Page 11 of 18
FM2.{23,27-28} | Crime Scene Investigation & Mass Disaster Response — SDL Guide
Learning Objectives
- Describe the objectives of a crime scene visit and the doctor's duties, and how to reconstruct the sequence of events (FM2.23)
- Demonstrate ability to exchange information verbally and non-verbally with peers, family, law enforcement, and the judiciary (FM2.27)
- Demonstrate ability to use local resources in mass disaster situations (FM2.28)
INSTRUCTIONS
Modern forensic medicine requires the physician to operate effectively not only in the autopsy room but also at the scene of death, in multi-agency disaster response settings, and across all the communication interfaces that connect medicine to law. This module covers the forensic physician's role at the crime scene — as a scientific advisor, not a detective — and the structured framework of Disaster Victim Identification (DVI) that turns the chaos of a mass casualty event into an organised, legally sound process. It also addresses the communication competencies that make the forensic physician effective as an expert witness, family liaison, and interdisciplinary team member.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed., Ch. 5, 6 (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed., Ch. 6, 9 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A train derailment at 3 AM leaves 47 dead and 120 injured across a 200-metre stretch of track. Bodies are dismembered, incomplete, and scattered. Families arrive from multiple states. A police officer calls you — the forensic medicine faculty member at the nearest government medical college — and asks: 'We need a doctor at the scene. What do you do when you get here?' Simultaneously, a second call: 'The Minister wants the bodies identified and families notified within 24 hours.' You are the forensic physician for this mass disaster. Where do you start, what resources do you use, and how do you communicate with the families, the police, the railway administration, and the court?
WHY THIS MATTERS
Crime scene visits and mass disaster response are competencies that separate a broadly-trained forensic physician from one who operates only in the autopsy room. India experiences mass casualty events regularly — rail accidents, building collapses, flood and earthquake disasters, communal violence — and the forensic physician is a critical member of the response team. Understanding your role at the scene (as a medical advisor, not a police investigator) and knowing the structured DVI protocol enables you to contribute meaningfully, protect evidence integrity, and support justice even under chaotic conditions.
RECALL
For this module, review: (1) post-mortem changes and how they can be read at the scene to estimate time of death (from the au1 module); (2) the four wound types (abrasion, contusion, laceration, incised wound) — at the scene you make preliminary observations only; full wound characterisation happens at autopsy; (3) the team-based approach from the au3 module — mass disasters require the same multi-agency coordination principle, scaled up dramatically; (4) the biological profile of skeletal remains from au4 — DVI frequently involves fragmented or incomplete remains.
The Doctor at the Crime Scene: Role and Objectives
The forensic physician's attendance at a crime scene is requested by the police and authorised under the inquest framework. The fundamental principle that must be understood before any scene visit is that the doctor's role is that of a scientific advisor and medical examiner — not a primary investigator. The physician does not collect evidence, question witnesses, or direct the investigation. The physician provides medical expertise to assist the police in understanding what happened, when, and through what mechanism — information that is then incorporated into the police investigation.
The objectives of the doctor's crime scene visit (FM2.23) are:
- Confirm death — this is legally the first act; a certified determination of death by a medical officer is required before the body can be removed or any detailed scene investigation can proceed
- Estimate the post-mortem interval — using scene observations of rigor mortis, livor mortis, decomposition, and environmental conditions
- Describe external findings — a preliminary external examination, without touching or moving the body more than necessary; injuries described in general terms (their number, location, and apparent type — not their precise forensic interpretation, which awaits the autopsy)
- Assist in reconstruction of the sequence of events — based on body position, blood distribution, injury pattern, and relationship to scene features
- Advise on evidence preservation — particularly biological evidence: blood, hair, biological fluids, the body itself before it dries or is contaminated
- Provide a scene visit report — a brief written record of the above observations, submitted to the investigating officer
What the doctor does NOT do at the scene: photograph evidence as the primary photographer (that is the forensic photographer's role); collect or bag exhibits (police do this under scene-of-crime procedures); make definitive cause-of-death statements (these require the full autopsy); move the body without the investigating officer's consent; or allow any finding to be shared publicly before the inquest.
The boundary between the doctor's role and the police's role is not always intuitively understood by newer trainees. A useful framing: the doctor reads the body; the police read the scene. Both sets of readings feed the same investigation.
Scientific Basis: What Scene Evidence Tells the Forensic Physician
The forensic physician at the crime scene is primarily a reader of biological evidence — specifically, what the body and its immediate context reveal about the time, mechanism, and manner of death before the autopsy provides definitive answers.
Post-mortem changes at the scene provide PMI estimates that may be refined later. Rigor mortis state (absent, developing, fully established, or resolving) combined with ambient temperature gives a working PMI range. Livor mortis (hypostasis) distribution and fixation reveals body position at the time of death: if the lividity pattern is inconsistent with the body's position as found, the body has been moved after death (a critical scene-reconstruction finding). Lividity is fixed after approximately 8–12 hours — if the body shows dependent lividity on the back but is found face-down, someone moved it after the lividity fixed.
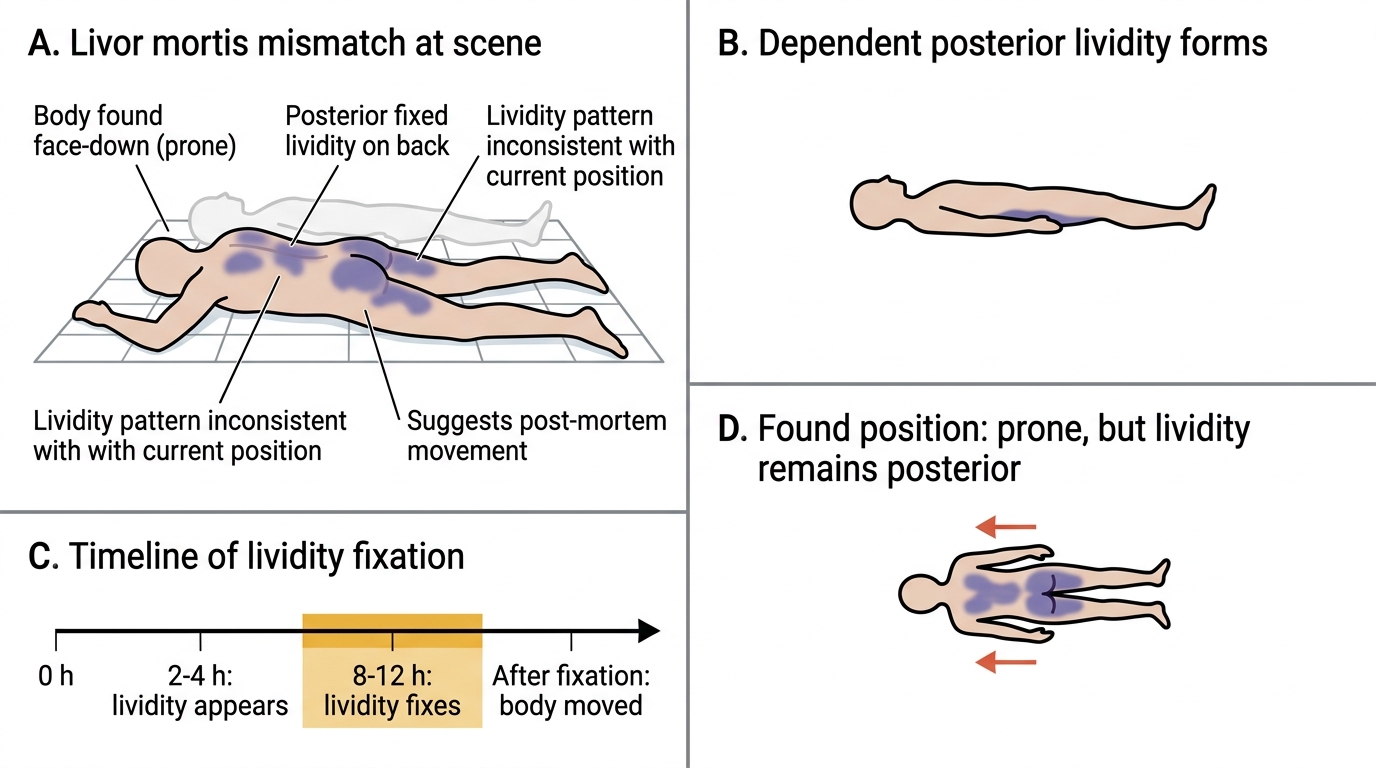
Livor Mortis Mismatch and Post-Mortem Movement
Injury pattern at scene observation — a preliminary, non-contact visual assessment — provides direction: the distribution of blood on clothing and on the scene (its area, spatter patterns if visible, direction of flow), the apparent type of injuries (blunt force pattern? sharp force pattern? firearm exit/entry pattern?), and whether injuries are consistent with the scene context (does the injury pattern fit a fall from the observed height, or does it suggest a different event?). The physician provides a preliminary assessment; the autopsy confirms.
Scene reconstruction (sequence of events) is a collaborative inference drawn from the totality of findings: body position, evidence of a struggle (overturned furniture, disrupted blood trails), post-mortem changes, visible injury pattern, and witness accounts. The forensic physician's contribution is to advise on the biological aspects — when death occurred and what the injuries preliminarily suggest about mechanism. The sequence reconstruction itself is a joint product of the police, the forensic physician, and (in complex cases) other forensic specialists (forensic scientists, entomologists, blood pattern analysts).
A critical principle: scene observations are preliminary. The physician should make careful observations and notes but must be disciplined about the language used: 'findings are consistent with a sharp force injury' rather than 'this is a knife wound'; 'post-mortem changes suggest death occurred 12–24 hours before discovery' rather than 'the person died yesterday afternoon.' Preliminary statements made at the scene may be quoted in court, and overstating certainty at the scene can compromise the autopsy opinion.
SELF-CHECK
A body is found face-down in a locked room. Livor mortis is fixed and shows hypostasis on the posterior (back) surface. This finding MOST LIKELY indicates:
A. The person was face-down at the time of death
B. The body was placed face-down after lividity had fixed on the back
C. The person died standing upright
D. Lividity distribution confirms a natural death
Reveal Answer
Answer: B. The body was placed face-down after lividity had fixed on the back
Livor mortis reflects the position of the body during the period when blood pools by gravity in dependent vessels (and before fixation at 8–12 hours). If fixed lividity is on the back (posterior surface) but the body is found face-down, the body was moved to the face-down position AFTER the lividity had fixed — indicating the body's position was altered post-mortem. This is an important scene-reconstruction finding suggesting the death scene has been tampered with.
Crime Scene Visit: Conduct and Documentation
The forensic physician's conduct at a crime scene must be methodical, restrained, and documented. Arriving at the scene and immediately touching or moving the body — even with good intentions — can destroy evidence and compromise the scene. The standard sequence of conduct is:
On arrival: report to the officer-in-charge; record the time of arrival; confirm that the scene has been cordoned and the status of other personnel. Do not enter the scene until authorised by the officer-in-charge.
Scene approach: walk-the-scene from the periphery to the body along the designated path; note the general scene (indoors/outdoors, lighting, access points, any obvious disturbance); do not touch surfaces.
Body examination sequence:
1. Confirm death (absence of vital signs — the legal act of certification)
2. Note the position of the body and its relationship to scene features; make a sketch or assist the photographer in documenting it
3. Assess post-mortem changes: rigor mortis (state), lividity (distribution, fixed or unfixed, whether consistent with position), early decomposition signs
4. Describe visible external injuries — their approximate location, size, and apparent type — without probing, opening wounds, or removing clothing (at scene)
5. Note clothing condition: intact, torn, blood-stained, displaced
6. Note any items in immediate proximity to the body that may be relevant: weapons, medications, ligature material, drug paraphernalia
Documentation: the scene visit report includes: date, time, exact location (with GPS coordinates if available), officer present, description of scene, body position and condition, post-mortem changes with PMI estimate, preliminary injury description, and specimens if any were collected at scene (blood swabs, trace evidence — in conjunction with police).
The physician's role and the police role at a crime scene are distinct but complementary:
| Doctor's duties | Police duties |
|---|---|
| Certify death | Secure and cordon scene |
| Preliminary external examination | Photograph scene systematically |
| Estimate PMI | Collect and bag physical evidence |
| Advise on biological evidence preservation | Interview witnesses |
| Note injury pattern (preliminary) | Investigate circumstances |
| Provide scene visit report | Manage chain of custody of all exhibits |
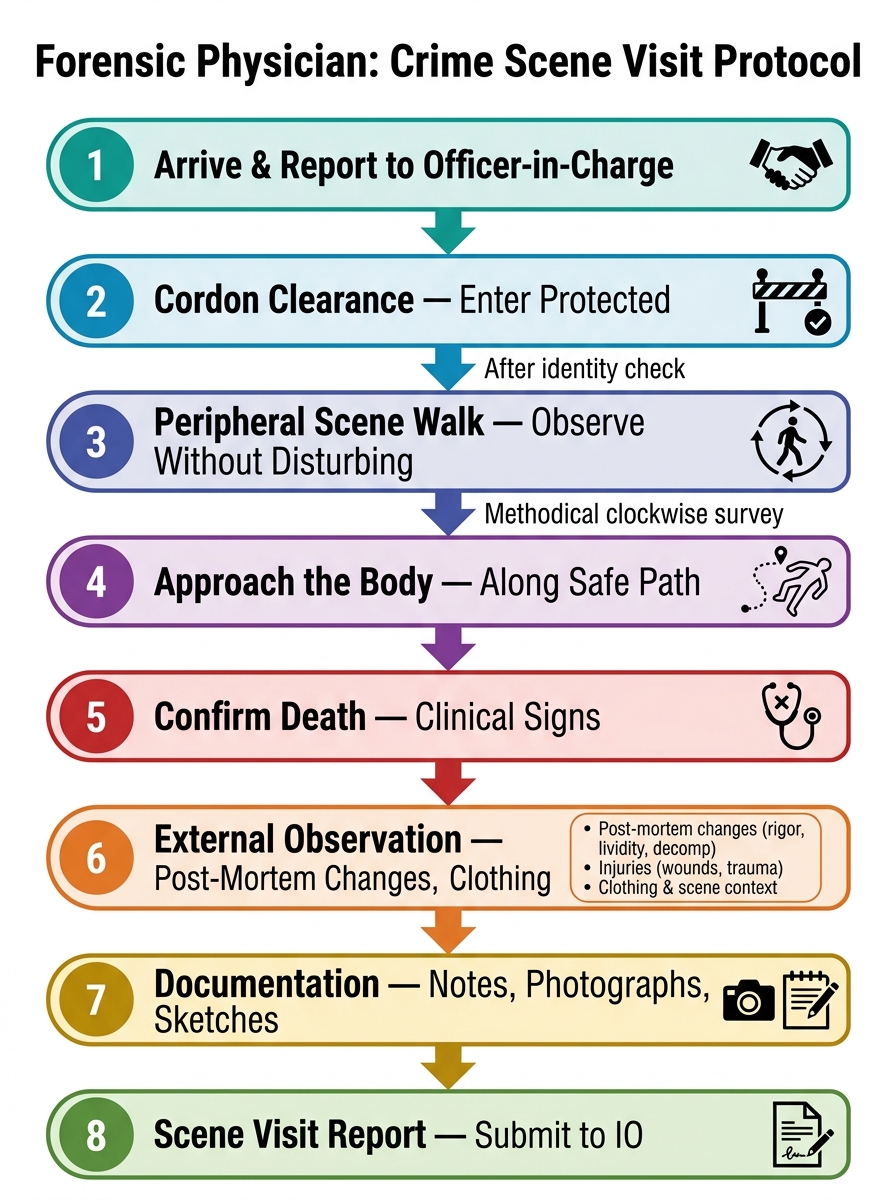
Forensic Physician's Crime Scene Visit Sequence