Page 8 of 16
FM11.5 | Delirium Tremens — SDL Guide (Part 2)
Clinical Assessment and Management Principles
The forensic physician encountering a prisoner or patient with suspected alcohol withdrawal must perform a structured clinical assessment that serves both immediate clinical and later medicolegal documentation purposes. The same record that guides treatment will be scrutinised at an inquest if the patient dies.
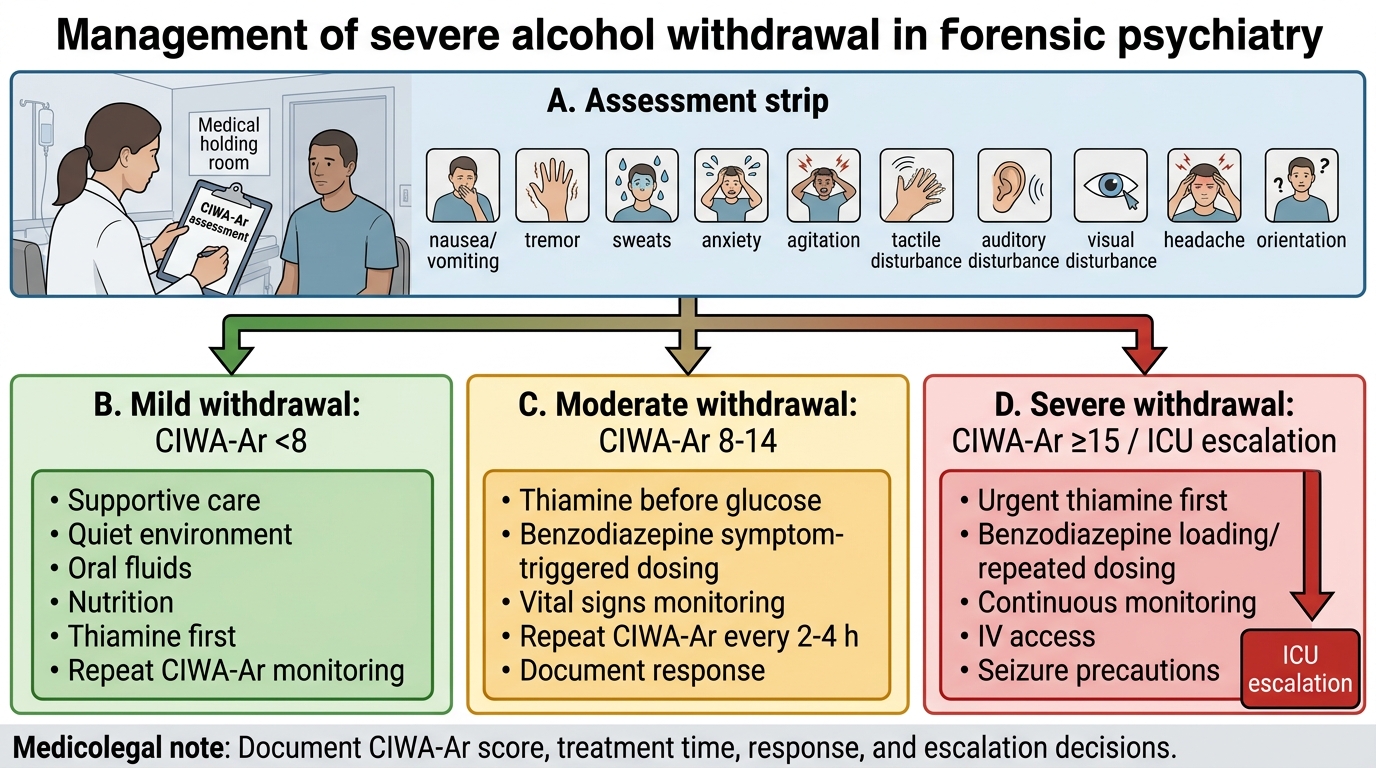
Clinical assessment tools: The Clinical Institute Withdrawal Assessment for Alcohol — Revised (CIWA-Ar) is the validated scale for quantifying withdrawal severity. It assesses ten domains: nausea/vomiting, tremor, paroxysmal sweats, anxiety, agitation, tactile disturbances, auditory disturbances, visual disturbances, headache, and orientation. Scores are summed: a CIWA-Ar score of ≥15 indicates severe withdrawal requiring pharmacological intervention. Scores 8-14 represent moderate withdrawal; scores <8 are mild. Documenting CIWA-Ar scores in the clinical record is both best practice and medico-legally protective — it demonstrates that the severity was formally assessed.
Pharmacological management — first line: benzodiazepines. Long-acting benzodiazepines (diazepam, chlordiazepoxide) are the first-line pharmacological treatment for alcohol withdrawal. They act on GABA-A receptors — the same receptors whose downregulation drives the hyperexcitability — and reduce the risk of seizures and DT progression. The dosing is titrated to the CIWA-Ar score. Lorazepam is preferred in patients with significant hepatic impairment because it does not require hepatic metabolism.
Thiamine supplementation: All patients with suspected chronic alcohol use should receive parenteral thiamine (100 mg IV or IM) as an immediate priority, before any glucose administration. High-dose thiamine (Pabrinex — thiamine 500 mg IV three times daily) is used when Wernicke's encephalopathy is suspected.
Monitoring and escalation: Continuous monitoring of vital signs (temperature, heart rate, blood pressure, oxygen saturation) is mandatory in suspected DT. Hyperthermia, cardiac arrhythmia, hypoxia, seizures refractory to benzodiazepines, or haemodynamic compromise — any of these require immediate ICU escalation.
Documentation for medicolegal purposes: Every clinical contact must record: time, vital signs, mental status (specifically CIWA-Ar score if available), the presence or absence of withdrawal features, the thiamine administration (time, dose, route), and the plan. Vague or absent notes in a patient who subsequently dies will be critically scrutinised at an inquest. The standard is: would this note allow a court to determine that the medical officer performed a clinically appropriate and timely assessment?
CIWA-Ar Based Management of Alcohol Withdrawal
CLINICAL PEARL
Four rules that determine the outcome in a DT case:
- Thiamine before glucose — no exceptions. In any confused, malnourished, or chronic-alcohol-use patient, give thiamine before dextrose. The COST of giving thiamine unnecessarily is zero. The COST of giving glucose first to a Wernicke's patient is permanent, irreversible amnestic disorder. When in doubt, give the thiamine.
- DT is withdrawal, not intoxication — the opposite direction. Detaining authorities and non-specialist staff commonly mistake the agitation and confusion of developing DT for continued intoxication and leave the patient without assessment. The forensic physician must communicate this: the drunk patient is sedated; the withdrawing patient is hyperexcitable, agitated, and progressively deteriorating. Early tremor + tachycardia + diaphoresis = call for medical assessment immediately.
- Kindling means each withdrawal is potentially worse. The clinical history of prior withdrawal episodes is prognostically critical — a patient with three prior DT episodes is at high risk of a severe, complicated withdrawal even if the initial presentation seems mild.
- Korsakoff syndrome is preventable, not treatable. Once the mammillary bodies and thalamic nuclei are permanently damaged by thiamine deficiency, the profound amnesia of Korsakoff syndrome is largely irreversible. Prevention is the only strategy: thiamine supplementation in every chronic drinker before and during any withdrawal episode.
Forensic Significance of Delirium Tremens
The forensic implications of DT are extensive and operate at the intersection of clinical medicine, criminal law, and state accountability for detainee welfare.
Post-mortem findings in DT deaths: When DT causes death, the post-mortem examination typically reveals non-specific findings that must be contextualised by the clinical history: pulmonary oedema, cerebral oedema, petechial haemorrhages, and signs of hyperthermia. There are no pathognomonic post-mortem findings for DT itself. The diagnosis is therefore primarily biochemical and circumstantial: blood and urine alcohol levels (which may be zero or low by the time of death — confirming cessation, not intoxication), elevated liver enzymes and macrocytosis on haematology (evidence of chronic alcoholism), and the exclusion of other organic causes of death (intracranial haemorrhage, myocardial infarction, sepsis). The medicolegal diagnosis of death due to DT requires the forensic pathologist to integrate clinical history (witnessed withdrawal syndrome), timeline (appropriate latency from last drink), ante-mortem records (documented withdrawal features), and the exclusion of other causes.
State duty of care and criminal negligence: The Indian Constitution's Article 21 and the Supreme Court's jurisprudence under DK Basu v State of West Bengal establish that detainees have a constitutional right to medical care. Failure to assess a detainee for alcohol withdrawal symptoms and failure to provide timely treatment can constitute gross negligence. Under BNS Section 106 (formerly IPC Section 304A — negligent act causing death), a medical officer who was called, assessed, and failed to initiate treatment for obvious DT signs may face criminal negligence charges. The forensic physician conducting the inquest post-mortem must document: when the prisoner was last seen alive and his condition, whether medical assessment was performed and when, whether appropriate treatment was initiated, and whether the death was preventable.
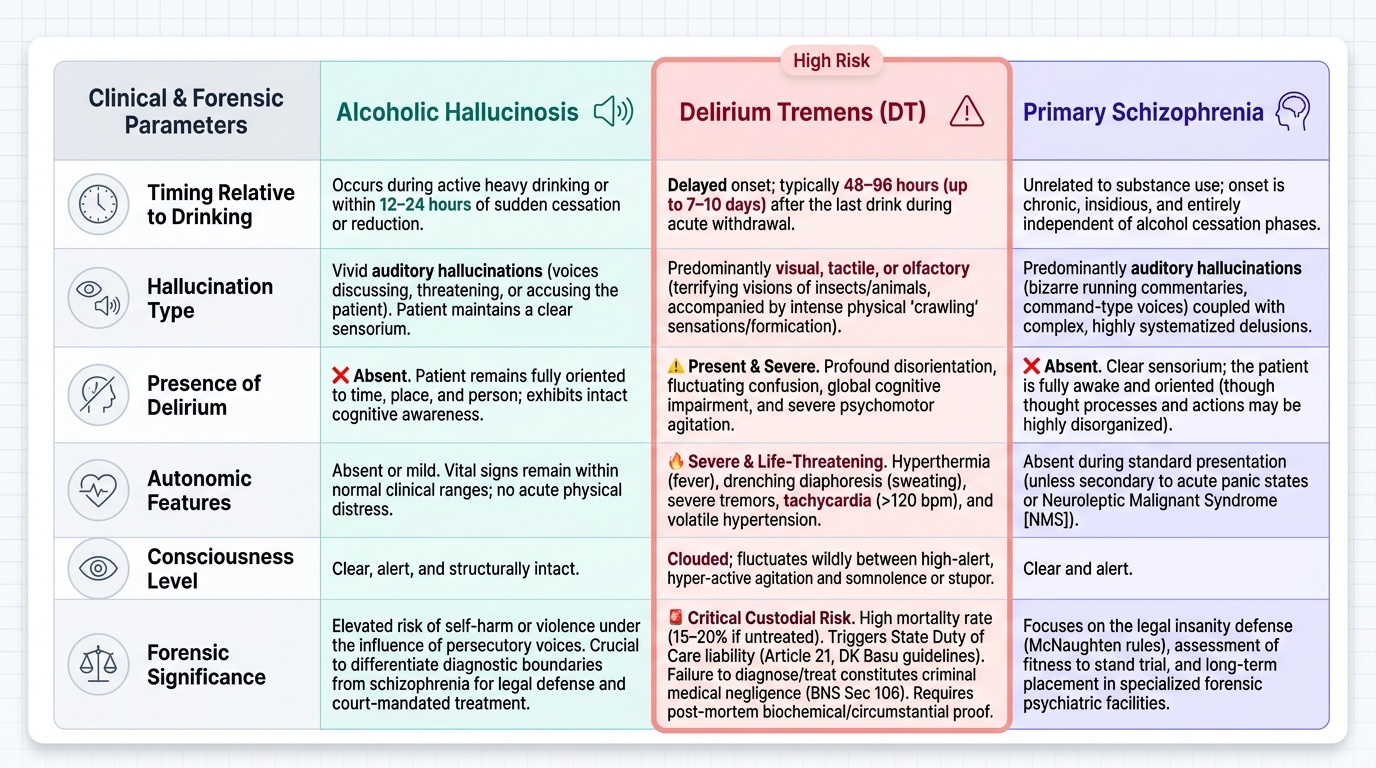
DT-induced psychosis vs primary psychotic disorder — the criminal responsibility distinction: When a person in DT commits a violent act — attacks a guard, injures another prisoner — the question of criminal responsibility arises. DT produces genuine psychotic symptoms (vivid visual hallucinations, terrifying delusions during the delirious state). However, the critical legal question under BNS Section 22 is whether the accused knew the nature of the act or its wrongness. Additionally, the intoxication was VOLUNTARY — the patient chose to drink chronically. Courts have generally held that criminal incapacity arising from voluntary intoxication is not a complete McNaughten defence (consistent with the rule discussed in SDL fpsy2). The distinction from a primary psychotic disorder is that DT is substance-induced, time-limited, and directly caused by voluntary behaviour, whereas primary schizophrenia is an endogenous mental illness with no voluntary component.
Alcoholic hallucinosis must be distinguished from DT: in alcoholic hallucinosis, vivid auditory hallucinations (typically accusatory voices) occur in a clear (not delirious) state, often during continued drinking or early withdrawal. There is no delirium, no autonomic storm. Alcoholic hallucinosis may persist for weeks and can develop into a chronic state resembling schizophrenia. The forensic physician must distinguish alcoholic hallucinosis from DT (different timing, different features) and from schizophrenia (history of chronic alcohol use, relationship to drinking pattern, absence of formal thought disorder).
Mental Healthcare Act 2017 (MHA 2017) and substance use: Under MHA 2017 Section 2(s), substance use disorders that produce substantial disorder of thinking, mood, or perception qualify as mental illness under the Act. Persons with severe alcohol use disorder may be admitted to a mental health establishment under the MHA 2017 provisions — voluntary (self-admission), supported (with the help of a nominated representative), or involuntary admission (by magistrate order, for persons posing a danger to themselves or others) — instead of merely being detained in a lock-up. The forensic physician must be familiar with these admission pathways as an alternative to punitive detention, which creates DT risk.
Provided image
SELF-CHECK
At a post-mortem examination of a 52-year-old man who died in police custody 60 hours after arrest, you find pulmonary oedema, cerebral oedema, and no other obvious cause of death. Blood alcohol level is zero. The police report states he was 'very loud and shaky' for the first night and was 'given paracetamol' but no further medical review was requested. What is your most likely medico-legal conclusion?
A. Natural death due to cardiac disease — pulmonary oedema is common in cardiac deaths
B. Death likely due to Delirium Tremens (severe alcohol withdrawal syndrome) — zero BAL confirms cessation state; symptoms and timeline are consistent; medical care was inadequate
C. Accidental death from fall — bruises explain the death
D. The death cannot be attributed to DT without finding a raised blood alcohol level
Reveal Answer
Answer: B. Death likely due to Delirium Tremens (severe alcohol withdrawal syndrome) — zero BAL confirms cessation state; symptoms and timeline are consistent; medical care was inadequate
The zero blood alcohol level is consistent with DT — DT is a WITHDRAWAL state, occurring 48-96 hours after the last drink, when alcohol has been fully metabolised. A raised BAL would actually argue AGAINST DT. The timeline (60 hours in custody), the witnessed features ('loud and shaky'), the non-specific post-mortem findings (pulmonary and cerebral oedema — typical of hyperthermia and cardiovascular collapse in DT), and the absence of other organic causes collectively support a conclusion of death from severe alcohol withdrawal (DT). The inadequate medical response ('paracetamol' without proper assessment) is a significant medicolegal finding regarding the duty of care.