Page 7 of 16
FM11.5 | Delirium Tremens — SDL Guide
Learning Objectives
- Describe the pathophysiology of Delirium Tremens (DT) as a severe alcohol withdrawal syndrome
- Identify the clinical features of DT and distinguish them from Wernicke's encephalopathy and Korsakoff syndrome
- Apply the thiamine-before-glucose rule and outline the management principles for severe alcohol withdrawal
- Explain the forensic significance of DT, including its role in custody deaths and its distinction from primary psychotic disorders
INSTRUCTIONS
Delirium Tremens is simultaneously a medical emergency and a forensic challenge. It kills within hours when unrecognised, and it occurs precisely in the populations most commonly encountered in forensic settings — prisoners brought in intoxicated, habitual heavy drinkers admitted for observation, or detainees held without medical assessment. Understanding DT means understanding that it is not intoxication but its opposite — it is the crisis of withdrawal — and that the Wernicke-Korsakoff spectrum it precipitates represents one of the most preventable causes of permanent neurological disability. This module covers DT from pathophysiology through forensic documentation.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old habitual daily drinker is arrested for a breach of peace and lodged in a lock-up at 10 PM. He appears intoxicated on admission and is given water and left in the cell. He is noisy through the night. At 7 AM two days later, the jailer finds him unresponsive on the floor. The police call you as the medical officer on duty. On arrival, the man is deeply unconscious, diaphoretic, with a temperature of 39.2°C, a rapid irregular pulse at 128/min, and blood pressure of 90/60 mmHg. There are fresh bruises consistent with falls. He cannot be roused. What has happened in those 48 hours, and what medicolegal and clinical obligations did the police and the duty medical officer fail to meet?
WHY THIS MATTERS
Delirium Tremens is not a clinical curiosity — it is a life-threatening, preventable emergency that demands immediate recognition. Its forensic relevance is multilayered: it is a known cause of sudden, unexpected death in police lock-ups and prisons; its misidentification as simple intoxication or feigned illness has resulted in preventable deaths and subsequent inquests; and the psychotic features it produces — vivid visual hallucinations, extreme agitation, delirious conviction — can superficially mimic a primary psychotic disorder, creating misdiagnosis risk. The Wernicke-Korsakoff spectrum it precipitates is one of the most preventable causes of permanent amnestic disorder in India. A forensic physician who cannot recognise, manage, and document DT is a liability both clinically and medicolegally.
RECALL
From Year-1 Physiology, recall that GABA (gamma-aminobutyric acid) is the principal inhibitory neurotransmitter and glutamate is the principal excitatory neurotransmitter in the CNS. Recall from Pharmacology that alcohol is a CNS depressant — it potentiates GABA receptors (specifically GABA-A) and inhibits NMDA-type glutamate receptors. From Biochemistry, recall that thiamine (Vitamin B1) is an essential coenzyme for several key metabolic pathways in the brain, including the pentose phosphate pathway and the citric acid cycle. With this foundation, the pathophysiology of DT and Wernicke's encephalopathy will be immediately logical.
A Death in Police Custody: Alcohol Withdrawal as a Forensic Emergency
Every year, deaths in police custody trigger inquests, magisterial investigations, and often public controversy. Among the identifiable medical causes of such deaths, Delirium Tremens (DT) and its complications occupy a significant and largely preventable category. When a habitual heavy drinker is abruptly deprived of alcohol — whether by arrest, hospitalisation, illness, or economic disruption — the brain's compensatory adaptations to chronic alcohol exposure are suddenly unmasked, generating a syndrome of CNS and autonomic hyperexcitability that can be fatal if not recognised and treated.
The forensic physician is called to custody deaths for two distinct purposes: first, to determine the cause of death at post-mortem; and second, retrospectively, to advise the investigating magistrate on whether the death was preventable — whether adequate medical care was provided and whether the warning signs were acted upon. In a DT-related custody death, both purposes hinge on the same question: did the detaining authorities and the duty medical officer recognise the early features of withdrawal and initiate treatment, or did they mistake the agitation and confusion of developing DT for intoxicated misbehaviour and leave the prisoner unattended?
The medicolegal significance of DT in custody therefore extends beyond clinical medicine. It intersects with the state's duty of care to detainees (established under Article 21 of the Indian Constitution — right to life, which courts have interpreted to include a right to healthcare in detention), the provisions of the Mental Healthcare Act 2017 that require assessment and care of substance use disorders, and the criminal negligence provisions of IPC Section 304A (reckless or negligent act causing death) — now mirrored in BNS — that can apply to medical officers who fail to assess a deteriorating detainee.
Alcohol Withdrawal Timeline and Duty of Care
Pathophysiology of Delirium Tremens
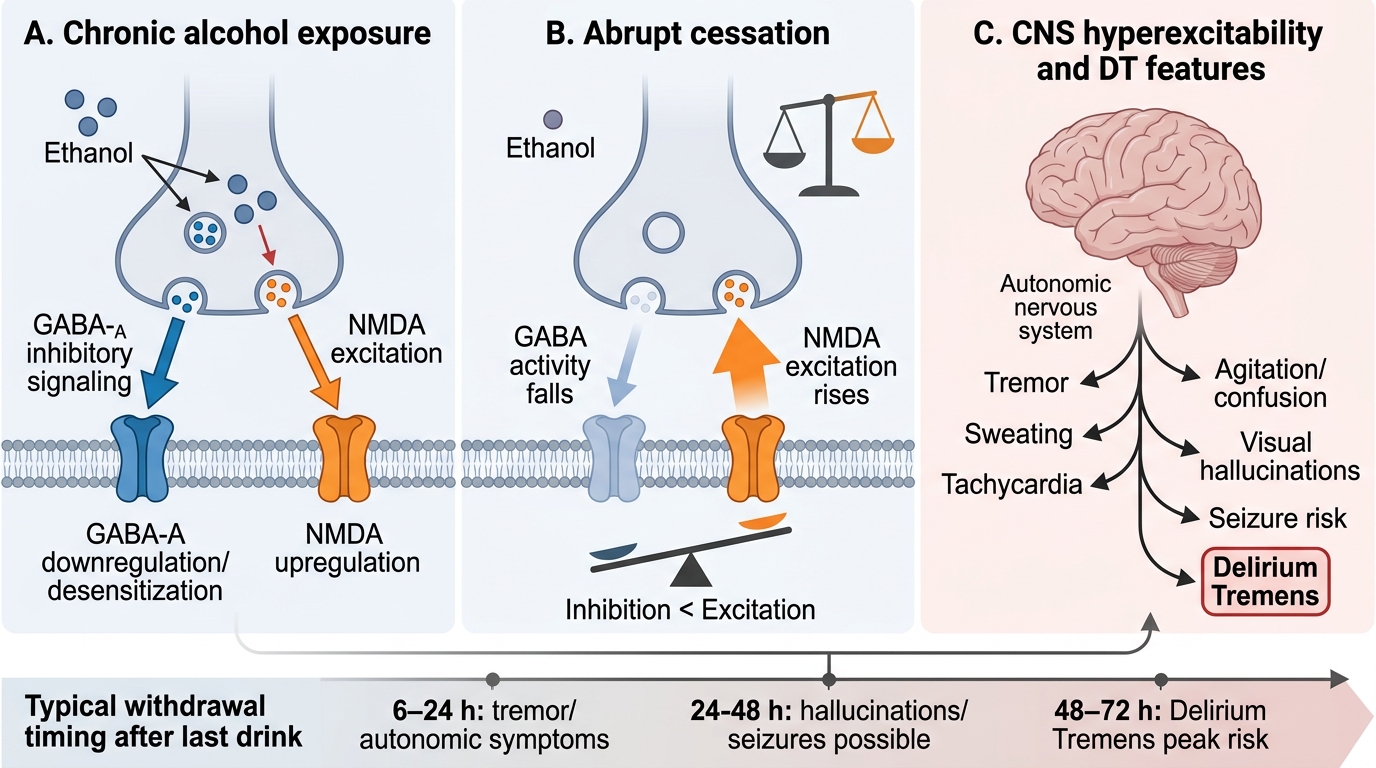
The pathophysiology of DT is best understood as the neurochemical consequence of sudden withdrawal of a substance that has chronically recalibrated the brain's excitatory-inhibitory balance. Chronic, heavy alcohol consumption leads to profound and lasting adaptations in CNS neurotransmitter systems: (1) GABA-A receptor downregulation and desensitisation — because alcohol continuously potentiates inhibitory GABAergic signalling, the brain compensates by reducing the number and sensitivity of GABA-A receptors; and (2) NMDA glutamate receptor upregulation — because alcohol chronically suppresses excitatory NMDA glutamate signalling, the brain compensates by increasing NMDA receptor expression and sensitivity.
When alcohol is abruptly discontinued, both adaptations are simultaneously unmasked. The GABAergic inhibitory tone falls sharply (because receptors are downregulated) while the glutamatergic excitatory drive surges (because receptors are upregulated). The net effect is a state of profound CNS hyperexcitability — manifesting as tremor, agitation, seizures, and ultimately the full clinical picture of DT. Crucially, this is the OPPOSITE of the intoxicated state. The drunk patient is sedated; the withdrawing patient is hyperexcitable.
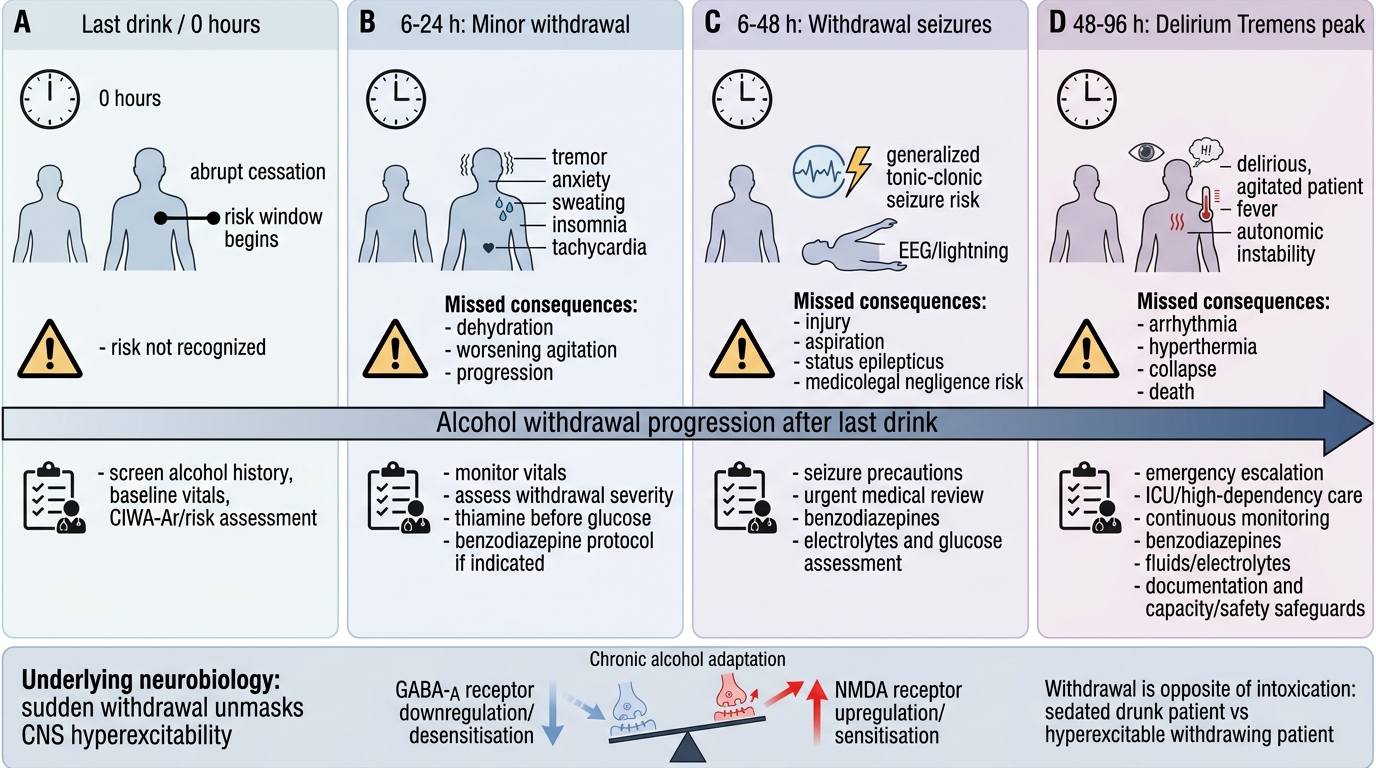
The temporal profile of this process follows a predictable pattern after the last drink:
- 6-24 hours: Minor withdrawal symptoms — tremor, anxiety, diaphoresis, tachycardia, headache, nausea. These are the warning signs.
- 6-48 hours: Withdrawal seizures — generalised tonic-clonic seizures ("rum fits"), typically self-limited, but a predictor of impending severe withdrawal.
- 48-96 hours (peak at 72-96 hours): Full Delirium Tremens — the combination of autonomic instability, delirium, and hallucinations. This is the dangerous phase.
The kindling phenomenon is an important clinical concept: each successive episode of alcohol withdrawal tends to be more severe than the previous one, because the neuroplastic changes become more entrenched with each cycle. A patient who experienced mild withdrawal symptoms after their first attempt to quit may develop full DT after a subsequent cessation — the clinical history of prior withdrawal severity is therefore a critical prognostic indicator.
The autonomic hyperactivity in DT — tachycardia, hypertension, hyperthermia, diaphoresis — is driven by heightened sympathetic discharge, which can precipitate fatal cardiac arrhythmias or cardiovascular collapse. It is this autonomic storm that most commonly causes death in untreated DT.
Neurochemical Basis of Alcohol Withdrawal and Delirium Tremens
SELF-CHECK
A 50-year-old man with chronic alcohol use disorder is admitted to hospital for an unrelated surgical procedure. His last drink was 36 hours ago. He is now trembling, sweating profusely, and appears confused and frightened. He reports seeing small animals crawling on the walls. What is the most likely diagnosis?
A. Acute alcohol intoxication
B. Wernicke's encephalopathy
C. Delirium Tremens in development
D. Korsakoff syndrome
Reveal Answer
Answer: C. Delirium Tremens in development
This presentation — 36-48 hours after the last drink, with tremor, diaphoresis, confusion, and visual hallucinations — is classic early Delirium Tremens developing in a chronic alcohol-dependent patient after abrupt cessation. The 36-hour timing is in the typical 48-72 hour DT window (the onset window begins at 48 hours but early features can appear sooner). This is NOT intoxication (which presents with sedation, not agitation). Wernicke's encephalopathy presents with the triad of confusion + ophthalmoplegia + ataxia and is a thiamine deficiency syndrome that may co-occur but is distinct. Korsakoff syndrome is a chronic amnestic state — not an acute presentation.
Clinical Features and the Wernicke-Korsakoff Spectrum
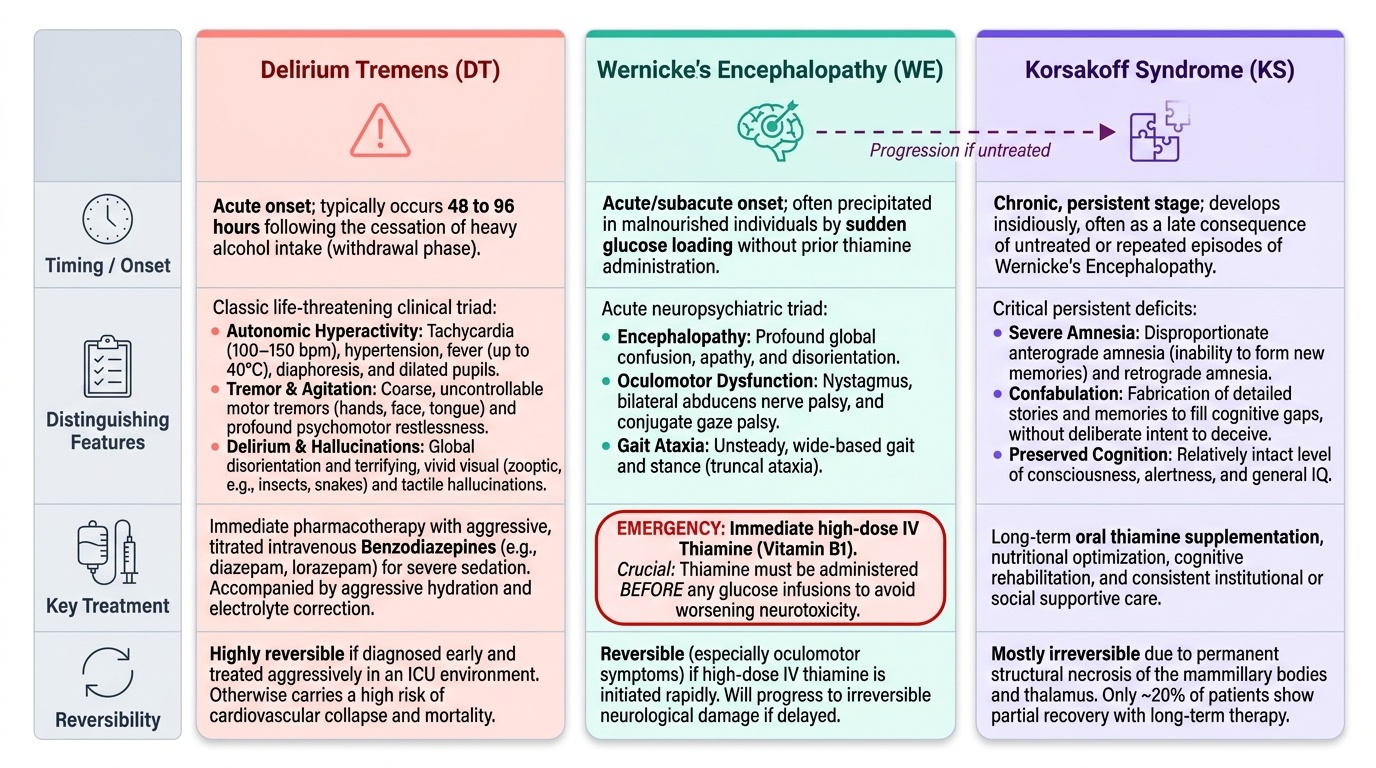
The full clinical picture of established Delirium Tremens combines three overlapping components that form a life-threatening triad:
1. Tremor and psychomotor agitation: Coarse tremor of the hands, face, and tongue — the original basis for the name "tremens." The patient is profoundly agitated, restless, and may show purposeless picking or grasping movements. They cannot remain still.
2. Autonomic hyperactivity: Tachycardia (heart rate commonly 100-150 bpm), hypertension, fever (low-grade to >40°C), diaphoresis, and dilated pupils. This is the most dangerous component — hyperthermia and cardiac arrhythmia are the proximate causes of DT-associated death. Blood pressure may swing dramatically, and the cardiovascular strain in a patient with pre-existing cardiac disease is immediately life-threatening.
3. Delirium with vivid hallucinations: The patient is globally confused with marked disorientation (time, place, person). The hallucinations of DT are characteristically visual — often vivid, complex, and often featuring small moving animals (insects, rats, snakes — zooptic hallucinations) or persons. Tactile hallucinations (formication — insects crawling on the skin) accompany visual hallucinations in many cases. Auditory hallucinations are less prominent than in alcoholic hallucinosis. The patient is typically terrified by the hallucinations, which drives the agitated behaviour.
The Wernicke-Korsakoff spectrum represents a critically important complication that arises from a separate but temporally linked mechanism — thiamine (Vitamin B1) deficiency, which is essentially universal in chronic heavy drinkers because alcohol impairs thiamine absorption, utilisation, and storage, while simultaneously reducing dietary intake.
Wernicke's encephalopathy is the acute phase, characterised by the classical triad: (1) confusion and global encephalopathy (which may be indistinguishable clinically from DT without careful examination), (2) ophthalmoplegia (classically lateral rectus palsy producing horizontal nystagmus and diplopia, or complete gaze palsy), and (3) ataxia (cerebellar and vestibular — the patient staggers or cannot stand). Not all three features need be present — partial presentations are common and are equally a medical emergency.
The critical intervention is thiamine administration BEFORE any glucose infusion. The biochemical basis is essential to understand: thiamine is a coenzyme for several critical metabolic enzymes in glucose metabolism (pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase, transketolase). In a thiamine-deficient patient, administering glucose without prior thiamine rapidly depletes the remaining thiamine stores as glucose metabolism demands more of the enzyme, precipitating or catastrophically worsening Wernicke's encephalopathy. The rule is absolute: thiamine first, then glucose. In a confused, potentially thiamine-deficient patient, give thiamine (100 mg IV) before the dextrose infusion.
Korsakoff syndrome (Korsakoff psychosis) is the chronic neuropsychiatric sequela of inadequately treated or repeated Wernicke's encephalopathy. The mammillary bodies and medial thalamic nuclei, which are selectively vulnerable to thiamine deficiency, are permanently damaged. The clinical syndrome is dominated by profound anterograde amnesia (inability to form new memories — the patient cannot remember events from one moment to the next) and retrograde amnesia (inability to recall past events, with a temporal gradient), accompanied by the characteristic phenomenon of confabulation — the unconscious fabrication of plausible memories to fill the gaps, without any intent to deceive. Patients with Korsakoff syndrome appear superficially alert and can hold a conversation, but demonstrate profound disorientation in time when tested. The syndrome is largely irreversible once established.
Provided image
SELF-CHECK
A 48-year-old man with DT is brought to the emergency department confused and ataxic. The nurse prepares a 5% dextrose infusion and thiamine 100 mg IV. In what order should these be administered?
A. Dextrose first, then thiamine — the hypoglycaemia is the immediate danger
B. Thiamine first, then dextrose — glucose before thiamine precipitates Wernicke's encephalopathy
C. They can be given simultaneously through the same IV line
D. Thiamine first only if ophthalmoplegia is present; otherwise dextrose first
Reveal Answer
Answer: B. Thiamine first, then dextrose — glucose before thiamine precipitates Wernicke's encephalopathy
Thiamine MUST be given before glucose in any patient who is thiamine-deficient or suspected to be so (all chronic heavy drinkers qualify). Administering glucose first depletes the remaining thiamine stores by driving glucose metabolism through thiamine-dependent enzymes (pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase), precipitating or catastrophically worsening Wernicke's encephalopathy. This rule is absolute — it does not depend on whether ophthalmoplegia is already present. Give thiamine 100 mg IV (or IM), then the glucose infusion.