Page 5 of 16
FM11.3-4 | Criminal & Civil Responsibility; Feigned Illness — SDL Guide (Part 2)
Feigned Mental Illness: Malingering and Its Detection
Malingering is the deliberate, conscious simulation or gross exaggeration of physical or mental symptoms, motivated by external incentives — avoiding criminal conviction, securing financial compensation, obtaining disability certification, evading military service, or gaining admission to hospital to escape an adverse situation. The critical features of malingering are that it is (1) fully conscious and deliberate, (2) goal-directed toward a specific external gain, and (3) NOT a mental disorder — malingering does not appear as a diagnosis in ICD-11 or DSM-5; it is listed as a condition that may be a focus of clinical attention.
This distinguishes malingering from factitious disorder (previously Munchausen syndrome), where the person deliberately induces or fabricates symptoms primarily for the psychological need to assume the sick role rather than for tangible external gain. It also distinguishes malingering from somatic symptom disorders, where symptoms are genuine (even if pathophysiology is not fully explained) and not deliberately feigned.
The detection of malingering in a forensic psychiatric setting requires a multi-source, multi-method approach:
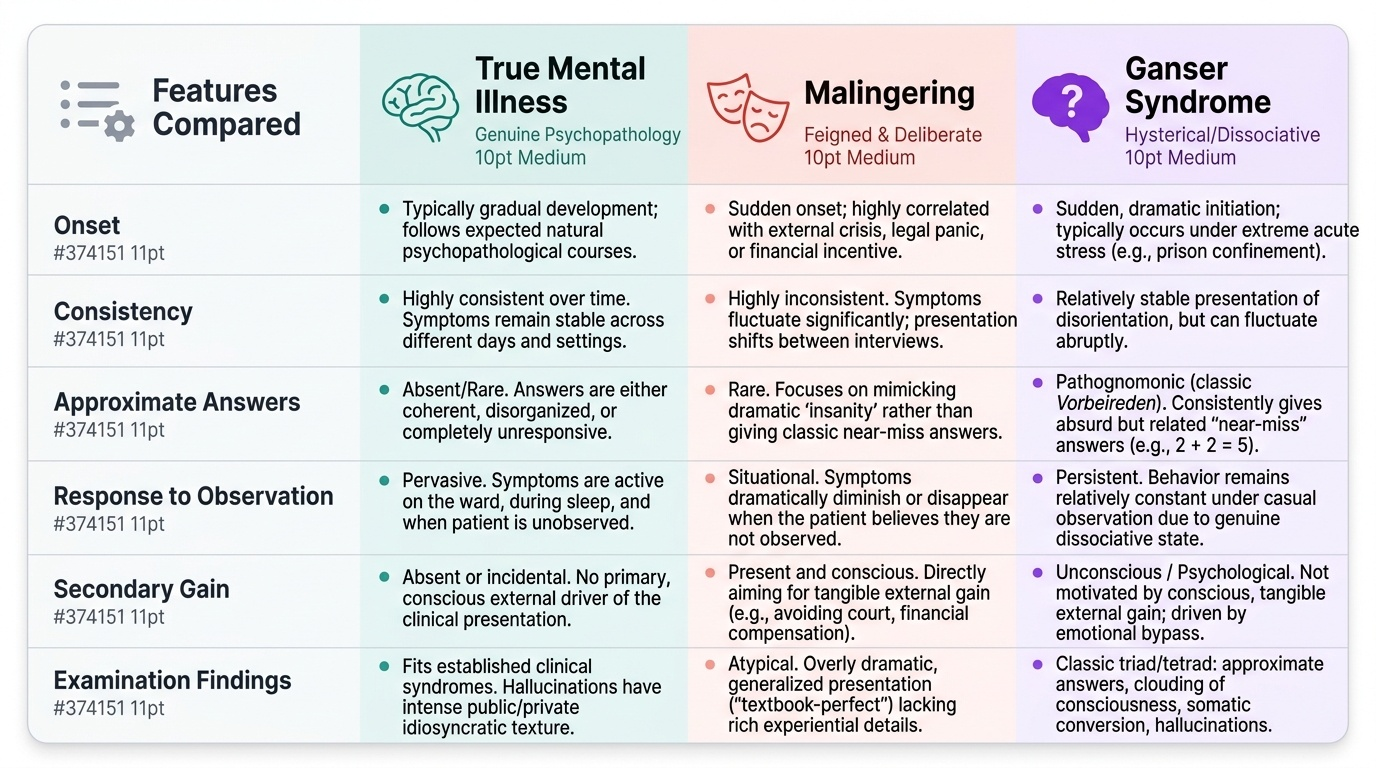
1. History inconsistency analysis: A malingerer typically presents symptoms that are textbook-perfect — gleaned from internet searches or accounts of genuinely ill patients — but fails to describe the full experiential texture of illness. True psychotic patients describe their hallucinations with idiosyncratic, private, sometimes bizarre content that reflects their specific history and personality. Malingerers tend to describe generic symptoms ("I hear voices") without the specific, personal content that characterises genuine auditory hallucinations. Interview the patient multiple times across different days — genuine psychotic symptoms have a degree of consistency (they are driven by a real underlying process), while deliberately fabricated symptoms frequently shift inconsistently.
2. Behaviour outside the formal interview: Genuine psychosis is pervasive — it affects the patient's behaviour with ward staff, other patients, and family visitors, not only during the formal examination. Observation on the ward is essential. A patient who is incoherent and unresponsive during the formal psychiatric interview but engages in a card game, checks their phone, and discusses cricket scores with other patients during recreational time is displaying behaviour inconsistent with the severity of claimed symptoms.
3. Response to suggested symptoms: A useful clinical manoeuvre is to ask leading questions that suggest symptoms the patient does not have. For example: "I understand you also sometimes smell flowers that aren't there?" A genuine patient typically denies symptoms they do not have. A malingerer, eager to appear maximally ill, often agrees to suggested symptoms.
4. Psychological testing: Structured instruments such as the Structured Inventory of Malingered Symptomatology (SIMS) and the Miller Forensic Assessment of Symptoms Test (M-FAST) are validated malingering detection tools, though their availability in Indian settings is variable.
5. Review of antecedent records: The absence of any prior contact with mental health services, in a person now claiming chronic and severe mental illness sufficient to negate criminal responsibility, is a red flag requiring careful explanation.
Provided image
SELF-CHECK
During a ward observation, a prisoner referred for fitness-to-plead assessment speaks incoherently and appears grossly disorganised during all formal psychiatric interviews. However, nursing staff report that he consistently beats other prisoners at chess and gives accurate legal advice to other inmates about bail procedures. What does this most strongly suggest?
A. True schizophrenia with preserved procedural memory despite psychosis
B. Ganser syndrome with approximate answers
C. Malingering — behaviour inconsistent with claimed severity outside formal interview
D. Bipolar disorder in a manic phase with flight of ideas
Reveal Answer
Answer: C. Malingering — behaviour inconsistent with claimed severity outside formal interview
The key finding is the stark contrast between behaviour during formal examination (incoherent, disorganised) and behaviour when not under observation (skilled chess, accurate legal knowledge). Genuine severe schizophrenia is pervasive — it affects behaviour across all contexts, not selectively during interviews. The ability to play complex strategic games and provide accurate legal information is entirely inconsistent with the level of disorganisation presented during interviews. This pattern is the hallmark of malingering: symptom performance is reserved for the examining audience.
Ganser Syndrome: The Medicolegal Trap
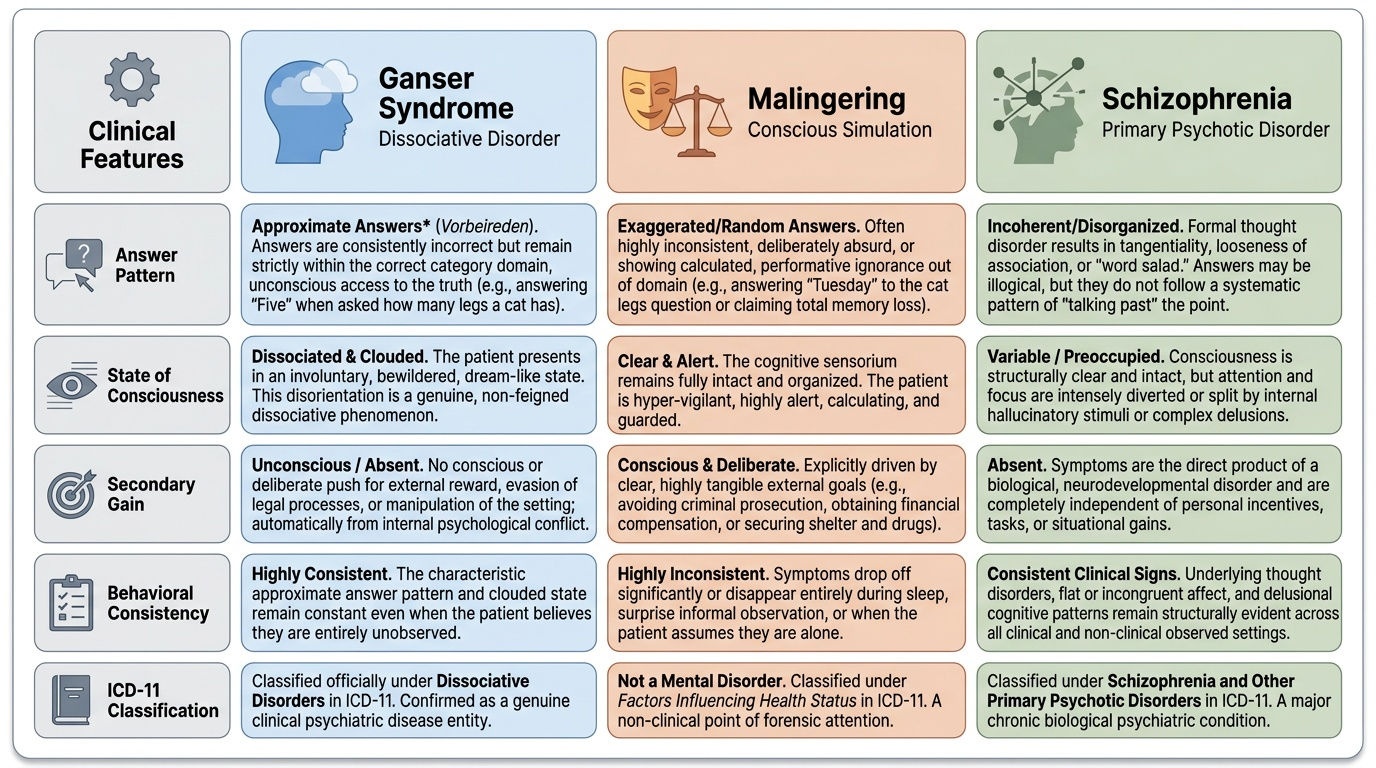
Ganser syndrome is a genuine dissociative disorder — classified under Dissociative Disorders in ICD-11 — that is of particular importance in forensic settings because it can easily be mistaken for malingering by inexperienced examiners, and can equally be mistaken for a primary psychotic disorder by clinicians unfamiliar with its distinctive features. Getting this wrong in either direction is a serious forensic error: diagnosing a genuine Ganser syndrome patient as a malingerer exposes a truly ill person to unjust criminal punishment; diagnosing a malingerer as having Ganser syndrome creates a false safe haven for simulation.
The syndrome was first described by Sigbert Ganser in 1898 in prisoners, and its forensic psychiatric context is therefore longstanding. Ganser syndrome is characterised by four cardinal features:
- Approximate answers (Vorbeireden, literally "talking past the point"): The patient gives answers that are clearly wrong but clearly demonstrate knowledge of the correct answer. This is the pathognomonic feature. When asked "How many legs does a cat have?" the patient answers "Five." When asked "What colour is the sky?" the patient answers "Green." The patient is not guessing randomly — the answer is in the correct domain (not "Tuesday" in response to the cat legs question) but is consistently just off. This is qualitatively different from a genuinely confused patient (who may answer randomly or perseverate) and qualitatively different from a malingerer trying to seem maximally ignorant (who would also show this pattern but with a deliberate and controlled quality).
- Clouded or altered consciousness: The patient appears bewildered, disoriented, and in a dream-like state — this is a dissociative alteration of consciousness, not a simple loss of consciousness.
- Somatic conversion symptoms: Hysterical paralysis, anaesthesia, or other conversion features may accompany the syndrome.
- Hallucinations and other psychotic-like symptoms: These may be present and may superficially resemble a psychotic illness.
Distinguishing Ganser syndrome from malingering: In Ganser syndrome, the approximate answers are unconsciously produced — the patient is not deliberately choosing a slightly wrong answer; the dissociative process produces this response automatically. In malingering, the answers are deliberately chosen to appear wrong. In practice, this distinction can be extremely difficult to make with certainty, which is why Ganser syndrome is said to be the "medicolegal trap." The critical approach is that Ganser syndrome requires a formal diagnosis from a trained psychiatrist, grounded in the full clinical picture; it should not be invoked as a convenient middle-ground category.
Distinguishing Ganser syndrome from primary psychosis: In schizophrenia, thought disorder produces incoherent or tangentially connected responses; in Ganser syndrome, the responses are structurally appropriate (in the correct domain, grammatically coherent) but consistently just off. The other dissociative features (altered consciousness, conversion symptoms) are not a feature of schizophrenia.
The forensic significance: if Ganser syndrome is genuinely present in a forensic context, it does not automatically provide the McNaughten defence — the key question remains whether, at the time of the act, the accused could not know the nature or wrongness of the act. Ganser syndrome in its acute phase may or may not meet this threshold, depending on severity.
Provided image
CLINICAL PEARL
Four forensic points that distinguish the expert from the novice:
- McNaughten is cognitive, not volitional. The test asks "did not know" — not "could not control." An accused who knew what they were doing was wrong but "couldn't stop themselves" does NOT satisfy the Indian insanity defence. This point is frequently misunderstood by defence lawyers, and a confident forensic physician must be prepared to explain it in court.
- Voluntary intoxication is never a McNaughten defence. If the accused voluntarily drank alcohol or took drugs and then committed the act in an intoxicated state without awareness, BNS Section 22 does not apply. The voluntariness of the intoxication breaks the causal chain between the "disease of the mind" and the incapacity. Involuntary intoxication (someone drugged without knowledge) is different.
- Ganser syndrome is a genuine ICD-11 diagnosis, not a fancy word for malingering. Calling Ganser syndrome "sophisticated malingering" in court — as if they were synonymous — is an error that will be challenged and can destroy your credibility as an expert witness.
- Assess at two time points. Every forensic psychiatric report must explicitly address BOTH: (a) the mental state at the time of the act (retrospective — based on available records, witnesses, police reports, medical notes) AND (b) the current mental state at the time of examination (for fitness to plead). Conflating the two is one of the most common errors in forensic psychiatric reports.
Conducting and Reporting the Fitness-to-Plead Assessment
The Mental Healthcare Act 2017 (MHA 2017) and the Code of Criminal Procedure (CrPC) (now largely replaced by the Bharatiya Nagarik Suraksha Sanhita 2023, BNSS) establish the statutory framework for court-ordered psychiatric evaluations. Under BNSS Section 367 (formerly CrPC Section 328), when a Magistrate has reason to believe that the accused is of unsound mind, the proceedings may be stayed and the accused sent for medical examination. Under BNSS Section 368, if the accused is found unfit to plead, the trial is postponed until capacity is restored or a guardianship proceeding is initiated.
Fitness to plead is a distinct concept from criminal responsibility at the time of the act. Fitness to plead assesses current mental capacity to participate meaningfully in the trial process: (a) understanding the nature of the charge, (b) following court proceedings, (c) instructing legal counsel, (d) challenging prosecution witnesses, and (e) understanding the significance of the evidence. A person who was genuinely insane at the time of the act may have since recovered and be fully fit to plead today. Conversely, a person who committed the act in a sane state may have since deteriorated and become unfit to plead.
Structure of the forensic psychiatric court report on responsibility and feigned illness must include:
- Personal particulars and source of referral — who ordered the examination and under which provision.
- History — present illness history, past psychiatric history, family history, substance use, prior forensic contacts, treating physician records, police remand reports.
- Current mental status examination (MSE) — all domains: appearance, behaviour, speech, mood, affect, thought content, thought form, perceptions, cognition (MMSE if indicated), insight, judgment.
- Reliability assessment — explicit statement on whether clinical findings are internally consistent, consistent with collateral history, and consistent with ward behaviour observations. Document any detected inconsistencies.
- Diagnosis (ICD-11) — formal diagnostic conclusion.
- Opinion on criminal responsibility — applying the McNaughten test: (a) was a mental disorder present at the time of the act? (b) if yes, did it deprive the accused of the ability to know the nature of the act OR that it was wrong? Support each conclusion with specific findings from the examination and history.
- Opinion on fitness to plead — current capacity across the five fitness-to-plead domains listed above.
- Opinion on genuineness of illness — explicit statement on whether the findings are consistent with genuine mental illness, deliberate simulation (malingering), or a genuine dissociative disorder (Ganser syndrome).
The MHA 2017 additionally requires that any person admitted to a mental health establishment be admitted only under its provisions (voluntary, supported, or involuntary admission) — the forensic physician must be familiar with these pathways so that the court can direct the appropriate disposition if the accused is found unfit to plead or is acquitted on grounds of insanity.
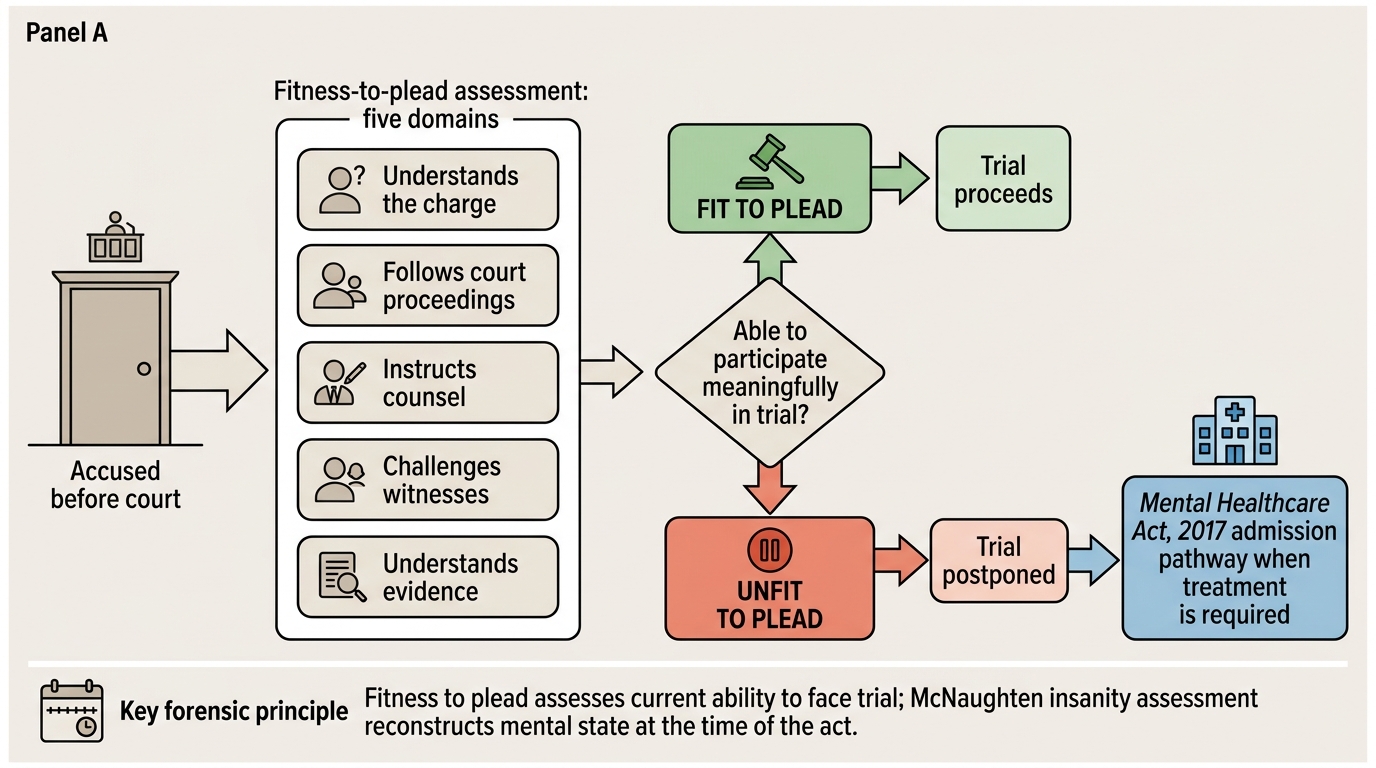
Fitness-to-Plead Assessment Flowchart
SELF-CHECK
A forensic psychiatric board report states that the accused currently shows no symptoms of mental illness and is fully oriented. However, witness accounts from the time of the act describe him speaking to invisible persons, expressing fear that he was being chased by evil spirits, and making no attempt to flee after the assault. What is the correct approach to the McNaughten assessment?
A. Since the accused is currently sane, the insanity defence cannot apply
B. The assessment must focus on the retrospectively reconstructed mental state at the time of the act, not the current examination
C. The witness accounts are inadmissible hearsay and cannot inform the forensic opinion
D. Current sanity proves the accused was always sane and was malingering at the time of the act
Reveal Answer
Answer: B. The assessment must focus on the retrospectively reconstructed mental state at the time of the act, not the current examination
The McNaughten test under BNS Section 22 is explicitly retrospective — it asks about the mental state 'at the time of doing' the act. A current recovery does not extinguish the defence; the assessment requires reconstructing mental state at the time of the act from all available evidence: contemporaneous medical records, witness accounts, police reports, and the pattern of symptom onset and treatment. Witness accounts are admissible as part of the clinical history and can be relied upon by the expert witness. The forensic physician must clearly distinguish the two time points: mental state at time of act (governs criminal responsibility) and mental state at time of examination (governs fitness to plead).