Page 3 of 22
DR8.1 | Common Viral Skin Infection Foundations — SDL Guide (Part 3)
Self-Assessment: Viral Infections at a Glance
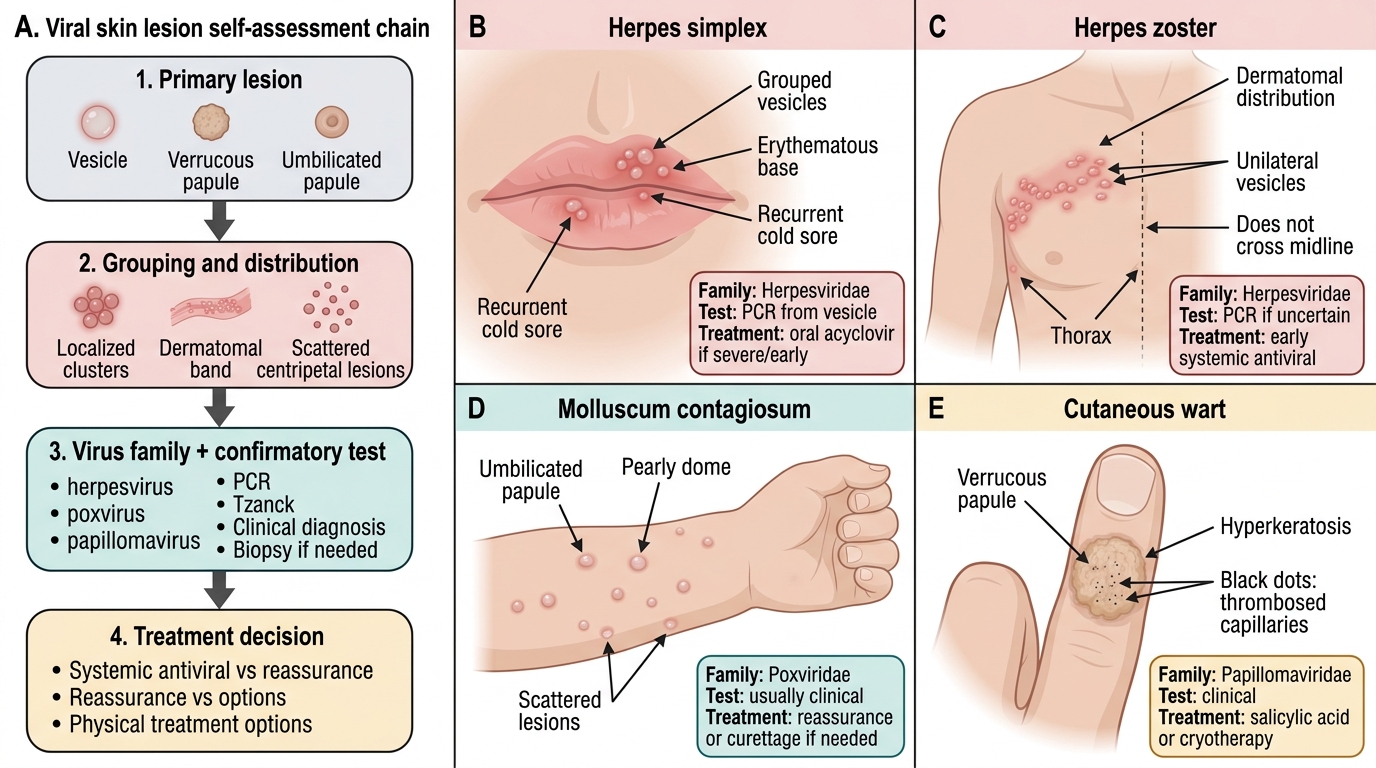
Viral Skin Infections: Recognition Chain
Consolidating the framework, the goal of this closing section is to test whether you can move from a clinical description to the correct virus family and then to the right next step. The discipline that distinguishes a confident clinician is reading the lesion type, grouping and distribution first, and only then selecting a confirmatory test or treatment — exactly the sequence this SDL has built. Recognition is not a single act of pattern-matching but a short ordered chain of questions, and rehearsing that chain until it becomes automatic is the purpose of self-assessment. The scenarios you should be able to handle range from the everyday cold sore and the schoolchild's molluscum to the painful dermatomal band of shingles and the rough, black-dotted wart on a finger. Use the self-check below to rehearse the sequence across these common entities, and notice where you hesitate — those are the points to revisit in the focused recognition SDLs.
Work through each scenario by asking, in order:
- What is the primary lesion (vesicle, verrucous papule, umbilicated papule)?
- How is it grouped and distributed (localised, dermatomal, centripetal, scattered)?
- Which family does that pattern fit, and what is the single best confirmatory test?
- Does a systemic antiviral change the outcome here, or is the right answer reassurance or a physical treatment?
These four questions, applied in sequence, will carry you correctly through the large majority of cutaneous viral infections — and they are the throughline into the focused recognition SDLs on herpes simplex, varicella zoster, viral warts and molluscum contagiosum that follow.
SELF-CHECK
A young adult presents with crops of pearly, dome-shaped papules each with a central dimple, scattered on the trunk. There is no preceding pain and no dermatomal pattern. What is the most appropriate next step?
A. Start systemic aciclovir, as this is reactivated herpes zoster
B. Diagnose molluscum contagiosum clinically; reassure (often self-limiting) or offer physical removal such as cryotherapy or curettage — no systemic antiviral
C. Perform a Tzanck smear expecting multinucleate giant cells to confirm the diagnosis
D. Prescribe oral antibiotics for presumed bacterial folliculitis
Reveal Answer
Answer: B. Diagnose molluscum contagiosum clinically; reassure (often self-limiting) or offer physical removal such as cryotherapy or curettage — no systemic antiviral
Pearly, dome-shaped papules with central umbilication are the signature of molluscum contagiosum, a poxvirus infection. It is a clinical diagnosis — a Tzanck smear would not show multinucleate giant cells (those are seen in herpesvirus infections), and there is no systemic antiviral for molluscum. In immunocompetent people the condition is often self-limiting, so reassurance is reasonable; when treatment is desired, physical methods such as cryotherapy or curettage are appropriate. Aciclovir treats herpesviruses, not poxviruses, and antibiotics are not indicated for a viral papular eruption.
CLINICAL PEARL
The single most useful bedside discriminator across cutaneous viral infections is the primary lesion type read together with its distribution. Grouped vesicles on an erythematous base mean a herpesvirus — localised for HSV, dermatomal for zoster, centripetal with mixed stages for varicella. A verrucous papule with black dots means HPV. A pearly papule with a central dell means molluscum. Reach for a Tzanck smear only when you suspect a herpesvirus, and remember it confirms the family but never the specific virus. Extensive, atypical or giant molluscum, or unusually severe herpes infections, should prompt you to consider underlying immunosuppression such as HIV.