Page 16 of 22
DR8.5 | Molluscum Contagiosum Recognition — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Molluscum Contagiosum: Differential Diagnosis and Investigations
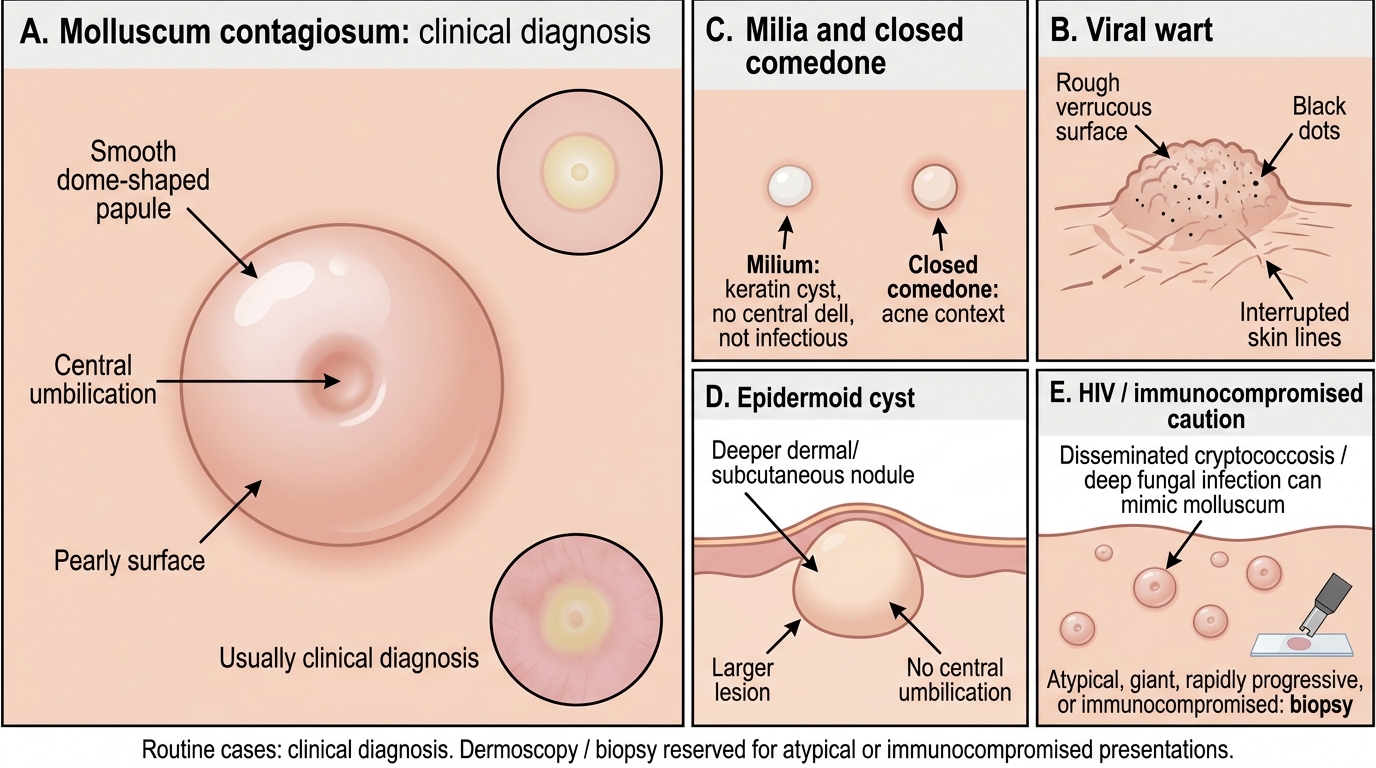
Molluscum is usually a confident clinical diagnosis, and the differential is settled by reading the surface of the papule and, where present, its central dimple. The most important everyday distinction is from a viral wart: molluscum is smooth, dome-shaped and centrally umbilicated, whereas a wart is rough, verrucous and shows black dots with interrupted skin lines — quite different surfaces. Milia are tiny white keratin cysts without a central dell and are not infectious; closed comedones occur in an acne context; and a sebaceous (epidermoid) cyst is a deeper, larger, non-umbilicated nodule. A special caution applies in HIV: disseminated cryptococcosis (and other deep fungal infections) can produce umbilicated papules that mimic molluscum closely, so in an immunocompromised patient with atypical or rapidly progressive lesions a biopsy is warranted to avoid missing a serious infection. In routine cases, clinical diagnosis suffices; dermoscopy and biopsy are reserved for atypical, giant or immunocompromised presentations.
The differential and investigation points are:
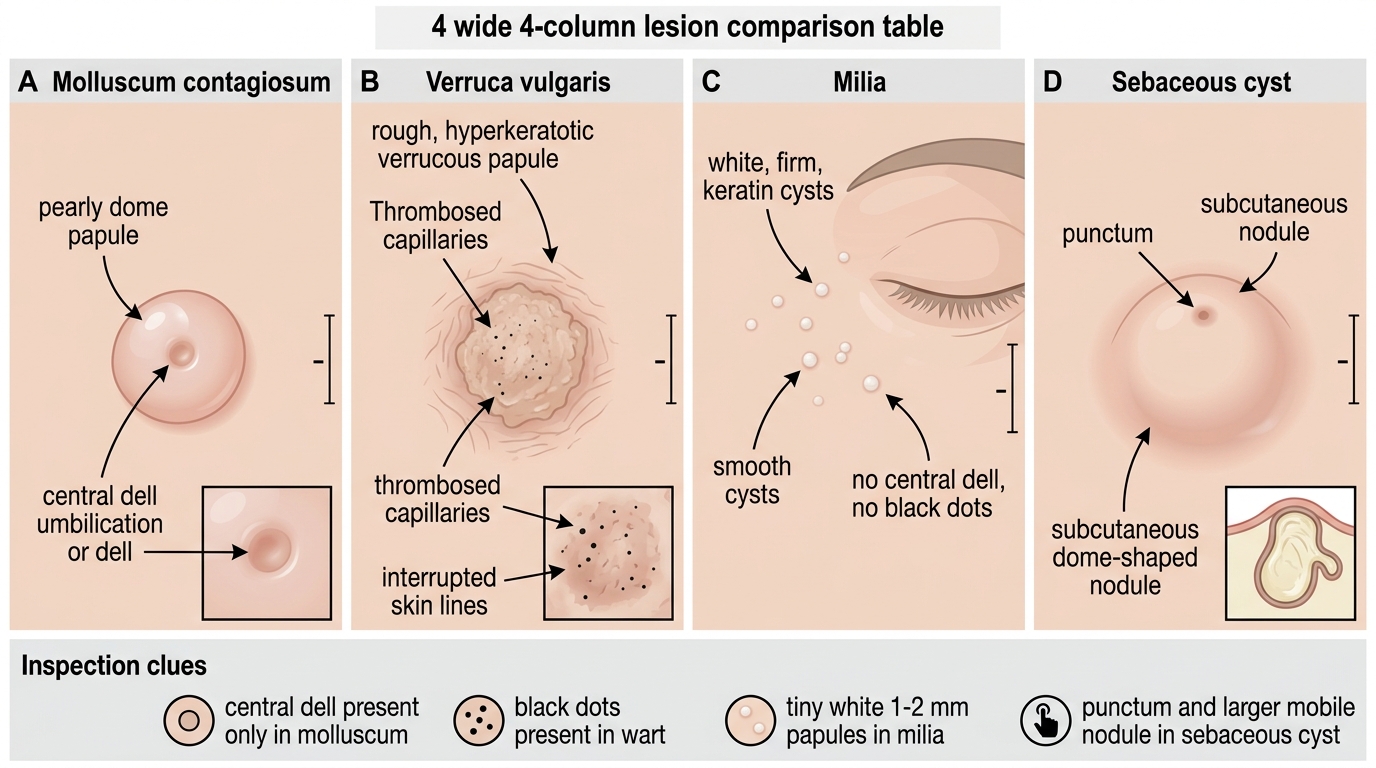
- Viral wart: rough, verrucous, black dots, interrupted skin lines (vs smooth, umbilicated molluscum).
- Milia: tiny white keratin cysts, no central dell, not infectious; closed comedones: acne context.
- Sebaceous (epidermoid) cyst: deeper, larger, non-umbilicated nodule.
- In HIV — cryptococcosis / deep fungal infection: can mimic molluscum; biopsy atypical or progressive lesions to exclude it.
- Investigations: clinical diagnosis usually sufficient; dermoscopy (central pore, polylobular white-yellow structures, crown vessels) and biopsy (Henderson-Paterson bodies) for atypical/giant/HIV cases.
Inspection Clues: Molluscum vs Wart vs Milia vs Sebaceous Cyst
SELF-CHECK
Which single feature best distinguishes molluscum contagiosum from a common viral wart on inspection?
A. Molluscum is rough and verrucous with black dots; warts are smooth and umbilicated
B. Molluscum is a smooth, dome-shaped papule with central umbilication; warts are rough, verrucous and show black dots with interrupted skin lines
C. Molluscum shows multinucleate giant cells on Tzanck smear; warts do not
D. Molluscum is always dermatomal; warts are scattered
Reveal Answer
Answer: B. Molluscum is a smooth, dome-shaped papule with central umbilication; warts are rough, verrucous and show black dots with interrupted skin lines
Molluscum contagiosum presents as a smooth, pearly, dome-shaped papule with a central umbilication (dell), whereas a viral wart is rough and verrucous, with black dots (thrombosed capillaries) and interrupted skin lines. The surface and the central dell are the decisive discriminators on inspection. Neither molluscum nor warts shows multinucleate giant cells (that is a herpesvirus finding on Tzanck smear), and molluscum is not dermatomal — a dermatomal pattern describes herpes zoster. Reading the smooth umbilicated surface versus the rough black-dotted surface is the key bedside distinction.
Management of Molluscum Contagiosum
Management of Molluscum Contagiosum
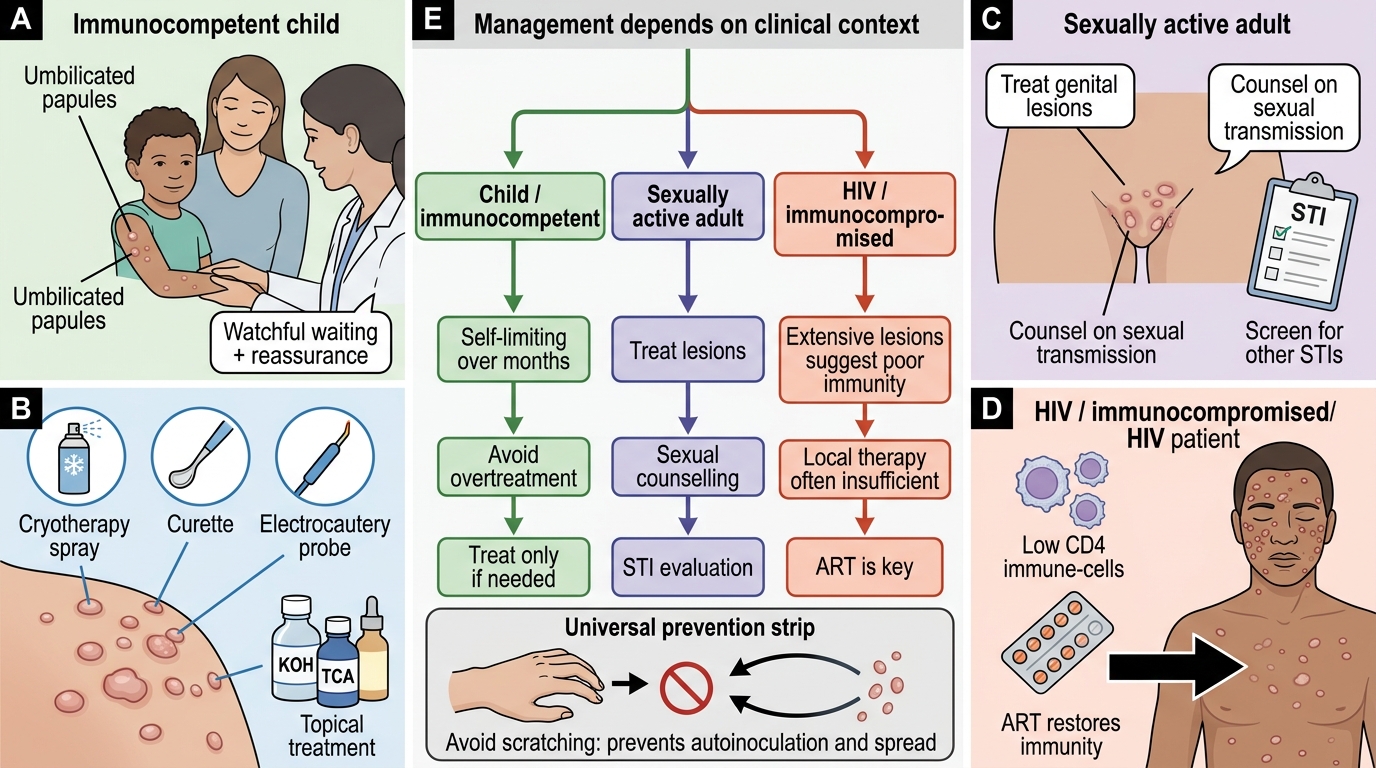
Management of molluscum is guided by the clinical context, because the right action differs sharply between a healthy child, an adult with a sexually transmitted infection, and an immunocompromised patient. In immunocompetent people — especially children — molluscum is self-limiting, often clearing over months, so watchful waiting with reassurance is a legitimate and often preferred option that avoids painful procedures in young children. When treatment is wanted, it is largely physical or topical: physical destruction (cryotherapy, curettage, electrocautery) or topical agents that provoke resolution. In sexually active adults, treating genital lesions and counselling on sexual transmission and other STIs is appropriate. The most important context-specific principle is in HIV/immunocompromise: extensive molluscum reflects poor immunity, topical and physical treatments alone are often ineffective, and restoring immunity with antiretroviral therapy (ART) is the key intervention that brings the lesions under control. Throughout, counsel patients to avoid scratching, since autoinoculation spreads the infection.
The management principles are:
- Children/immunocompetent: often self-limiting — watchful waiting and reassurance are appropriate; avoid overtreatment.
- Physical destruction: cryotherapy, curettage, electrocautery; topical options include trichloroacetic acid, imiquimod, and potassium hydroxide (KOH) solution.
- Sexually active adults: treat genital lesions; counsel on sexual transmission and screen for other STIs.
- HIV / immunocompromised: antiretroviral therapy (ART) to restore immunity is the key intervention; topical/physical treatments are less effective without immune recovery.
- Counsel: avoid scratching (prevents autoinoculation), avoid sharing towels/sponges; the condition is contagious by contact.
Self-Assessment: Molluscum Contagiosum Recognition
Molluscum Contagiosum: Morphological Recognition, Clinical Contexts, and Management Pathway
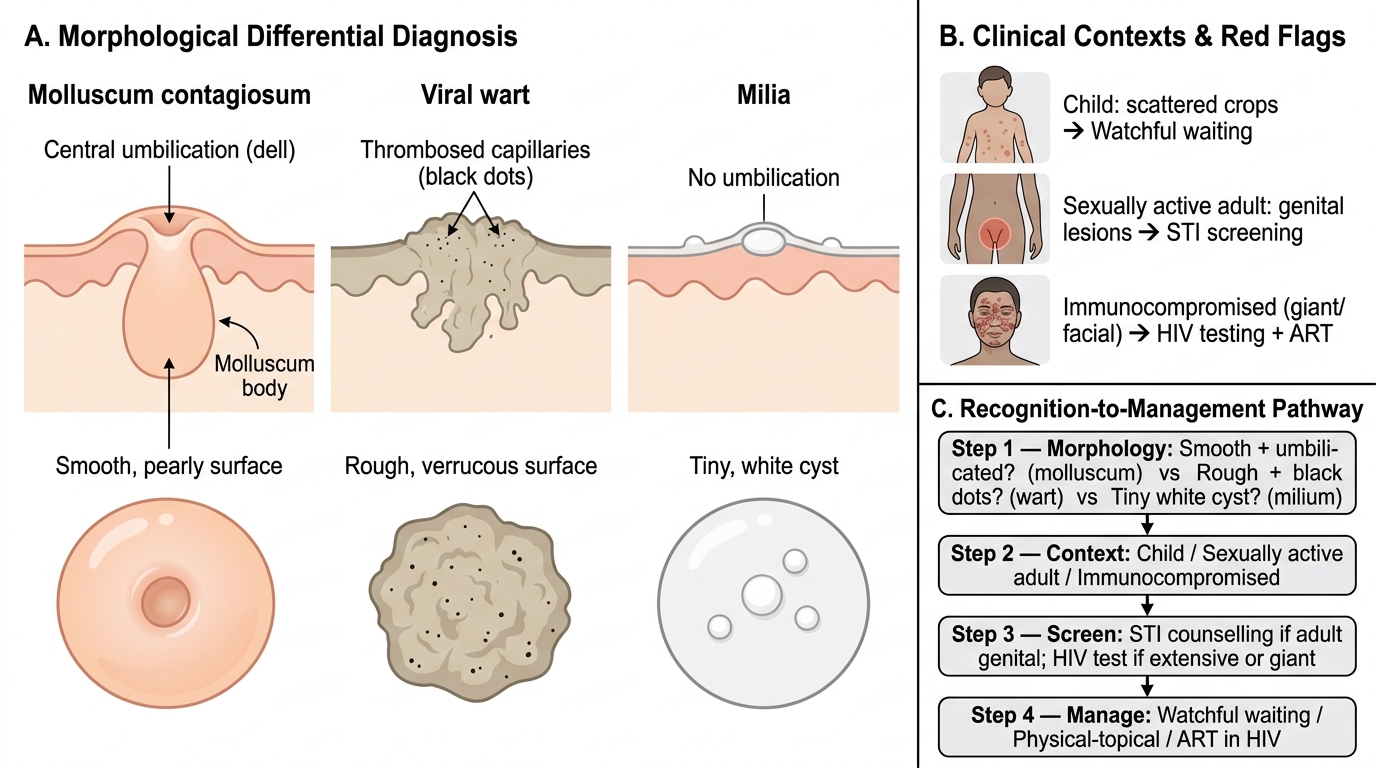
The aim of this closing section is to confirm that you can recognise molluscum contagiosum by its umbilicated papule, read its clinical context, and separate it from warts and milia before choosing management. Recognition is an ordered reading: identify the pearly, dome-shaped papule with a central dell; place it in context (a healthy child, a sexually active adult, or an immunocompromised patient); run the key differentials (smooth umbilicated molluscum versus rough black-dotted wart, versus tiny non-umbilicated milia); and only then decide between watchful waiting, physical/topical treatment, STI counselling, or — in HIV — immune restoration with ART. The scenarios you should be able to handle include the scattered crops of a child's molluscum, the genital lesions of an adult needing STI screening, and the extensive giant facial molluscum that should trigger HIV testing. Use the self-check below to rehearse moving from lesion to context to management.
For each scenario, ask in order:
- Is the papule smooth, dome-shaped and centrally umbilicated (molluscum) rather than rough and black-dotted (wart) or a tiny white cyst (milium)?
- In which context does it appear — child, sexually active adult, or immunocompromised patient?
- Does the context demand STI screening, or does an extensive/giant/atypical pattern demand HIV testing?
- Is watchful waiting appropriate, is physical/topical treatment indicated, or is immune restoration (ART) the key intervention?
SELF-CHECK
An HIV-positive patient presents with more than 100 papules over the face, several larger than 1 cm, each with a central umbilication. What is the diagnosis and the key management principle?
A. Viral warts; treat all lesions with salicylic acid
B. Molluscum contagiosum; the extensive/giant atypical pattern reflects immunosuppression, and restoring immunity with antiretroviral therapy (ART) is the key intervention
C. Herpes zoster; start aciclovir within 72 hours
D. Milia; reassure, no treatment needed
Reveal Answer
Answer: B. Molluscum contagiosum; the extensive/giant atypical pattern reflects immunosuppression, and restoring immunity with antiretroviral therapy (ART) is the key intervention
Pearly, centrally umbilicated papules are molluscum contagiosum; when they are extensive, giant (greater than 1 cm), atypical and facial, this pattern reflects significant immunosuppression and should prompt HIV evaluation. In an HIV patient, the key management principle is immune restoration with antiretroviral therapy (ART), because topical and physical treatments alone are often ineffective while immunity remains poor — control of the lesions follows immune recovery. Warts are rough and black-dotted (not umbilicated), herpes zoster is a dermatomal vesicular eruption, and milia are tiny non-umbilicated keratin cysts; none fits this picture. Note that disseminated cryptococcosis can mimic molluscum in HIV, so atypical or progressive lesions warrant biopsy.
CLINICAL PEARL
The central umbilication (a dimple in a pearly, dome-shaped papule) is the diagnostic fingerprint of molluscum contagiosum — and the clinical context tells you what it means. In a healthy child it is a trivial, self-limiting infection best managed by reassurance; in a sexually active adult, genital molluscum is a sexually transmitted infection that warrants STI screening; and extensive, giant or atypical molluscum, especially on the face, is a red flag for immunosuppression that should prompt HIV testing. In HIV, do not rely on cryotherapy or topical agents alone — restoring immunity with antiretroviral therapy is the intervention that controls the disease. Remember that disseminated cryptococcosis can mimic molluscum in HIV, so biopsy atypical or progressive lesions.