Page 10 of 18
FM2.21-22 | Examination of Mutilated Remains & Exhumation — SDL Guide
Learning Objectives
- Describe the examination of mutilated bodies, charred bones, and bundle of bones (FM2.21)
- Describe and discuss exhumation — legal requirements, procedure, and evidentiary value (FM2.22)
INSTRUCTIONS
Forensic medicine is frequently called upon to answer questions about death when the body itself no longer presents in a recognisable form. A body burnt beyond recognition, a bundle of bones discovered in a forest, a decomposed corpse recovered from water, or a body disinterred months after burial — all of these present the forensic physician with the challenge of extracting maximum information from severely compromised remains. These situations are encountered in disaster victim identification, cold case investigations, and routine medicolegal practice across India. The skills covered in this module are specific, procedural, and testable.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed., Ch. 5, 13 (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed., Ch. 6, 9 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Police call you to a rural scene where a burnt motorcycle is surrounded by charred remains. The investigating officer believes it was an accident, but the deceased's family insists he was murdered and the body was burnt to conceal the crime. The charred remains include a partial skull, some long bones, and fragments of soft tissue. Can you still determine: Who was this person? Was it a man or a woman? How old were they? And — crucially — were they dead before the fire started, or killed by it? The answer to each question will determine whether this is a crime scene or an accident, and whether the family's allegations have forensic merit.
WHY THIS MATTERS
The examination of mutilated and compromised remains is not a rare subspecialty skill — it is encountered in everyday Indian forensic practice, from road traffic accidents where bodies are severely injured, to domestic fires, to bodies recovered from rivers days after death, to the growing forensic challenge of disaster victim identification. Exhumation cases arise in cold cases, contested suicide determinations, and suspected custodial deaths where the original autopsy is challenged. Competence in these scenarios marks the difference between a forensic physician who can support justice even in difficult circumstances and one who is forced to report 'inconclusive' when justice demands more.
RECALL
Prepare for this module by reviewing: (1) the stages of decomposition (autolysis → putrefaction → adipocere/mummification → skeletonisation) from earlier FM modules; (2) basic skeletal anatomy — which bones are most resistant to destruction (skull, teeth, dense cortical long bones) and which are most fragile (small hands/feet bones, costal cartilages); (3) the general aims of forensic identity determination (biological profile: sex, age, stature, ancestry); (4) that exhumation requires court authority — this is the single most critical legal point and it will be tested.
The Forensic Challenge: When Standard Autopsy Is Impossible
Standard medico-legal autopsy requires a body in reasonable condition — recognisable, with organs largely intact, and post-mortem changes that are interpretable. In a subset of forensic cases, this baseline is unavailable: the remains presented for examination may be unrecognisable, fragmented, or so altered by fire, decomposition, or deliberate mutilation that the conventional examination sequence cannot be applied.
The forensic physician's task in these cases is restructured around a set of fundamental questions that must be answered, in order of priority, with whatever evidence is available:
- Is this human? (exclude non-human animal remains, especially in remote or rural scenes)
- How many individuals are represented? (scenes with multiple victims, disaster sites, or deliberate body disposal may involve more than one set of remains)
- Who is this person? — identity determination via biological profile (sex, age, stature) and unique identifiers (dentition, DNA, implants)
- What was the cause of death? — where determinable from the compromised remains
- What was the manner of death? — natural, accidental, homicidal, suicidal
- Was the body condition produced ante-mortem or post-mortem? — was the person alive when burnt, or was the body burnt after death?
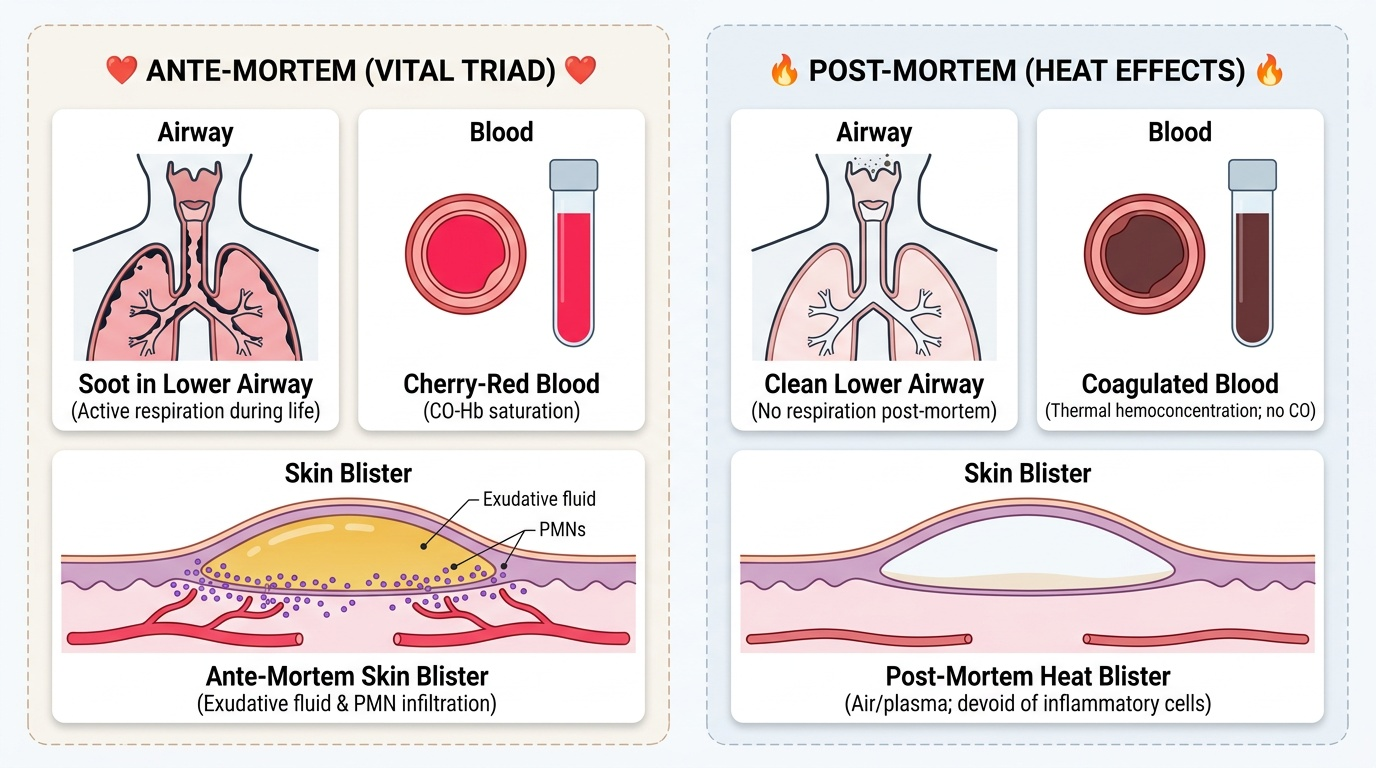
The last question is often the medicolegally critical one. A vital reaction — defined as any tissue response that occurs only in living tissue — is the key to answering it. In charred bodies, the presence of soot in the lower airway (trachea, bronchi) indicates that the person was breathing during the fire; its absence suggests the fire was post-mortem. Similarly, carbon monoxide in the blood (cherry-red or bright-red discolouration of the blood and organs) indicates ante-mortem exposure; a purely post-mortem fire produces no COHb elevation.
Understanding which vital reactions are detectable in compromised remains, and how to look for them, is the core skill of this module.
Scientific Basis: Decomposition, Charring, and Skeletal Changes
The scientific basis for examining compromised remains rests on understanding what changes occur to the body under the relevant conditions, and which forensic evidence survives those changes.
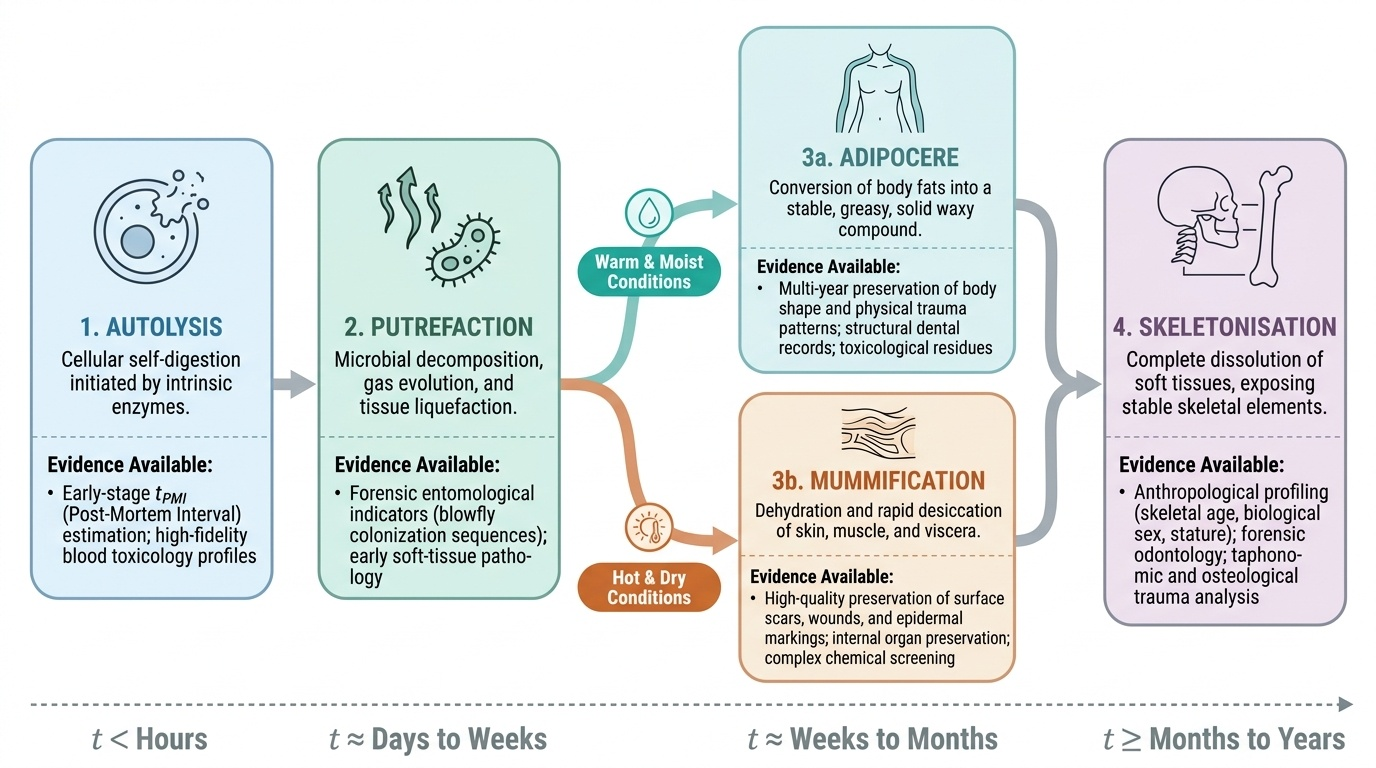
Decomposition proceeds through four stages: autolysis (cellular self-digestion, begins within hours of death), putrefaction (bacterial decomposition, producing gas, discolouration, and liquefaction), adipocere formation or mummification (preservation states under specific environmental conditions), and skeletonisation. The rate is heavily temperature-dependent: warm, moist conditions accelerate putrefaction but may produce adipocere (the saponification of body fat into a greasy, grey-white substance with a rancid soap odour, which can preserve body contours for years to decades). Hot, dry conditions promote mummification, with desiccation and preservation of skin and organs. Both adipocere and mummification, counterintuitively, preserve useful forensic evidence: wound patterns, dental structures, and sometimes even toxicological material.
Provided image
Charring changes the forensic evidence available. Soft tissue burns at approximately 300°C; bone becomes charred (black) at 400–600°C and calcined (grey-white, fragile, chalk-like) at above 700°C. Calcined bone is extremely fragile but is still useful for sex and age estimation from shape (pelvis, skull) and dental examination. Heat-induced fractures in bone must be distinguished from ante-mortem blunt force fractures: heat fractures are typically transverse, irregular, and associated with surface crazing (cracking pattern), while ante-mortem fractures show soft-tissue haemorrhage at the margins (vital reaction).
The boxing position (pugilistic attitude) — a characteristic flexion of the arms with flexion of the elbows and elevation of the forearms seen in badly burnt bodies — results from heat-induced contraction of flexor muscles. It does NOT indicate that the person died fighting or defending themselves. Misinterpreting the boxing position as evidence of a struggle is a classic medicolegal error.
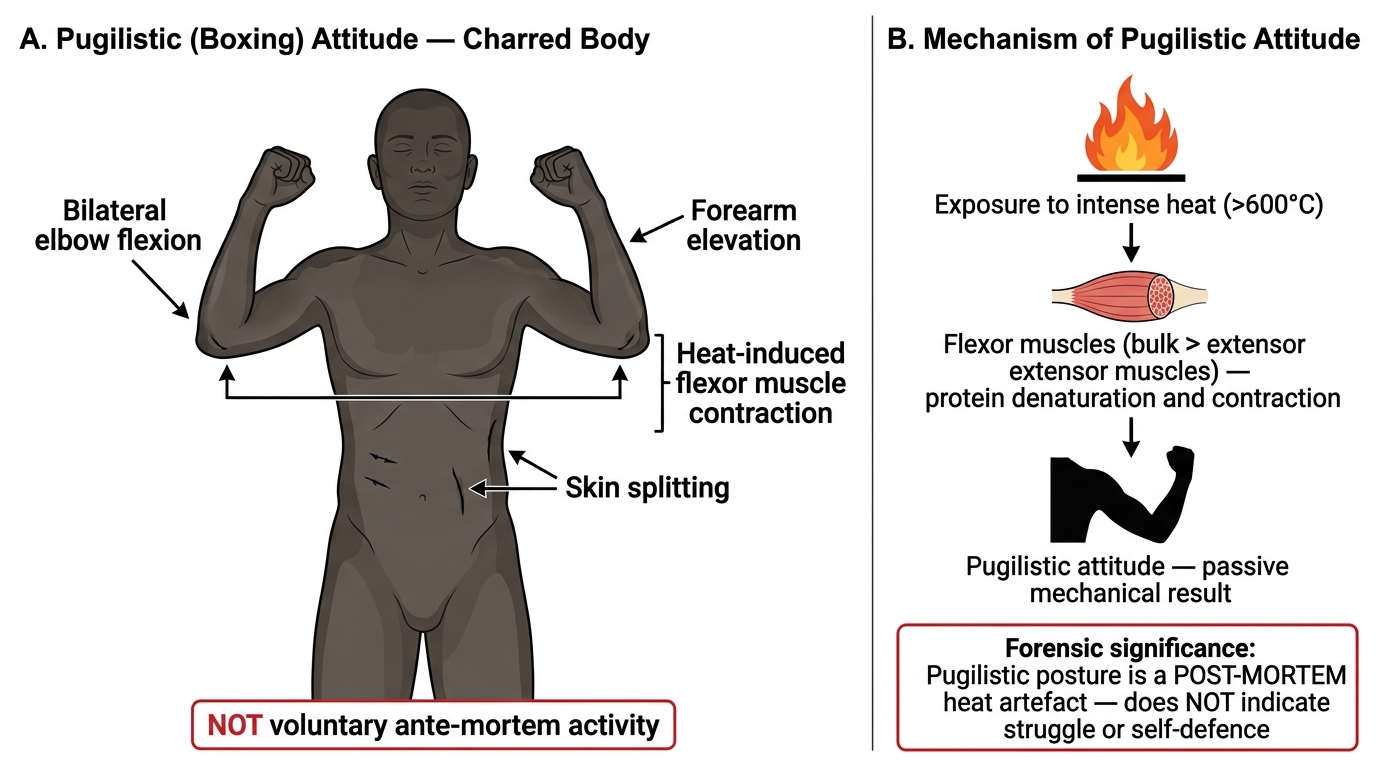
Pugilistic (Boxing) Attitude in Burnt Bodies: Appearance and Mechanism
Skeletonisation destroys most soft-tissue forensic evidence but leaves bone, teeth, and potentially DNA (particularly in dense cortical bone and teeth roots). Teeth are the most durable biological material in the body and retain forensic information even after centuries.
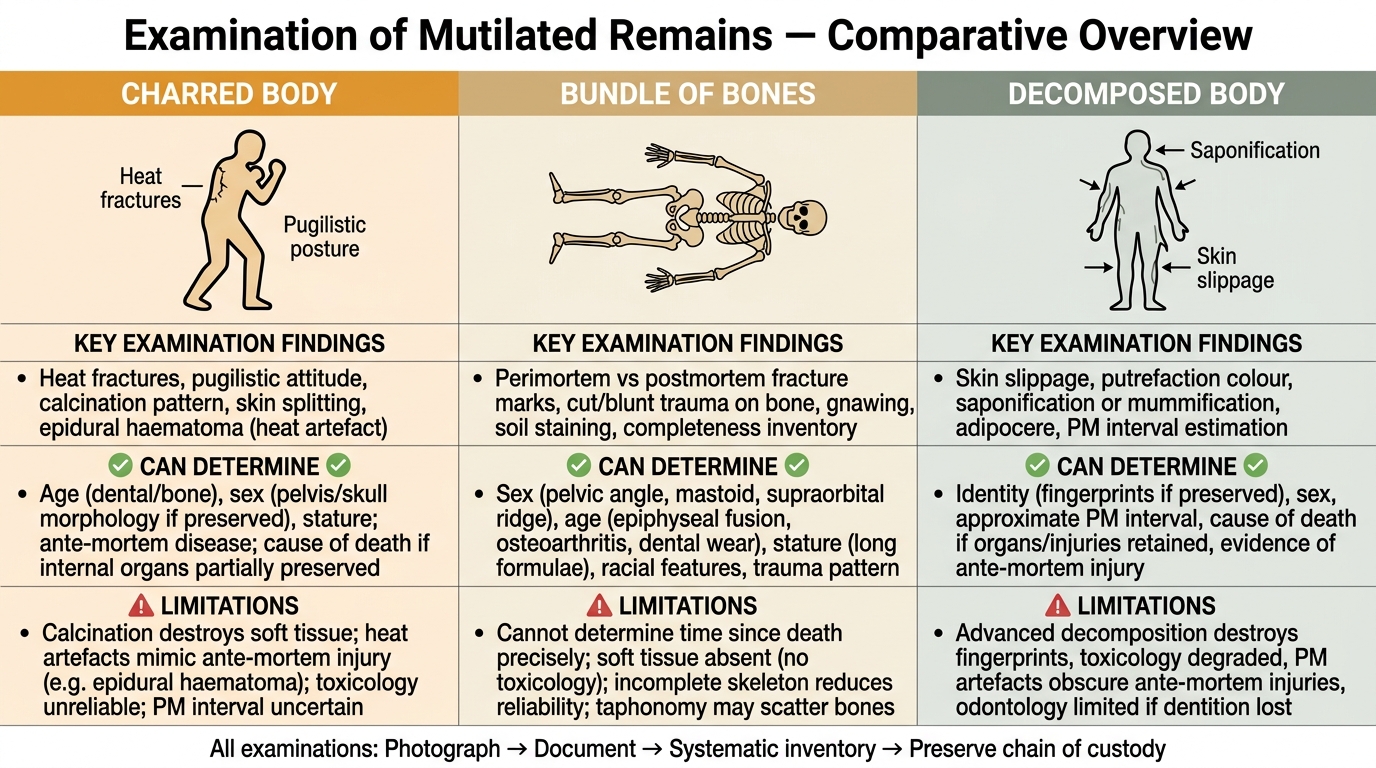
Comparison of Mutilated Remains Types: Examination Findings, Determinable Facts, and Limitations
SELF-CHECK
A body recovered from a house fire has soot deposited in the trachea and bronchi. This finding MOST LIKELY indicates that:
A. The fire was deliberately set to conceal a murder
B. The person was alive and breathing during the fire
C. The fire was of high temperature (above 700°C)
D. The body was moved to the site of the fire after death
Reveal Answer
Answer: B. The person was alive and breathing during the fire
Soot deposition in the lower airway (trachea, bronchi) is a vital reaction — it occurs only if the person was breathing during the fire. A dead body cannot aspirate soot. This finding indicates ante-mortem exposure to fire, which has critical medicolegal significance: it suggests the person was alive when the fire started, making post-mortem body burning to conceal a prior murder less likely (though the cause of death may still have been something other than the fire). It does not by itself indicate arson or murder.
Examination of Mutilated Bodies, Charred Remains, and Bundle of Bones
The examination of mutilated, charred, and skeletal remains follows the same fundamental logic as a standard autopsy — work systematically, document everything, and never assume — but with specialised techniques adapted to the specific condition of the remains.
CHARRED/BURNT REMAINS: examination sequence:
1. External examination of the intact scene (if possible before body removal): position, relationship to fire origin, presence of accelerants (petrol, kerosene), clothing remnants
2. Assess degree of charring: partial (soft tissue present), full charring (carbonised), or calcination (grey-white, crumbling)
3. Vital reaction search: (a) soot in airways — gently open mouth and larynx; (b) blood colour — cherry-red suggests CO; (c) skin blistering — ante-mortem blisters contain fluid and inflammatory cells; post-mortem heat blisters contain air and plasma
4. Sex and age estimation from surviving bone: pelvis (most reliable for sex — female has wider sub-pubic angle, oval obturator foramen, broader sciatic notch); skull (male supraorbital ridges more prominent, mastoid processes larger); long bone length for stature
5. Dental examination: each tooth charted, dental records if available compared; root fragments may yield DNA
6. Implants, prostheses, and unique identifying features
Provided image
DECOMPOSED BODY: the emphasis shifts from injury documentation to identity and cause-of-death clues. Document: stage of decomposition; entomological findings (insect species and developmental stage can estimate PMI via 'accumulated degree days'); adipocere or mummification; dental record comparison; DNA from bone or teeth; any injuries that survived decomposition (fractures, penetrating injuries leaving bone marks).
BUNDLE OF BONES / SKELETAL REMAINS: systematic inventory first:
- Count and identify every bone present; note which are missing
- Determine if human (compare with animal bone structures — key differences in skull shape, pelvis, and long bone proportions)
- Determine minimum number of individuals (MNI) if multiple individuals suspected
- Biological profile estimation:
- Sex: pelvis most reliable (female: wider sub-pubic angle >90°, oval obturator foramen, deeper sciatic notch); skull secondary
- Age: for subadults — epiphyseal fusion timings (Indian reference per Reddy's); for adults — Gustafson's method (6 criteria on tooth sections: attrition, periodontosis, secondary dentine, cementum apposition, root resorption, root translucency — each scored 0–3, maximum 18; age derived from regression formula)
- Stature: long bone lengths converted using Indian regression formulae (Pearson's or Indian-adapted formulae from Reddy's — do NOT use Western reference values)
- Ancestry: more complex; usually requires specialist input
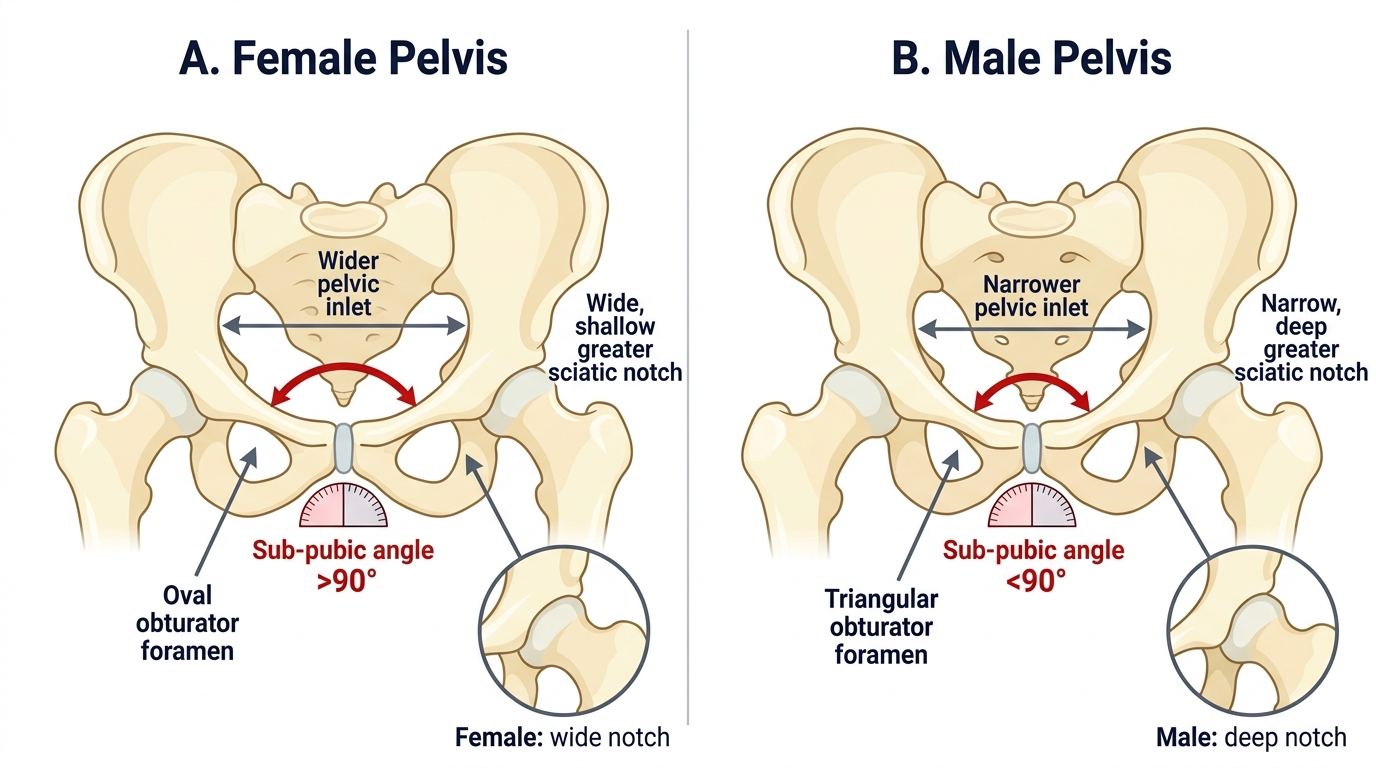
Sex Determination from Skeletal Pelvis: Female vs. Male Morphology
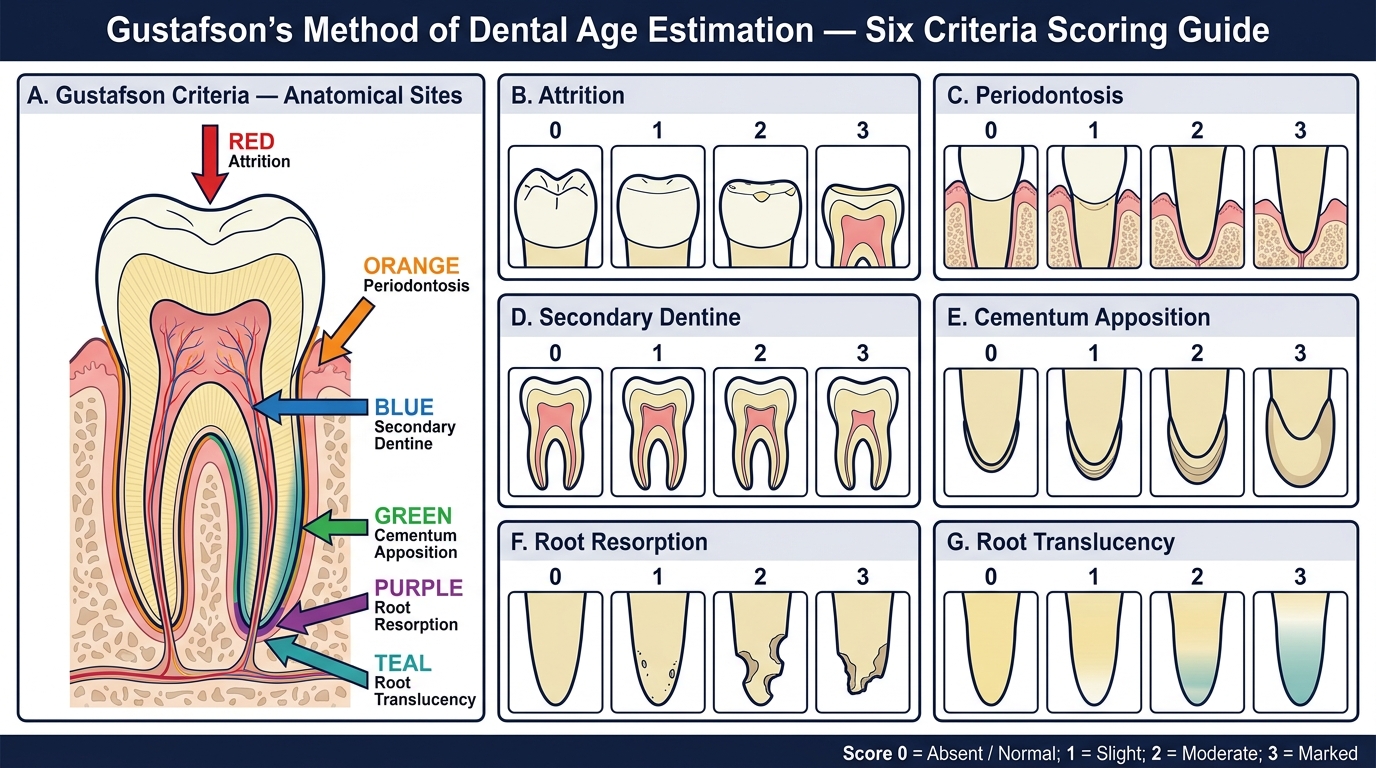
Gustafson's Six Dental Age Estimation Criteria (Score 0–3)
DISMEMBERED BODY: document each fragment separately; attempt to reconstruct the body to assess completeness; examine saw/cut marks on bone for tool mark analysis; look for overlapping injuries; DNA from all pieces for identity.
SELF-CHECK
For sex determination from skeletal remains, the MOST reliable bone is:
A. The femur
B. The skull
C. The pelvis
D. The sternum
Reveal Answer
Answer: C. The pelvis
The pelvis is the most reliable bone for sex determination in skeletal remains, with an accuracy of approximately 95% by an experienced examiner. Key differences: females have a wider sub-pubic angle (>90°), an oval obturator foramen, and a deeper, more rounded sciatic notch. The skull provides secondary sex estimation with lower accuracy (~90%). The femur and sternum are used for stature and age estimation respectively.
Exhumation: Legal Requirements and Procedure
Exhumation is the disinterment of a buried body for forensic examination. It is ordered when: (1) the original PM was incomplete or inconclusive; (2) new evidence has emerged after burial suggesting a different cause or manner of death; (3) the identity of the buried person is contested; (4) specimens not collected at the original PM are needed (e.g. toxicological samples in a suspected poisoning where poison was not suspected at the time of burial); or (5) the original PM report is being legally challenged.
Legal requirement — court order is mandatory: Exhumation in India requires a magistrate's order (court order). A police officer's written request alone is not sufficient legal authority. This is a critical distinction that is frequently tested in examinations and arises in practice. The court order specifies the location, identifies the person to be exhumed, names the examining physician(s), and authorises the presence of specified parties.
Who must be present at exhumation:
- The magistrate (or a representative)
- The forensic physician(s) — ideally the same doctor who conducted the original PM, if applicable, plus a second independent examiner
- The investigating police officer
- A panchas (witnesses — typically two impartial local residents)
- A representative of the family (if they request)
- A cemetery/graveyard official
Procedure:
1. Documentation before disinterment: photograph the grave as found; note condition, any disturbance, vegetation growth, soil condition
2. Careful disinterment: soil removal in layers; note soil staining, fluids, insect activity; preserve any objects found in or around the coffin/shroud
3. External examination of remains as exhumed: position, clothing/shroud condition, any objects present
4. Transportation: transfer to mortuary for detailed examination under proper conditions — not examination at graveside
5. Examination at mortuary: identical to standard PM examination sequence, with attention to: the state of preservation (adipocere? decomposition? skeletal?), findings that were noted in the original PM, new findings not previously documented, specimen collection for toxicology/histology/DNA
6. Specimens: blood (if available), bone marrow, bone, liver and kidney (if preserved), gastric contents, hair and nails (for toxicology — heavy metals and some drugs persist), and soil samples from around the body for comparison
7. Reburial: the body MUST be reburied after the examination is completed. It cannot be retained indefinitely. The magistrate oversees the reburial and it is documented.
8. Report: submitted to the magistrate; cross-referenced with the original PM report; specific findings compared and discrepancies addressed
Evidentiary value and limitations: exhumation can yield new evidence from preserved specimens, reveal injuries missed at the original PM, and confirm or contradict the original cause of death opinion. However, decomposition reduces the quality of evidence with time: toxicological analysis of putrefied tissue has limitations; bruise dating becomes impossible in decomposed tissue; and post-mortem changes may mimic ante-mortem injuries. The forensic physician must clearly state in the report what the state of preservation allows and what it precludes.
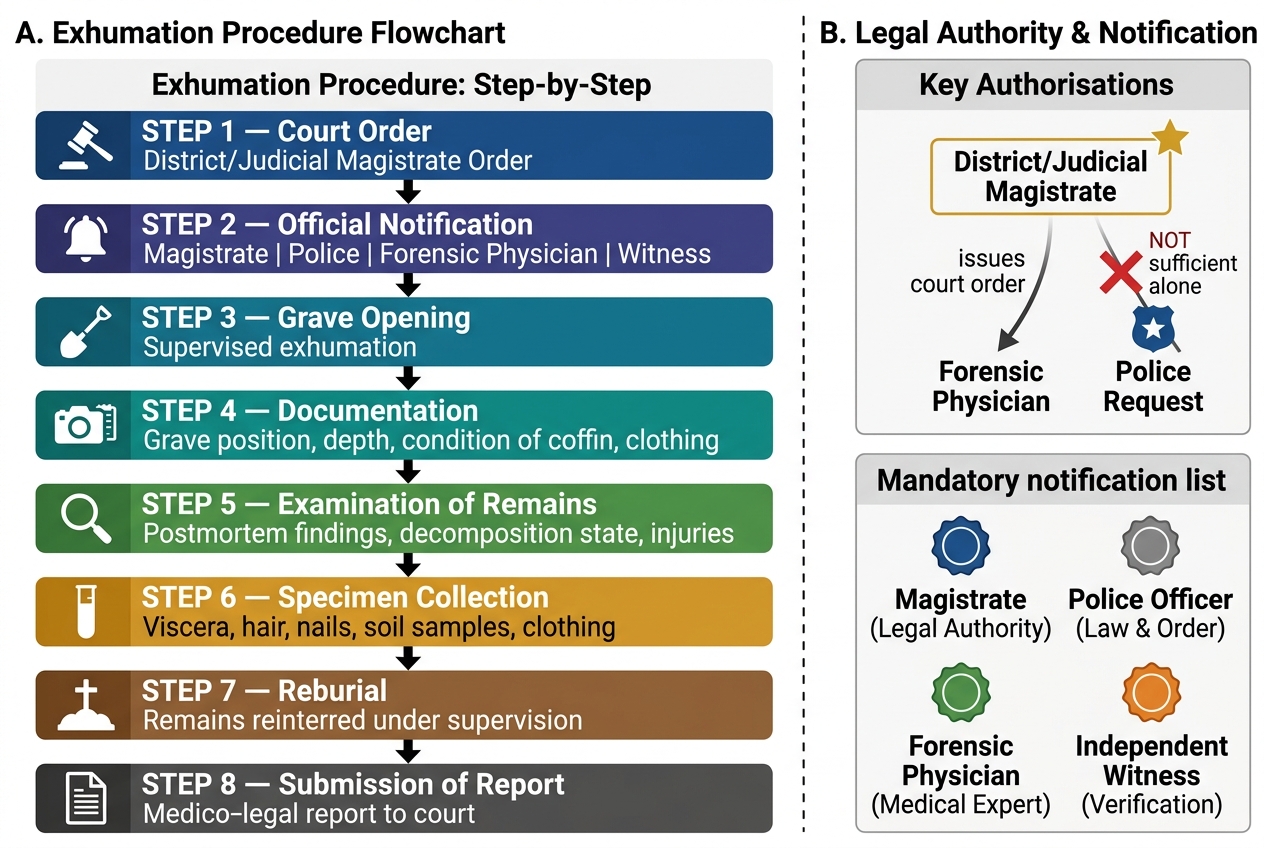
Exhumation Procedure: Legal Authority, Sequential Steps, and Mandatory Notifications
CLINICAL PEARL
Pearl: The boxing position (pugilistic attitude) does NOT mean the person was alive and fighting. This is one of the most common medicolegal misinterpretations in fire deaths. The characteristic flexion of the arms with elbow flexion and raised forearms in badly burnt bodies is caused entirely by heat-induced contraction and shortening of flexor muscle groups — the flexors are larger and stronger than extensors and contract differentially when protein is denatured by heat. The position occurs in bodies that were both alive and dead when fire started. To determine whether the person was alive in the fire, look for vital reactions (soot in airways, CO in blood, ante-mortem blisters with inflammatory cells) — not body position.
SELF-CHECK
Exhumation in India requires which of the following as the primary legal authority?
A. Written request from the police officer in charge of the case
B. Order from the District Magistrate or Judicial Magistrate
C. Consent from the deceased's family
D. Application from the forensic physician conducting the examination
Reveal Answer
Answer: B. Order from the District Magistrate or Judicial Magistrate
Exhumation requires a court order from a magistrate — a police request alone is insufficient. This is a critical legal point that distinguishes exhumation from standard medico-legal autopsies (which can be ordered by police under CRPC Section 174). The magistrate's order specifies the site, persons to be present, and purposes of the examination. Family consent is not required but family representation may be permitted.
KEY TAKEAWAYS
Examination of mutilated remains requires a structured approach centred on vital reaction detection, identity determination, and maximum information extraction from compromised evidence. Charred bodies: vital reactions (soot in airways, cherry-red CO-saturated blood, ante-mortem blisters with inflammatory cells) establish whether the person was alive in the fire. The boxing position is a heat artefact, not a sign of ante-mortem activity. Bundle of bones (skeletal remains): biological profile via sex (pelvis most reliable), age (Gustafson's 6-criteria dental method for adults; epiphyseal fusion for subadults using Indian reference values), and stature (Indian regression formulae). Decomposed bodies: entomology assists PMI; adipocere and mummification preserve forensic evidence despite appearance. Exhumation requires a magistrate's court order — not a police request. The body is examined in the mortuary, not at the graveside; specimens collected; and the body MUST be reburied after examination. Exhumation yield decreases with time as decomposition advances; the forensic physician must state explicitly what the state of preservation allows and precludes.
REFLECT
You are asked to conduct an exhumation in a case where a family alleges their relative was murdered six months ago but the original PM reported 'death by natural causes.' At the grave, you find the body in an advanced state of putrefaction. Before beginning, you need to counsel the family on what the examination can and cannot reasonably be expected to establish six months after death. How would you explain the limitations of forensic evidence after decomposition to a grieving family with strong suspicions of foul play, while maintaining scientific accuracy and professional compassion?