Page 12 of 18
FM2.{23,27-28} | Crime Scene Investigation & Mass Disaster Response — SDL Guide (Part 2)
Mass Disaster Response: INTERPOL DVI and Local Resources
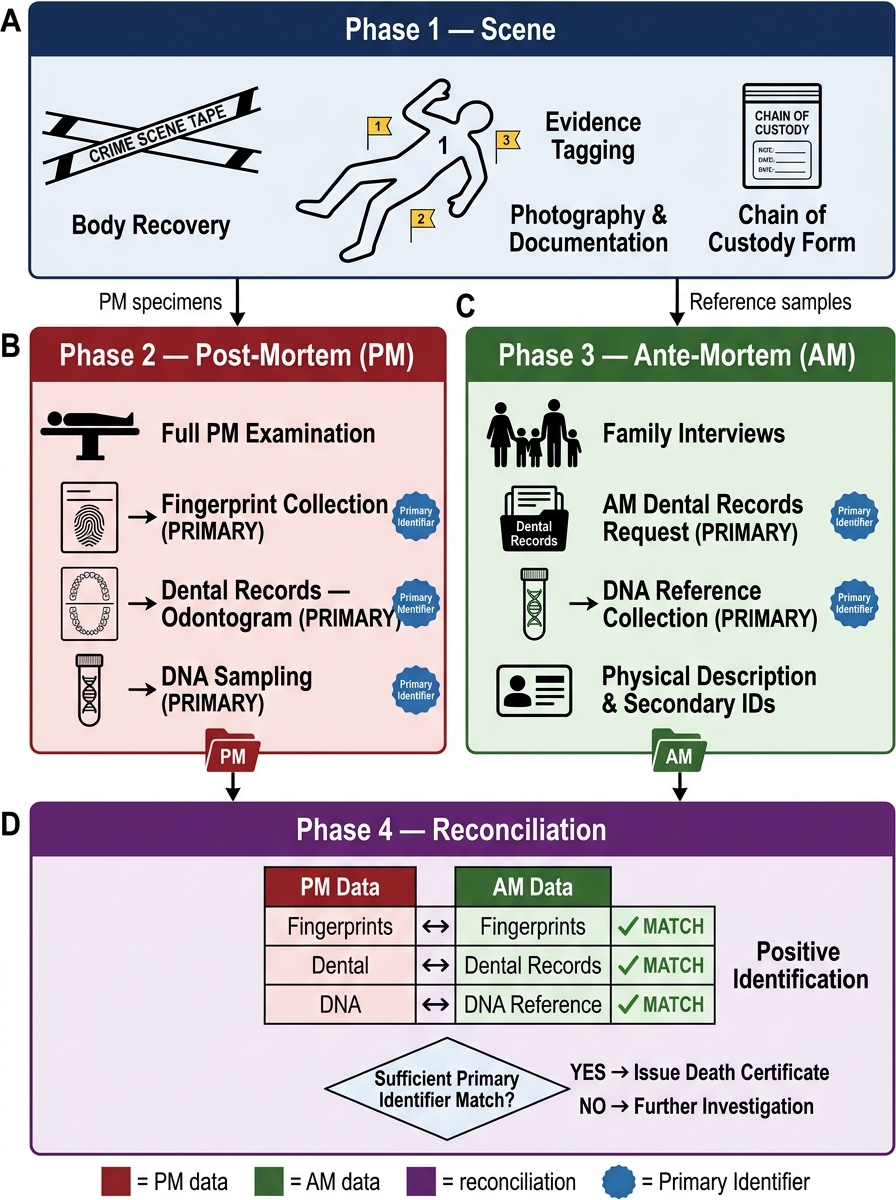
Mass disaster situations — defined as events resulting in multiple fatalities that exceed the routine capacity of local mortuary and investigative services — require a structured, international standard-compliant approach to victim identification. The recognised framework is the INTERPOL Disaster Victim Identification (DVI) protocol, which divides the entire response into four sequential phases:
Phase 1: Scene — recovery and documentation of remains and associated evidence. Bodies and body fragments are tagged, numbered, and mapped to their location in the scene. The position, condition, and associated personal effects (clothing, jewellery, documents) are photographed and documented before any remains are moved. Human remains search teams systematically cover the scene.
Phase 2: Post-mortem — examination of recovered remains to generate identifying information. This is the forensic physician's primary operational domain. Each set of remains (even fragments) is examined for: fingerprints, dental findings (charting on standardised forms), DNA samples (blood, bone, teeth, hair roots), anthropological assessment (sex, age, stature), and distinctive marks (tattoos, surgical scars, implants). Findings are recorded on standardised INTERPOL DVI forms (pink forms — post-mortem data).
Phase 3: Ante-mortem — parallel collection of identifying information from family members and pre-disaster sources. Family interviews document physical descriptions, dental history, medical history, fingerprint records (passport, national ID), and DNA reference samples (from family members or personal effects). Dental records from treating dentists, medical implant records, and previous DNA profiles from forensic databases are collected. Findings are recorded on yellow INTERPOL DVI forms (ante-mortem data).
Phase 4: Reconciliation — systematic comparison of post-mortem and ante-mortem data to establish identity. The reconciliation team matches PM data to AM data using: primary identifiers (fingerprints, DNA, dental — considered definitive) and secondary identifiers (physical description, clothing, jewellery — supportive but not individually conclusive). Each identification is reviewed and approved before the family is notified.
Using local resources (FM2.28): India's mass disaster response frequently operates in resource-limited settings where INTERPOL-standard equipment may not be immediately available. The forensic physician must be adept at using local resources: improvised body bags from plastic sheeting; local dental practitioners for ante-mortem record retrieval; local forensic laboratories for DNA analysis; regional blood banks for large-scale DNA reference sampling; local community leaders and language interpreters for family communication in multi-lingual disasters; and publicly available ante-mortem data (voter ID photos, Aadhaar biometrics) as supplementary identification tools.
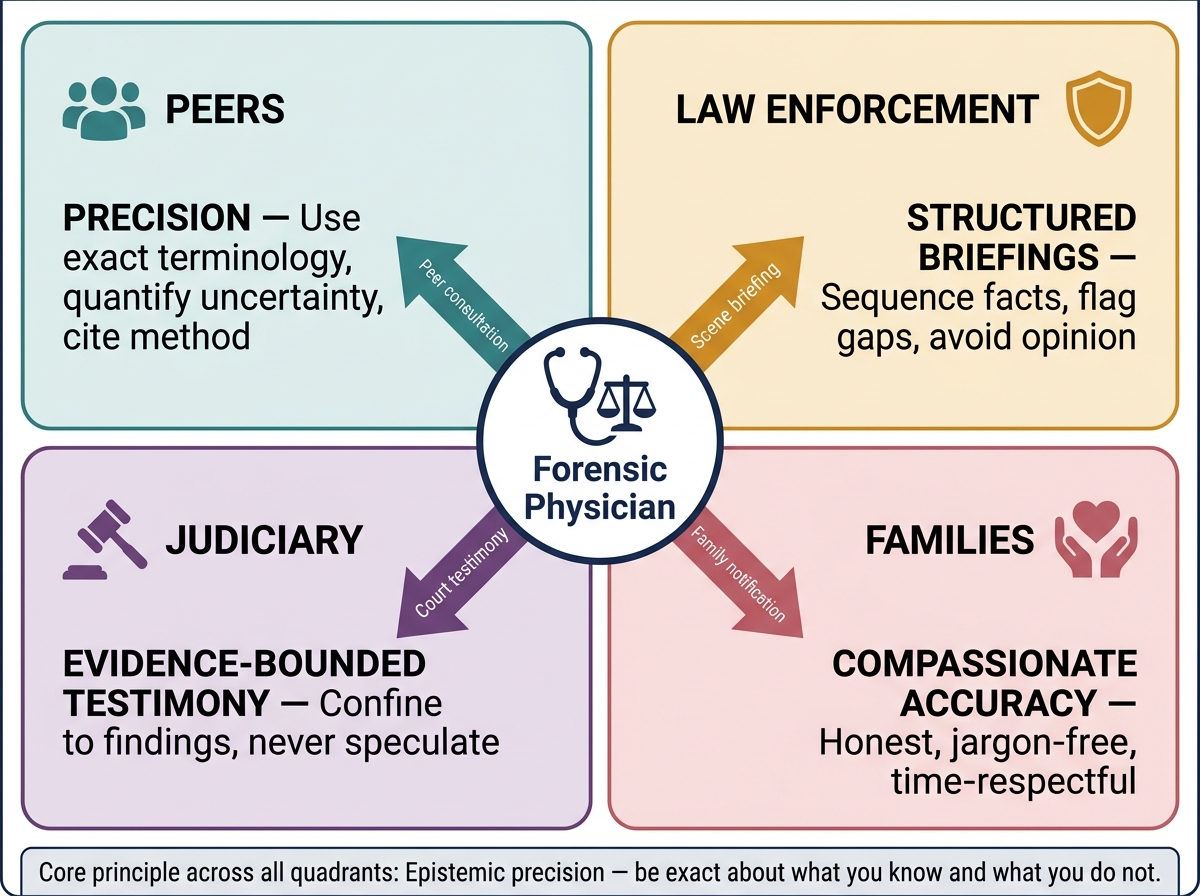
Communication with stakeholders (FM2.27): mass disaster communication demands are intense and multi-directional. The forensic physician must communicate: with peers (forensic team members, pathologists, anthropologists) using precise technical language to prevent identification errors; with law enforcement using structured briefings that distinguish confirmed from provisional findings; with the judiciary (if a magistrate inquest is convened) using evidence-grounded testimony; and with families using compassionate, culturally sensitive language that is simultaneously accurate about what is and is not yet known. FM2.27 emphasises both verbal and non-verbal communication — in a disaster family waiting area, the physician's body language, eye contact, and tone convey as much as the words, particularly across language barriers or in states of severe grief.
INTERPOL DVI Protocol: Four-Phase Disaster Victim Identification Framework
SELF-CHECK
In the INTERPOL DVI protocol, DNA matching and dental comparison are considered 'primary identifiers' because they:
A. Are the fastest methods available in disaster settings
B. Are individually sufficient to establish identity without requiring corroboration
C. Are legally required by all jurisdictions
D. Are the cheapest methods available in resource-limited settings
Reveal Answer
Answer: B. Are individually sufficient to establish identity without requiring corroboration
Primary identifiers (fingerprints, DNA, dental) are those that are individually sufficient to establish a positive identification — a single primary identifier match, properly verified, is enough to identify a victim without requiring corroboration by other methods. Secondary identifiers (physical description, clothing, jewellery) support but cannot individually confirm identification. This distinction is important because it prevents misidentification errors in mass casualty settings.
Medicolegal Inference and Communication Framework
The statutory framework for crime scene visits and disaster victim identification intersects multiple domains of law: criminal law (the inquest provisions of the CRPC), disaster management law (the Disaster Management Act 2005, which establishes the National Disaster Management Authority and state disaster management frameworks), and identity documentation law (deaths in mass disasters must be formally certified under state rules).
For crime scenes: the doctor attends on police/magistrate request under the inquest framework. The scene visit report is a medicolegal document submitted to the investigating officer and may be produced in court. The physician may be called as a witness to describe scene findings and their interpretation — and must confine testimony to what was observed at the scene and its preliminary significance, not to autopsy conclusions not yet made.
For mass disasters: the Disaster Management Act 2005 provides the overarching framework, with state and district authorities coordinating response. The forensic physician operates within the Incident Command Structure, typically as part of the medical sub-component or specifically as the DVI coordinator if so designated. Identifications made through the DVI process are submitted to the appropriate magistrate for formal death certification — without formal certification, families cannot access insurance, provident funds, or other legal benefits.
Communication standards (FM2.27) operationalised:
- With peers: use INTERPOL-standard terminology; record all communications in writing; never communicate a 'probable identification' verbally without written documentation
- With law enforcement: distinguish 'confirmed findings' from 'preliminary impressions'; provide structured written briefings rather than informal oral updates
- With the judiciary: all testimony is under oath; confine statements to findings within your direct expertise; state uncertainty explicitly ('I cannot determine the exact cause of death from the available remains at this time')
- With families: use the family liaison framework; never give identification information at the scene informally; formal notifications should occur in a private, culturally appropriate setting with interpreter support if needed; acknowledge uncertainty honestly without causing unnecessary distress
The principle underlying all of FM2.27 is that the forensic physician is a communication bridge between medical science and the legal, investigative, and social systems that depend on that science for justice. The quality of that bridge — its accuracy, clarity, and compassion — determines whether the scientific work translates into useful outcomes for families and the justice system.
FM2.27 Forensic Physician Communication Framework: Audience-Adapted Epistemic Standards
CLINICAL PEARL
Pearl: At the crime scene, say 'consistent with' — not 'is.' 'The body has injuries consistent with blunt force trauma to the head' is the correct preliminary statement; 'the body shows blunt force head injuries' closes interpretive options before the autopsy. 'Death occurred approximately 12–24 hours ago based on the post-mortem changes observed' is correct; 'death was yesterday evening' is not. Crime scene statements are preliminary — they are made before the full examination, without laboratory results, and in conditions that are suboptimal for examination. They become part of the investigation record, are sometimes leaked to the media, and will be quoted back to you in court. Epistemic precision — being exact about what you know and what you don't — is a professional standard, not timidity.
SELF-CHECK
In a mass disaster response, a family member insists on being told immediately whether the body of their relative has been found among the recovered remains. The forensic physician's MOST APPROPRIATE response is:
A. Show the family the body immediately to confirm identification
B. Explain that formal identification through the DVI process is required before notification, to prevent misidentification
C. Refer the family to the police officer without any explanation
D. Allow the family to search through the recovered remains themselves
Reveal Answer
Answer: B. Explain that formal identification through the DVI process is required before notification, to prevent misidentification
Informal identification at the scene without systematic DVI verification risks misidentification — a family incorrectly notified that their relative is dead, or (worse) incorrectly notified that their relative has been identified among the living, when it is someone else's remains. The DVI process exists to prevent these errors. The forensic physician should acknowledge the family's distress, explain the DVI process and its purpose, and commit to timely notification once formal identification is confirmed.