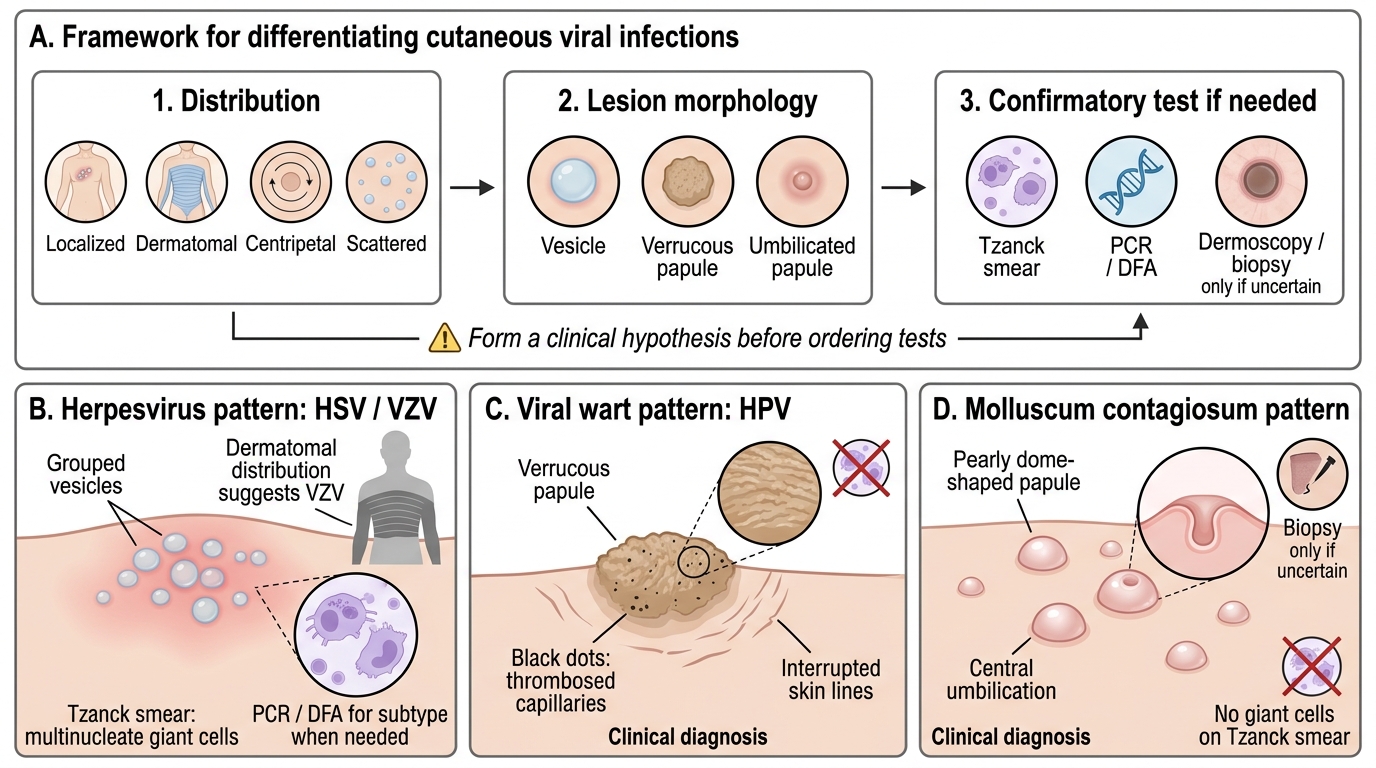
When the morphological signature alone is not decisive, a small set of differentiating features and bedside investigations resolves most cases. The framework is to combine three readings — distribution (localised, dermatomal, centripetal or scattered), lesion type (vesicle, verrucous papule, umbilicated papule), and a confirmatory bedside test where needed. Investigations are used to confirm a clinical impression, not to replace it, and the choice of test follows directly from which family you suspect. It is a common error to order a test before forming a clinical hypothesis; the better discipline is to decide which family the lesion belongs to and then select the one investigation that confirms or refutes it. For herpesviruses that test is the Tzanck smear (with PCR or DFA in reserve); for warts and molluscum the diagnosis is usually clinical, with dermoscopy or biopsy held for genuinely uncertain lesions. Approaching investigations this way avoids unnecessary tests and keeps the reasoning transparent.
The practical decision points are:
- A Tzanck smear is useful only when you suspect a herpesvirus (HSV or VZV); multinucleate giant cells confirm the family but not the specific virus, so reach for PCR or DFA when subtype identification matters (e.g., neonatal or atypical disease).
- Warts and molluscum are clinical diagnoses — neither shows giant cells on Tzanck smear. A wart is verrucous with black dots and interrupted skin lines; molluscum is dome-shaped with a central dell. When uncertain, dermoscopy and, rarely, biopsy (koilocytes for HPV; Henderson-Paterson bodies for MCV) settle the question.
- Distribution is a powerful discriminator: dermatomal and unilateral points to zoster; centripetal with mixed lesion stages points to varicella; localised grouped vesicles point to HSV.
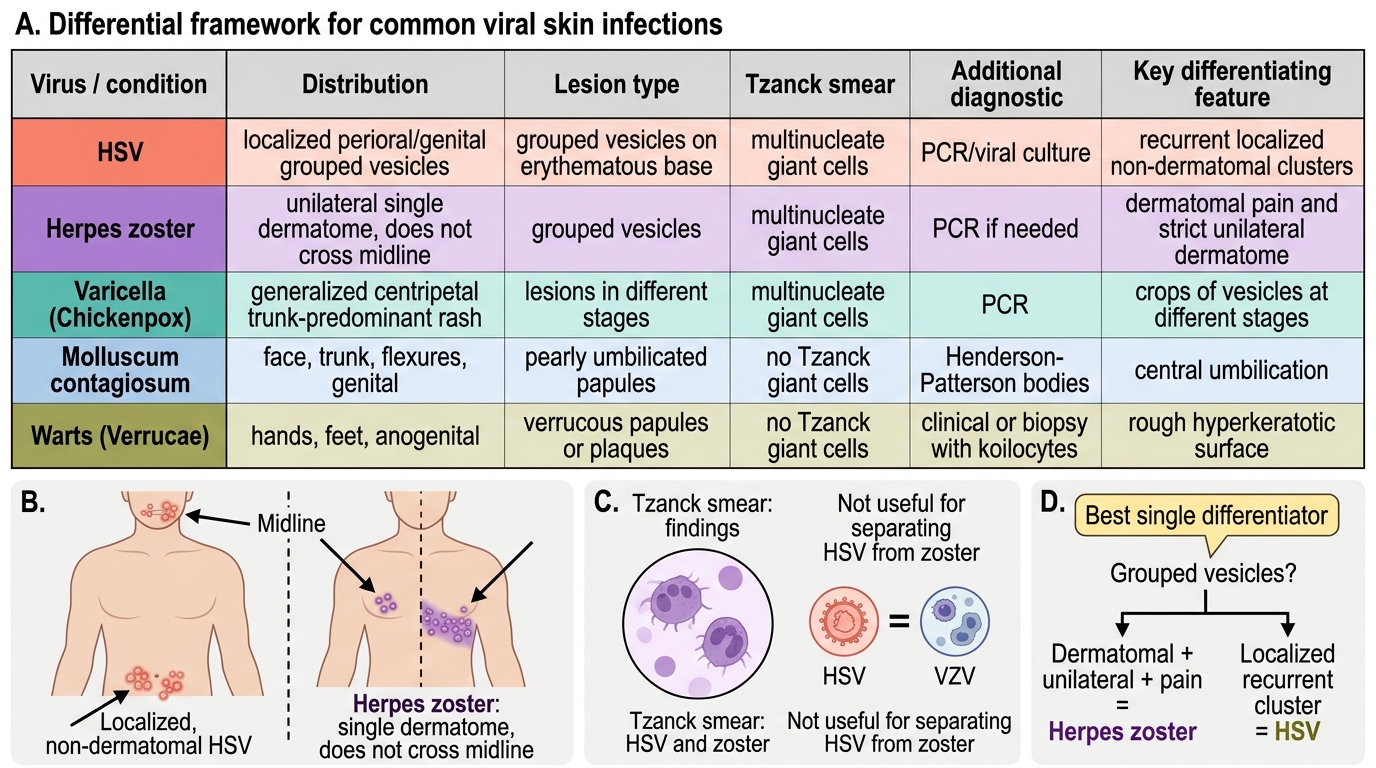
The summary table below consolidates these discriminators across the common entities.
Differentiating Common Viral Skin Infections
SELF-CHECK
Which single feature best distinguishes herpes zoster from a cluster of herpes simplex lesions?
A. Herpes zoster shows multinucleate giant cells on Tzanck smear, whereas herpes simplex does not
B. Herpes zoster is confined to one dermatome and does not cross the midline, whereas herpes simplex is localised but not dermatomal
C. Herpes zoster lesions are umbilicated papules, whereas herpes simplex lesions are warty
D. Herpes zoster is caused by a poxvirus, whereas herpes simplex is caused by a papillomavirus
Reveal Answer
Answer: B. Herpes zoster is confined to one dermatome and does not cross the midline, whereas herpes simplex is localised but not dermatomal
Both herpes zoster and herpes simplex are herpesviruses and both show multinucleate giant cells on Tzanck smear, so cytology does not separate them. The decisive clinical discriminator is distribution: herpes zoster (VZV reactivation) is confined to a single dermatome, is unilateral, and characteristically does not cross the midline, often with preceding dermatomal pain. Herpes simplex produces localised grouped vesicles (perioral or genital) that are not dermatomal. Neither is caused by a poxvirus or papillomavirus — those families produce molluscum and warts respectively.
Management Principles Across Viral Skin Infections
Management Principles Across Viral Skin Infections
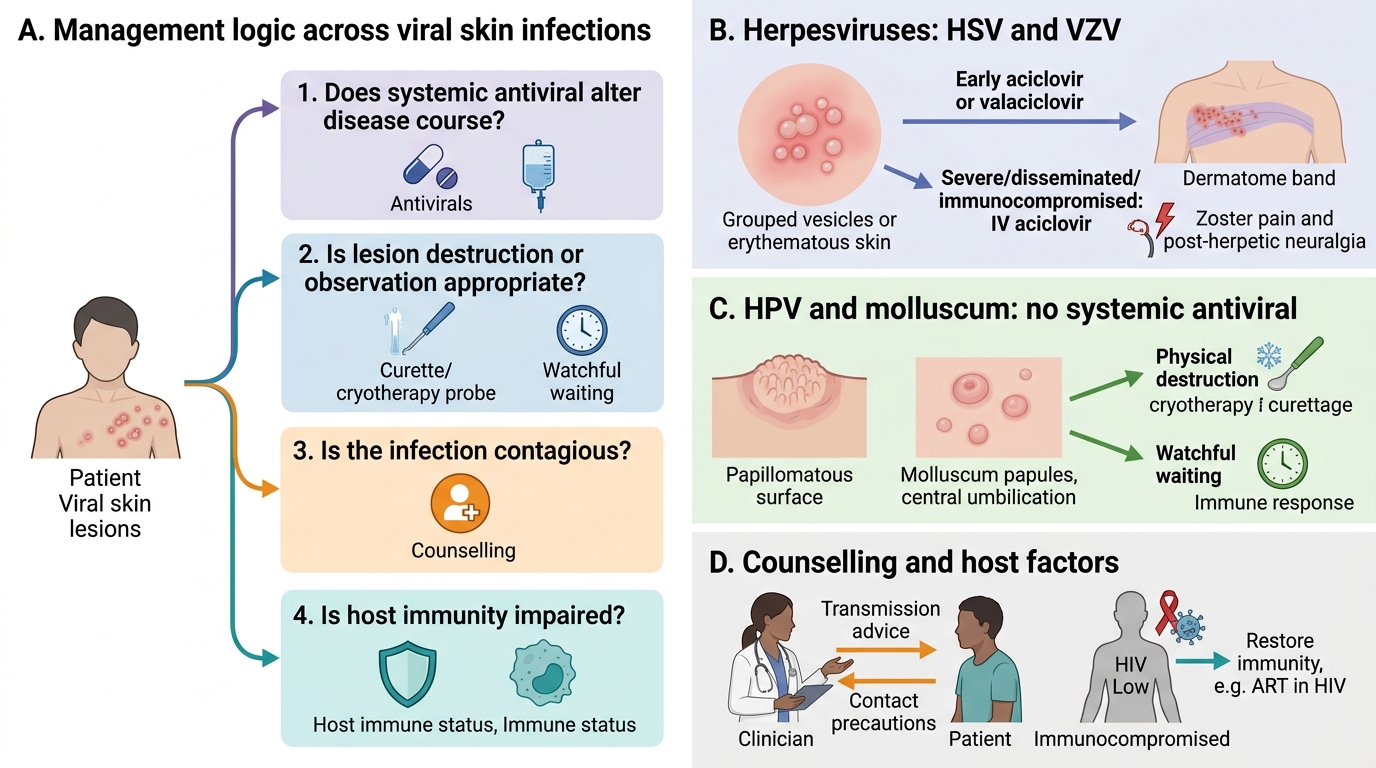
Management across cutaneous viral infections follows family-specific logic, and the most important early decision is whether a systemic antiviral genuinely alters the course. For the herpesviruses, antivirals shorten and attenuate disease and are most effective when started early; for HPV and molluscum, no systemic antiviral exists and treatment is either physical destruction or watchful waiting, since many lesions resolve as immunity controls the virus. Layered onto this is the public-health dimension: several of these infections are contagious, and counselling on transmission and contact precautions is part of management rather than an afterthought. A further consideration is the host: extensive or atypical disease in an immunocompromised patient may need more aggressive or prolonged treatment, and restoring immunity (for example, antiretroviral therapy in HIV) can be the single most effective intervention. Holding these threads together — antiviral logic, physical treatment, contagion counselling and host immune status — is what separates rote prescribing from sound management.
The principles by family are:
- Herpesviruses (HSV, VZV): nucleoside analogue antivirals — aciclovir or valaciclovir — are the mainstay; they are most effective when started early. Severe, disseminated or immunocompromised disease warrants intravenous aciclovir. Herpes zoster additionally requires attention to pain and to post-herpetic neuralgia.
- HPV warts: there is no systemic antiviral; treatment is destructive or keratolytic — cryotherapy, electrocautery, salicylic acid — and many warts eventually clear spontaneously as cell-mediated immunity develops.
- Molluscum contagiosum: often self-limiting in immunocompetent people; when treatment is wanted, options are physical (cryotherapy, curettage) or topical. In HIV, restoring immunity with antiretroviral therapy is the key intervention.
- Across all: counsel on transmission — avoid skin-to-skin contact while lesions are active, do not share towels/razors, and screen for sexually transmitted co-infection where the distribution is genital.
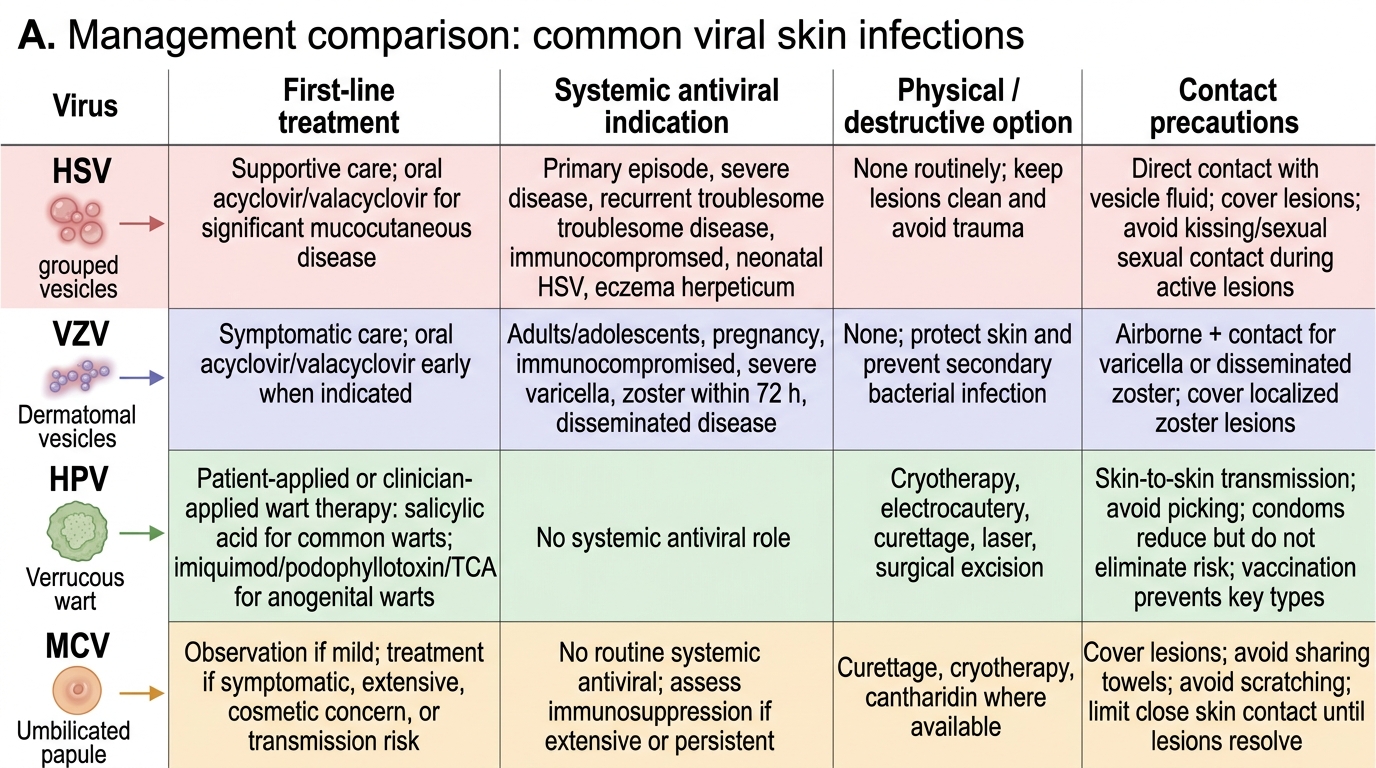
Management of Common Viral Skin Infections