Page 10 of 16
FM11.6 | Mental Healthcare Act 2017 — SDL Guide
Learning Objectives
- Describe the key provisions of the Mental Healthcare Act 2017 relating to rights, admission, care, and discharge of persons with mental illness
- Explain the Advance Directive and Nominated Representative provisions under MHA 2017
- Describe the treatment prohibitions under MHA 2017, including those relating to ECT
- Explain Section 115 MHA 2017 and its forensic significance for attempted suicide cases
- Identify the forensic physician's obligations under MHA 2017 in clinical and medicolegal practice
INSTRUCTIONS
The Mental Healthcare Act 2017 represents one of the most significant legal reforms in Indian psychiatry and forensic medicine in the past three decades. It replaced the Mental Health Act 1987 — a colonial-era framework that emphasised custody and control — with a modern, rights-based statute that treats persons with mental illness as rights-bearing citizens entitled to dignity, autonomy, and appropriate care. For the forensic physician, this Act is not optional background reading: it governs how psychiatric patients may be admitted, treated, and discharged; it defines the rights patients can invoke against their treating institutions; and it contains the landmark Section 115 that decriminalised attempt to suicide. Ignorance of this Act is a clinical and medicolegal liability.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman with a five-year history of paranoid schizophrenia is brought to a government mental health establishment by her husband. She is acutely psychotic, convinced that her neighbours are poisoning her food, refusing all oral medication, and has not eaten for three days. Her husband wants her admitted and treated urgently. The woman, however, insists she is not ill and refuses admission. She had previously made an Advance Directive, registered with the District Mental Health Authority, stating she consents to medication but refuses ECT under any circumstances. The treating team is considering involuntary admission and, if necessary, ECT to break the acute psychotic episode. Which provisions of the Mental Healthcare Act 2017 govern this scenario, and how do they constrain and guide every decision the treating team makes?
WHY THIS MATTERS
Every forensic physician will encounter situations governed by the Mental Healthcare Act 2017: a family brings a suicidal patient who refuses treatment; a Magistrate orders a psychiatric examination; a prisoner with chronic schizophrenia needs certification for a court hearing; a death occurs in a psychiatric establishment and you are called to investigate. In each of these scenarios, your obligations — and the rights of the patient — are defined by MHA 2017. Knowing this Act is the difference between acting lawfully and inadvertently violating the statutory rights of a patient, which can result in personal professional liability. It is also the difference between providing a court report that withstands legal scrutiny and one that is challenged on procedural grounds.
RECALL
From earlier modules, recall that the Mental Health Act 1987 was the preceding statute — it is now fully repealed and replaced by MHA 2017. Any reference to the 1987 Act in a contemporary clinical or medicolegal document is an error. Recall also from SDL fpsy1 that the MHA 2017 defines "mental illness" under Section 2(s) as a substantial disorder of thinking, mood, perception, orientation, or memory that grossly impairs judgment, behaviour, capacity to recognise reality, or ability to meet ordinary demands of life. This definition is deliberately broad and human-rights-aligned — it explicitly states that mental illness shall NOT be determined merely on the basis of non-conformity with political, cultural, religious, or social values.
A Court-Ordered Admission: The MHA 2017 in Practice
The scenario at the opening of this module captures a practical forensic dilemma that recurs in clinical practice: a person with established mental illness is acutely unwell, is refusing treatment, and has previously exercised their right to make decisions about their own care through an Advance Directive. The treating team — under pressure from the family and mindful of the clinical urgency — must navigate this situation entirely within the statutory framework of the Mental Healthcare Act 2017. Every step they take must be legally justifiable under the Act's provisions.
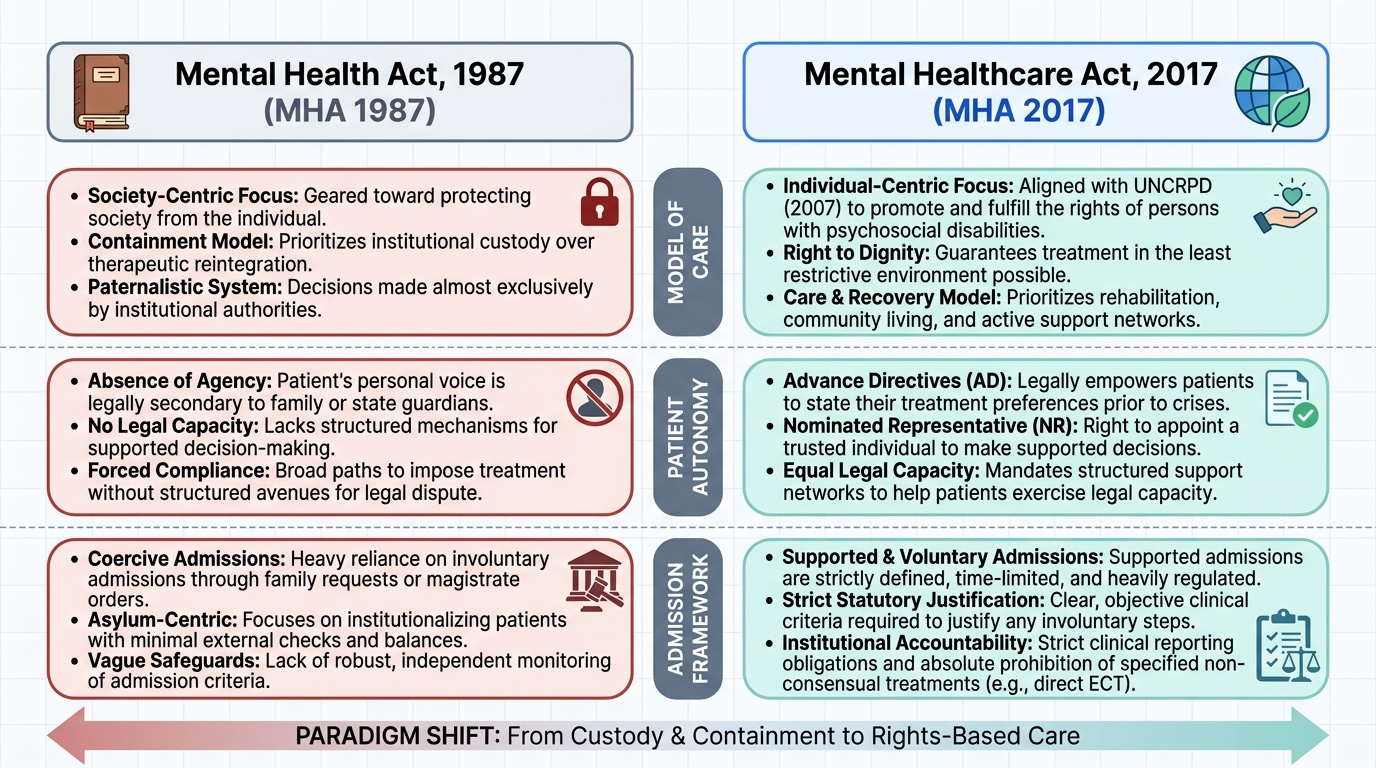
The MHA 2017 was enacted after India ratified the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) in 2007, which obligates states to ensure that persons with disabilities — including psychosocial disabilities (mental illness) — enjoy legal capacity on an equal basis with others and have access to appropriate support in exercising that capacity. The Act's rights-based philosophy flows directly from this international commitment. The central shift from the 1987 Act is from a model of custody and containment (which focused on protecting society from persons with mental illness) to a model of care, rights, and dignity (which focuses on protecting the rights of persons with mental illness and ensuring they receive appropriate treatment in the least restrictive environment).
For the forensic physician, the MHA 2017 creates obligations at three levels:
- Clinical obligations: compliance with treatment standards, consent requirements, and prohibited treatments when providing or certifying psychiatric care.
- Reporting obligations: notifying the relevant authority (DMHA or CMHA) of specified events occurring in mental health establishments (deaths, escapes, sexual assaults, improper use of physical restraint).
- Expert witness obligations: providing court-admissible opinions that accurately apply the MHA 2017 framework — including the definition of mental illness, the admission procedures, and the right-to-treatment provisions.
Provided image
Rights of Persons with Mental Illness under MHA 2017
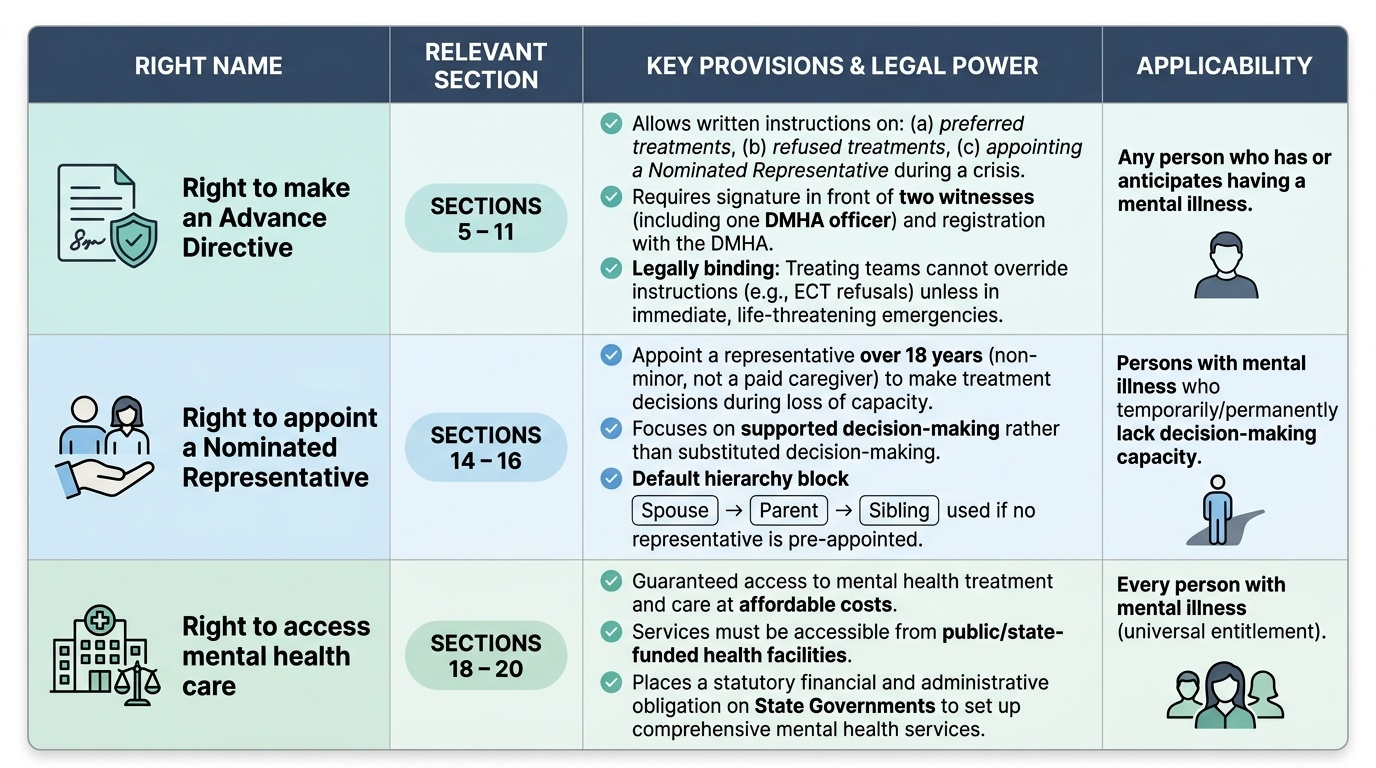
The MHA 2017 establishes an extensive catalogue of rights for persons with mental illness that have no precedent in the earlier 1987 Act. Understanding these rights is essential for the forensic physician because they represent enforceable entitlements — their violation can be challenged before the Mental Health Review Board or the courts. The key rights are as follows:
1. Right to make an Advance Directive (Sections 5-11): Any person who has or anticipates having a mental illness may make a written Advance Directive specifying: (a) how they wish to be treated during a mental health crisis, (b) how they do NOT wish to be treated, and (c) who they appoint as their Nominated Representative. The Advance Directive must be signed in the presence of two witnesses, one of whom must be a District Mental Health Authority (DMHA) officer, and must be registered with the DMHA to be legally enforceable. Once registered, the Advance Directive is binding on treating clinicians — they CANNOT administer a treatment that the patient's Advance Directive has refused, except in the case of immediate life-threatening emergency. In the hook scenario, the woman's Advance Directive refusing ECT is enforceable and legally binding: the treating team cannot administer ECT simply because the family consents.
2. Right to appoint a Nominated Representative (Sections 14-16): The person with mental illness may appoint a Nominated Representative (NR) — a person over 18 years who is not a minor and not involved in providing paid care — to take treatment decisions on their behalf when they lack capacity to do so. The NR is a specific legal role under MHA 2017 and carries specific responsibilities. In the absence of an NR designated by the patient, the Act specifies a default hierarchy: the spouse (if the marriage is not contested), a parent, a sibling (in that order). The NR's role is to support the patient's decision-making, not to substitute their own judgment — the Act emphasises supported decision-making, not substituted decision-making.
3. Right to access mental health care (Sections 18-20): Every person with mental illness has the right to access mental health care and treatment at affordable costs, including from public health facilities. State governments are obligated to provide mental health services. This right is enforceable and has been used in public interest litigation to compel state governments to fund mental health infrastructure.
4. Right to equality in treatment (Section 21): Persons with mental illness have the right to the same standard of emergency care as any other person with a physical health emergency — mental illness does not justify a lower standard of emergency care.
5. Right to protection from cruel, inhumane, or degrading treatment (Section 21(2)): This includes the right to live in the community (not to be institutionalised unnecessarily), the right to non-discrimination, and specific protections including freedom from physical restraint except in specified emergencies.
6. Right to confidentiality (Section 23): Information shared by a person with mental illness in the course of treatment must be kept confidential except in specific circumstances (risk to self or others, court order, public safety).
Provided image
SELF-CHECK
A 35-year-old man with bipolar disorder made a valid Advance Directive registered with the DMHA two years ago, in which he specified that he consents to lithium and antipsychotics but refuses ECT. During an acute manic episode, his wife (acting as his Nominated Representative) requests ECT to accelerate recovery. The treating psychiatrist agrees it is clinically indicated. Under MHA 2017, can ECT be administered over the patient's Advance Directive?
A. Yes — the Nominated Representative's consent overrides the Advance Directive
B. Yes — clinical necessity overrides a prior Advance Directive during acute episodes
C. No — a valid registered Advance Directive refusing ECT is binding; it cannot be overridden by the NR or treating team except in immediate life-threatening emergencies
D. No — ECT is always prohibited under MHA 2017 regardless of consent
Reveal Answer
Answer: C. No — a valid registered Advance Directive refusing ECT is binding; it cannot be overridden by the NR or treating team except in immediate life-threatening emergencies
Under MHA 2017 Sections 5-11, a valid, registered Advance Directive is legally binding. The treating team cannot administer a treatment explicitly refused in the Advance Directive, even if the Nominated Representative consents. The NR's role is to support the patient's expressed wishes (including those in the Advance Directive), not to override them. The only exception is an immediate life-threatening emergency where the treatment refused is the only available intervention. ECT is not categorically banned by MHA 2017 — modified ECT with proper consent IS permitted; it is unmodified ECT and ECT on minors that are prohibited.
Admission, Care, and Discharge — Types and Procedures
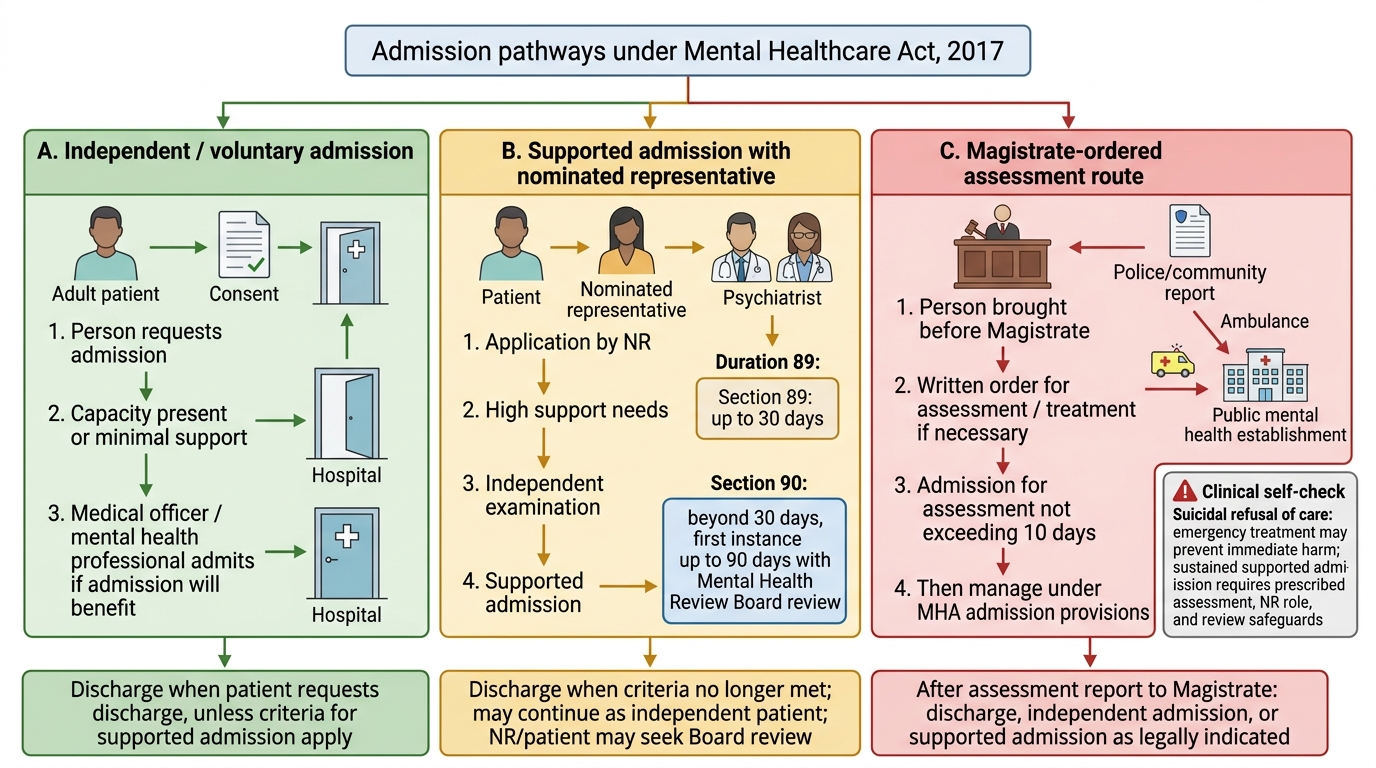
The MHA 2017 establishes a tiered admission framework that ranges from fully voluntary admission to magistrate-ordered involuntary admission. The framework is designed to ensure that the least restrictive option is always tried first and that involuntary admission is used only when genuinely necessary and with appropriate safeguards. Every admission to a registered Mental Health Establishment (MHE) must follow one of the specified procedures — informal admission of a person with mental illness without following the Act's procedures is itself a violation of the Act.
1. Independent (Voluntary) Admission (Section 86): Any person who considers themselves to have a mental illness may apply in writing to an MHE for admission as an independent patient. The MHE can admit them if the treating psychiatrist or medical officer certifies that admission is necessary for treatment. The person retains full autonomy — they can leave at any time by giving a written request for discharge. For persons who express a wish for admission but may lack full capacity, supported admission under the NR framework applies.
2. Supported Admission (Sections 88-90): When a person with mental illness either cannot make an independent application or expresses a wish for treatment with the support of their NR, the NR may make an application for supported admission. The NR's application must be supported by a medical certificate from a registered medical practitioner (not necessarily a psychiatrist). The person must not object to the admission — if they object, only the involuntary procedure can proceed.
3. Involuntary Admission (Sections 88-100 read together): When a person with mental illness is posing an imminent risk of harm to themselves or others, and refuses admission, involuntary admission may be initiated. The procedure requires: (a) an application by a relative, nominated representative, or a mental health professional; (b) examination by two psychiatrists who both certify that the admission is necessary; and (c) approval by the Magistrate for any admission beyond the initial emergency period. Initial involuntary admission is for 30 days, after which it must be reviewed. Extension beyond 30 days requires a further order from the Mental Health Review Board.
Discharge provisions: Discharge must occur when the patient no longer meets the criteria for admission (i.e., does not require inpatient treatment) or when the patient (for voluntary admission) requests it. The MHE cannot retain a voluntary patient against their will. For involuntary patients, discharge is by the treating psychiatrist or by the Mental Health Review Board.
Mental Health Review Board (MHRB): Each state must constitute MHRBs — quasi-judicial bodies that review involuntary admissions, hear appeals from patients, and adjudicate disputes about Advance Directives and treatment decisions. The MHRB includes a District Judge or advocate, a psychiatrist, and a person with psychosocial disability or a carer.
Admission Pathways Under MHA 2017
SELF-CHECK
A family member brings a 42-year-old woman with severe depression who is acutely suicidal and refusing all treatment. The family member requests involuntary admission. Under MHA 2017, what is the MINIMUM procedural requirement before she can be admitted involuntarily?
A. The treating psychiatrist's clinical judgment alone is sufficient for emergency involuntary admission
B. Examination by two psychiatrists certifying necessity, followed by Magistrate approval for admission beyond the emergency period
C. The family member's signed application is sufficient
D. A police report is required before any involuntary psychiatric admission
Reveal Answer
Answer: B. Examination by two psychiatrists certifying necessity, followed by Magistrate approval for admission beyond the emergency period
Under MHA 2017, involuntary admission requires: (1) an application by a relative, NR, or mental health professional; (2) examination by two psychiatrists, both of whom must certify that admission is necessary; and (3) Magistrate approval for continued involuntary admission beyond the initial emergency period (initial emergency observation is permitted, but sustained involuntary admission requires the judicial process). A single psychiatrist's opinion, a family member's application alone, or a police report are not sufficient. The two-psychiatrist certification requirement is a safeguard against arbitrary deprivation of liberty.