Page 15 of 22
DR8.5 | Molluscum Contagiosum Recognition — SDL Guide
Learning Objectives
- Recognise molluscum contagiosum by its pearly, dome-shaped, centrally umbilicated papules across its three clinical contexts (children, sexually active adults, immunocompromised)
- Explain MCV pathogenesis as a poxvirus with cytoplasmic replication and Henderson-Paterson inclusion bodies
- Describe the clinical features of molluscum in children, as a sexually transmitted infection in adults, and as extensive/atypical disease in HIV
- Differentiate molluscum from viral warts, milia and other mimics, and outline physical and topical management including the role of immune restoration in HIV
INSTRUCTIONS
Molluscum contagiosum is a common, benign poxvirus infection of the skin that you will see frequently in children and, in different contexts, in sexually active adults and in immunocompromised patients. This SDL builds the skill of recognising its unmistakable signature — pearly, dome-shaped papules with a central dimple (umbilication) — and of reading the clinical context, because the same lesion means something different in a healthy child, in an adult with genital lesions, and in an HIV patient with extensive atypical disease. Recognising the central dell, knowing the histological hallmark (Henderson-Paterson bodies), distinguishing molluscum from warts and milia, and choosing physical or topical treatment (or watchful waiting) are the core competencies here.
References
- Khanna N. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Viral Infections (Molluscum Contagiosum) (textbook)
- Sacchidanand S (ed). IADVL Textbook of Dermatology, 4th ed. Section: Poxvirus Infections / Molluscum Contagiosum (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A mother brings her 5-year-old with a scatter of small, smooth, skin-coloured bumps across his trunk and armpits; each one, when you look closely, has a tiny dimple in its centre. A week later you see a very different patient: a young man with HIV whose face is studded with dozens of similar but larger papules, some over a centimetre across. The same poxvirus — molluscum contagiosum virus — has produced both pictures, but the pearly, umbilicated papule means a trivial, self-limiting infection in the child and a marker of advanced immunosuppression in the man. Recognising the central dimple, and then reading the clinical context, is the skill this SDL builds.
WHY THIS MATTERS
Molluscum contagiosum is a frequent presentation in paediatric and general dermatology, and recognising it correctly across its three contexts has real clinical consequences. In children it is benign and usually self-limiting, and the main task is reassurance and avoiding overtreatment. In sexually active adults, genital molluscum is a sexually transmitted infection that warrants counselling and screening for other STIs. In the immunocompromised — especially in HIV — extensive, giant or atypical molluscum can be the presenting clue to significant immunosuppression and should prompt HIV testing and attention to immune restoration. Recognising the umbilicated papule, distinguishing it from warts and other papules, and tailoring management to the context is therefore a high-yield, everyday competency that also opens a window onto a patient's immune status.
RECALL
Recall from the viral foundations SDL and from Microbiology that molluscum contagiosum virus is a poxvirus — distinct from the herpesviruses and from HPV — and that, unusually, poxviruses replicate entirely in the cytoplasm of the host cell, carrying their own replication enzymes. Recall that this cytoplasmic replication produces the large eosinophilic cytoplasmic inclusion bodies called Henderson-Paterson (molluscum) bodies, in contrast to the intranuclear inclusions of herpesviruses and the koilocytes of HPV. Recall too that MCV does not establish ganglion latency and spreads by direct skin contact, fomites, sexual contact and autoinoculation, and that, because it is not a vesicular herpesvirus, a Tzanck smear is not the relevant test. Keep these mechanisms in mind — they explain both the morphology and the contagious behaviour you will recognise.
Recognising Molluscum Contagiosum: The Umbilicated Papule
Molluscum Contagiosum: Umbilicated Papule and Clinical Contexts
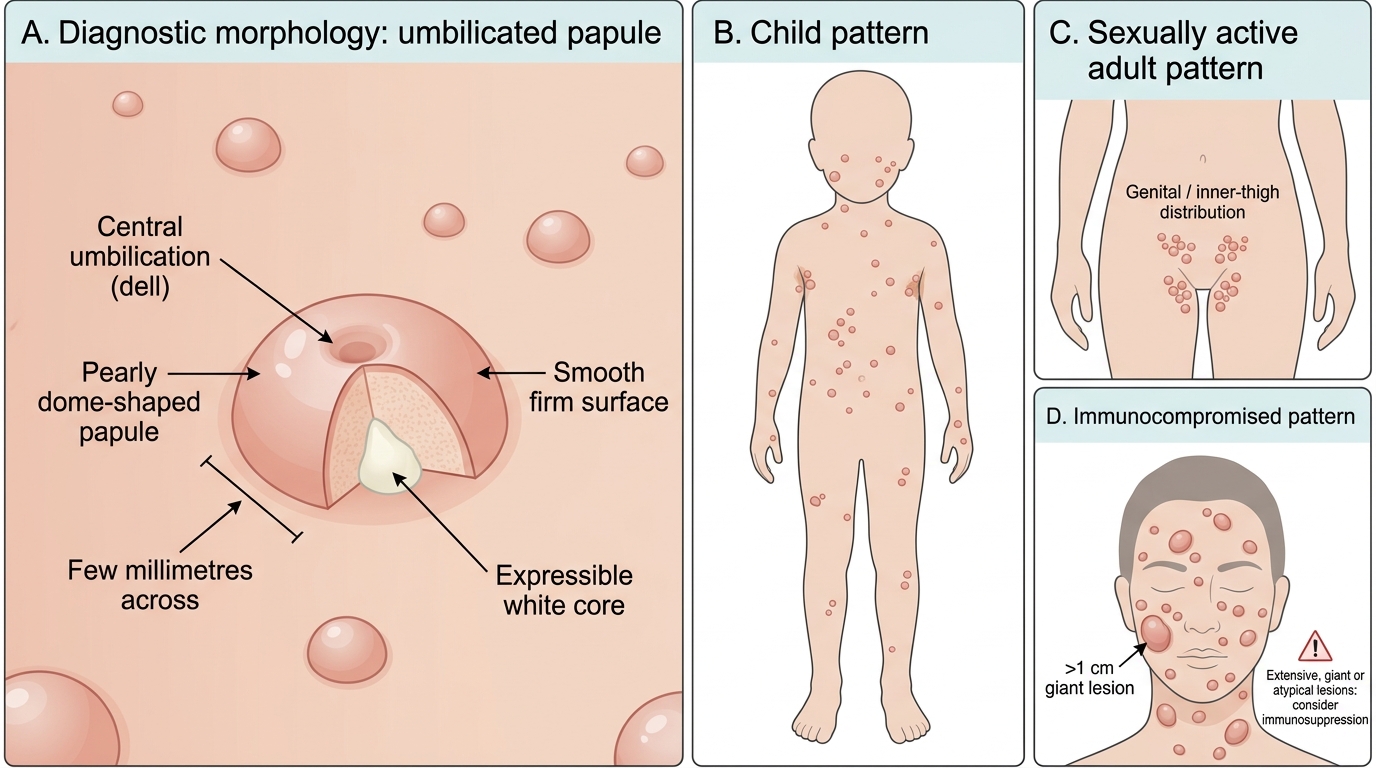
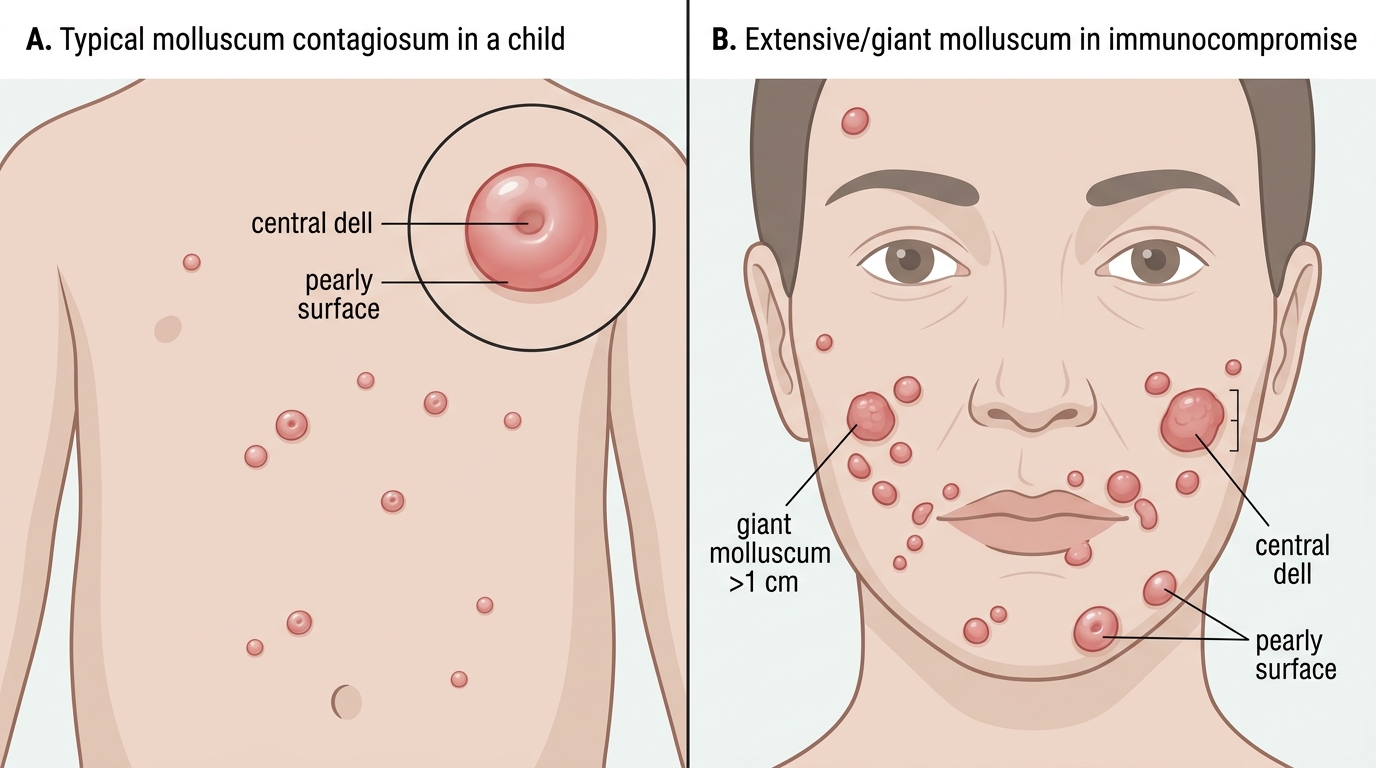
The defining recognition feature of molluscum contagiosum is the central umbilication — a small dimple or dell in the middle of a pearly, dome-shaped, flesh-coloured papule — and once you have trained your eye to look for this central dimple, the diagnosis is usually made at a glance. The papules are typically firm, smooth-surfaced and a few millimetres across, often occurring in crops, and they may contain a cheesy white core that can be expressed. The same morphology appears across three very different clinical contexts, and recognising the lesion is only half the task: reading the context tells you what the lesion means. In children the papules scatter over the trunk, axillae, face and limbs; in sexually active adults they cluster on the lower abdomen, genitalia and inner thighs; and in the immunocompromised they may be extensive, giant (greater than 1 cm), atypical and concentrated on the face.
The features that make molluscum recognisable are:
- Pearly, dome-shaped, flesh-coloured papules with a central umbilication (dell) — the diagnostic anchor.
- Firm, smooth, a few millimetres across, often in crops, sometimes with an expressible white core.
- Three contexts: scattered on trunk/face/limbs in children; genital/inner-thigh in sexually active adults; extensive/giant/atypical and facial in the immunocompromised.
- Extensive, giant or atypical lesions should raise concern for underlying immunosuppression (e.g. HIV).
Clinical Forms of Molluscum Contagiosum
MCV Pathogenesis and Histological Hallmark
Molluscum Contagiosum: Cytoplasmic Replication and Henderson-Paterson Bodies
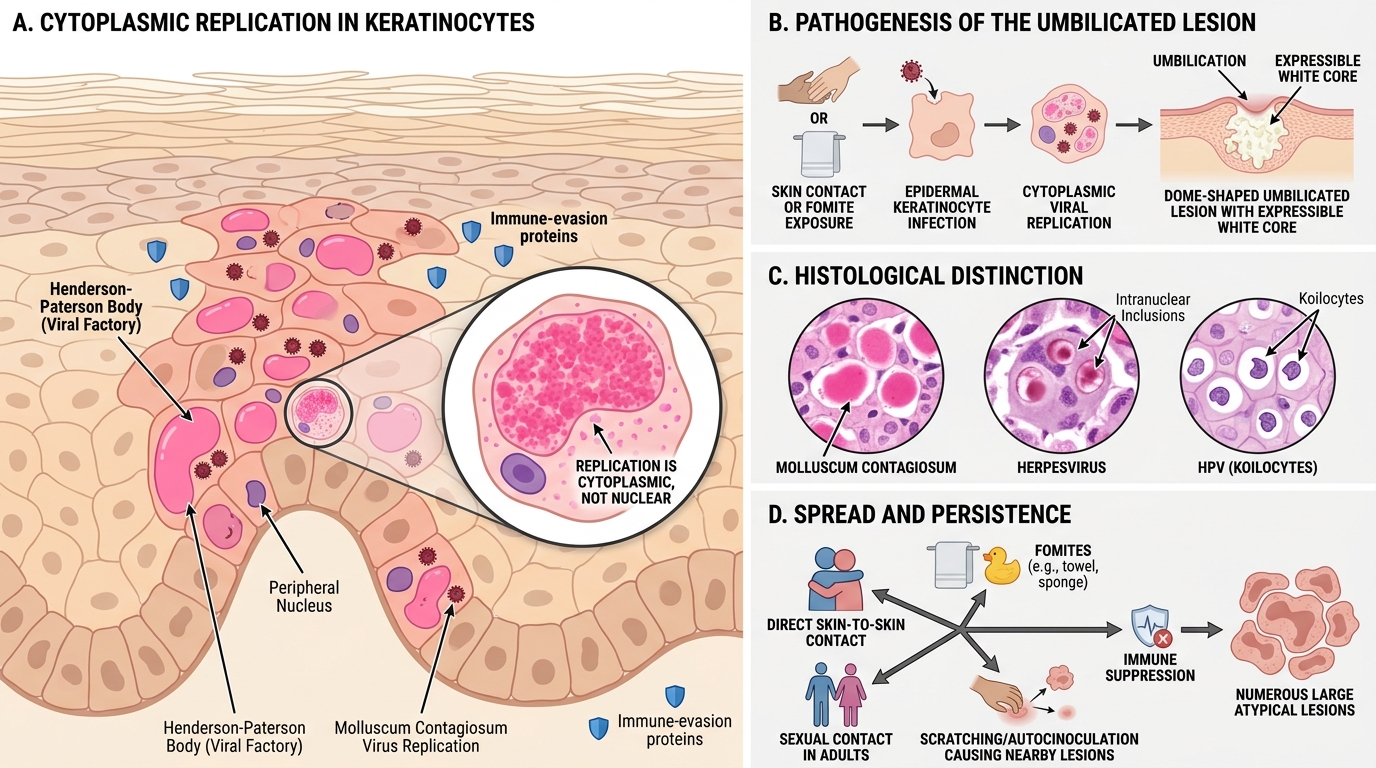
The appearance, the persistence and the contagiousness of molluscum all follow from the fact that its cause is a poxvirus replicating in the keratinocyte cytoplasm. Molluscum contagiosum virus infects epidermal keratinocytes and, because poxviruses carry their own enzymes, completes its entire replication cycle in the cytoplasm rather than the nucleus. This produces the histological hallmark — large eosinophilic cytoplasmic inclusion bodies called Henderson-Paterson (molluscum) bodies — which fill the infected keratinocytes and account for the white core that can be expressed from a lesion. Crucially, the virus encodes proteins that locally dampen the host immune response, which is why individual lesions can persist for months and why, when immunity is poor, lesions become numerous, large and atypical. Unlike the herpesviruses, MCV establishes no latency in nerve ganglia; instead it spreads by direct skin-to-skin contact, by fomites (towels, sponges), by sexual contact in adults, and by autoinoculation (scratching), seeding new lesions nearby.
The pathogenetic points that explain recognition are:
- MCV is a poxvirus replicating entirely in the keratinocyte cytoplasm (carries its own enzymes).
- Histological hallmark: Henderson-Paterson (molluscum) bodies — large eosinophilic cytoplasmic inclusions — distinct from herpesvirus intranuclear inclusions and HPV koilocytes.
- Virus-encoded immune-evasion proteins allow lesions to persist and to become extensive when immunity is poor.
- No ganglion latency; spread by contact, fomites, sexual contact and autoinoculation.
SELF-CHECK
What is the histological hallmark of molluscum contagiosum, and where in the cell is it found?
A. Multinucleate giant cells, found in the nucleus
B. Henderson-Paterson (molluscum) bodies — large eosinophilic inclusions found in the cytoplasm of infected keratinocytes
C. Koilocytes with perinuclear haloes, found at the epidermal surface
D. Intranuclear inclusion bodies typical of herpesviruses
Reveal Answer
Answer: B. Henderson-Paterson (molluscum) bodies — large eosinophilic inclusions found in the cytoplasm of infected keratinocytes
Molluscum contagiosum is caused by a poxvirus that replicates in the cytoplasm, producing large eosinophilic cytoplasmic inclusion bodies called Henderson-Paterson (or molluscum) bodies — the histological hallmark, and the basis of the expressible white core. Multinucleate giant cells are the Tzanck-smear hallmark of herpesvirus infection; koilocytes (perinuclear haloes) are the hallmark of HPV (warts); and intranuclear inclusions are characteristic of herpesviruses, not poxviruses. Recognising that the inclusion is cytoplasmic reflects the poxvirus biology that distinguishes molluscum from the other cutaneous viral infections.
Clinical Features Across the Three Contexts
Molluscum Contagiosum — Clinical Features Across the Three Contexts
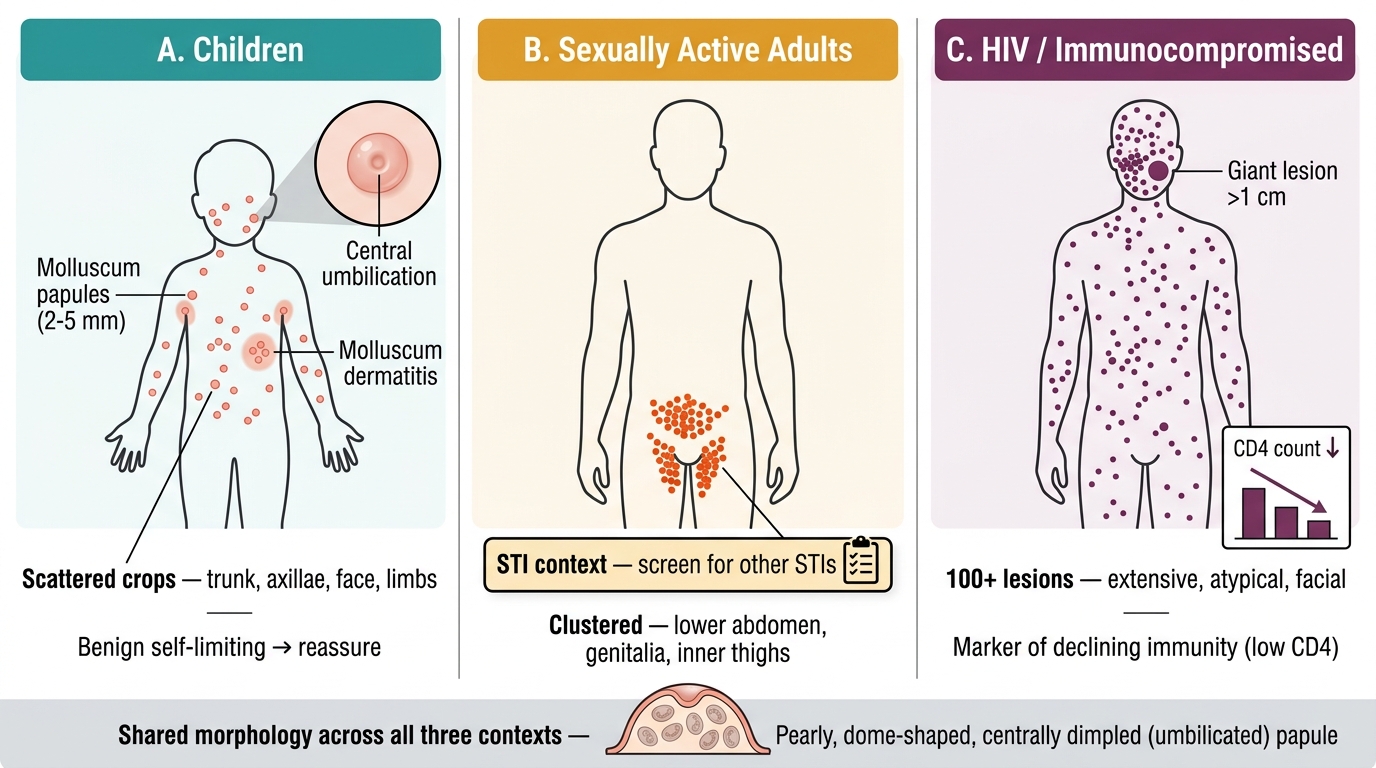
Reading molluscum well means recognising not just the umbilicated papule but the clinical context in which it appears, because the same lesion carries a different meaning and a different management implication in each of the three groups. The morphology — pearly, dome-shaped, centrally dimpled papules — is shared, but the distribution, the number, the size and the significance differ markedly between the healthy child, the sexually active adult, and the immunocompromised patient. Recognising the context is therefore as much a part of the diagnosis as recognising the lesion, and it is what determines whether you reassure, screen for sexually transmitted infections, or investigate for immunosuppression. A common associated finding is molluscum dermatitis, an eczematous reaction in the skin around the lesions.
The three contexts and their features are:
- Children: scattered crops of 2–5 mm papules on the trunk, axillae, face and limbs; benign and usually self-limiting; the main task is reassurance and avoiding overtreatment.
- Sexually active adults: lesions clustered on the lower abdomen, genitalia and inner thighs — a sexually transmitted infection warranting counselling and screening for other STIs.
- HIV / immunocompromised: extensive (sometimes more than 100 lesions), giant (greater than 1 cm), atypical, and often facial; a marker of declining immunity (low CD4) that should prompt HIV testing.
- Molluscum dermatitis: an eczematous halo around lesions, sometimes the reason a patient presents.