Page 11 of 16
FM11.6 | Mental Healthcare Act 2017 — SDL Guide (Part 2)
Treatment Standards and Prohibitions
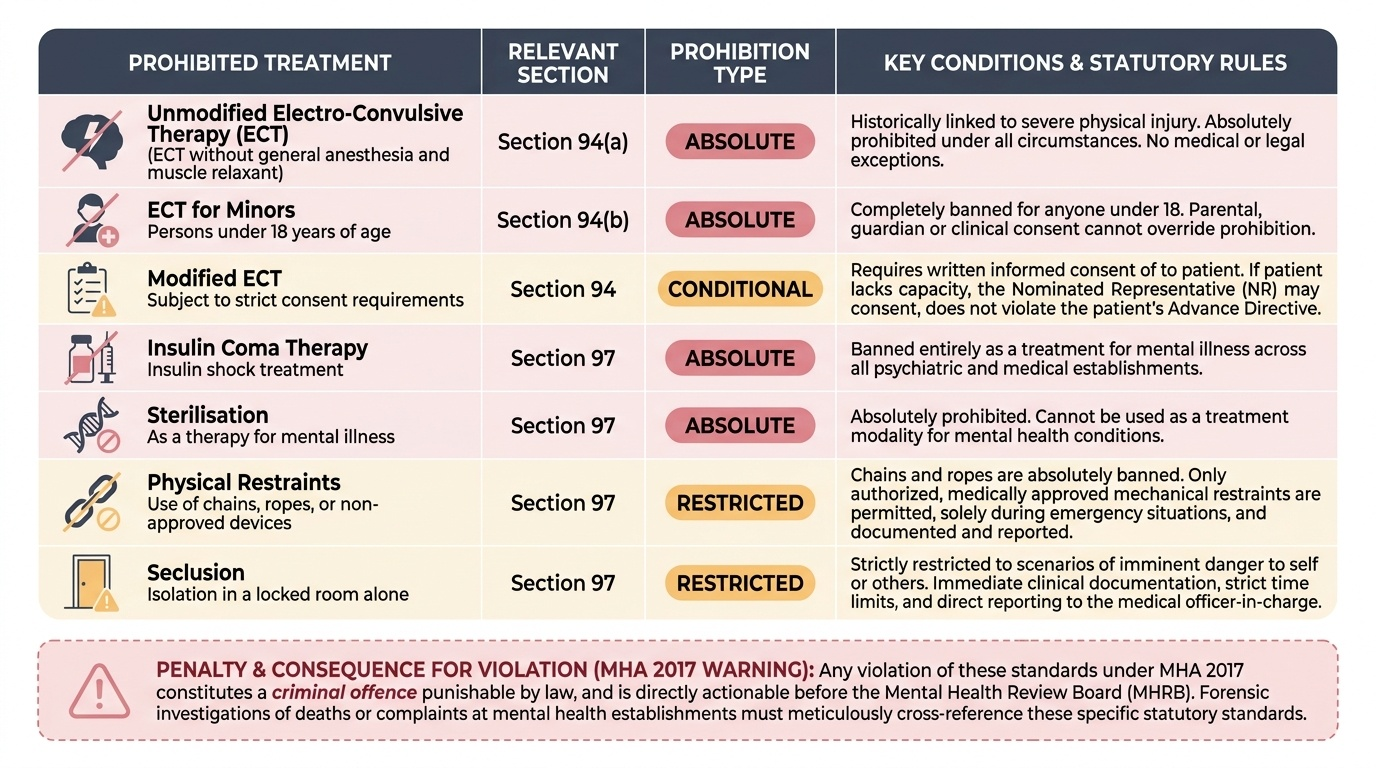
The MHA 2017 imposes specific standards and absolute prohibitions on treatment — going beyond the general requirement for informed consent to mandate specific protocols for certain high-risk or historically abused treatments. The forensic physician called to investigate a complaint or a death at a mental health establishment must know these standards precisely, because violations are both criminal offences under the Act and actionable before the MHRB.
Electro-Convulsive Therapy (ECT) — MHA 2017 Section 94:
The MHA 2017 permits modified ECT — ECT administered under general anaesthesia with muscle relaxant — as a legitimate and approved treatment for specific conditions, subject to strict consent requirements. However, it prohibits the following:
- Unmodified ECT (ECT without general anaesthesia and without muscle relaxant) is absolutely prohibited under Section 94(a). This form of ECT was historically common in India and was associated with significant physical injury (spinal fractures from unmodified convulsions, respiratory complications). The prohibition is absolute — there is no exception.
- ECT for minors (persons under 18 years) is absolutely prohibited under Section 94(b), with no exceptions, regardless of clinical indication or parental consent.
- ECT without informed consent: Modified ECT may be administered only with the written informed consent of the patient. If the patient lacks capacity to consent, the Nominated Representative's consent is required, AND only if the Advance Directive does not specifically refuse ECT. ECT cannot be administered over a patient's valid Advance Directive refusal.
Other prohibited treatments (Section 97):
- Insulin coma therapy (insulin shock treatment) is absolutely prohibited.
- Sterilisation as a treatment for mental illness is prohibited.
- Physical restraints (chains, ropes) are prohibited; only specifically approved mechanical restraints may be used in defined emergency situations, subject to documentation and reporting requirements.
- Seclusion (confinement in a room alone) is restricted to situations of imminent danger and requires documentation, a time limit, and reporting to the medical officer in charge.
Medication without consent: In general, medication requires the patient's informed consent. In emergency situations where the patient lacks capacity and there is immediate risk, the NR's consent or the treating physician's clinical judgment (with documentation) may authorise emergency medication. However, this is a narrow exception — routine administration of medication without consent or over a competent patient's explicit refusal is a violation of MHA 2017 rights.
Maintenance of dignity in treatment: Section 20 mandates that all persons in a mental health establishment must be treated with dignity — physical conditions (hygiene, nutrition, clothing), communication, and privacy must all meet specified standards. The forensic physician inspecting an MHE or investigating a complaint must assess these standards against the Act's requirements.
Provided image
Section 115 and Decriminalisation of Attempt to Suicide
Section 115 of the Mental Healthcare Act 2017 is one of the most important legislative provisions in Indian forensic medicine and public health law, and its implications must be clearly understood by every forensic physician.
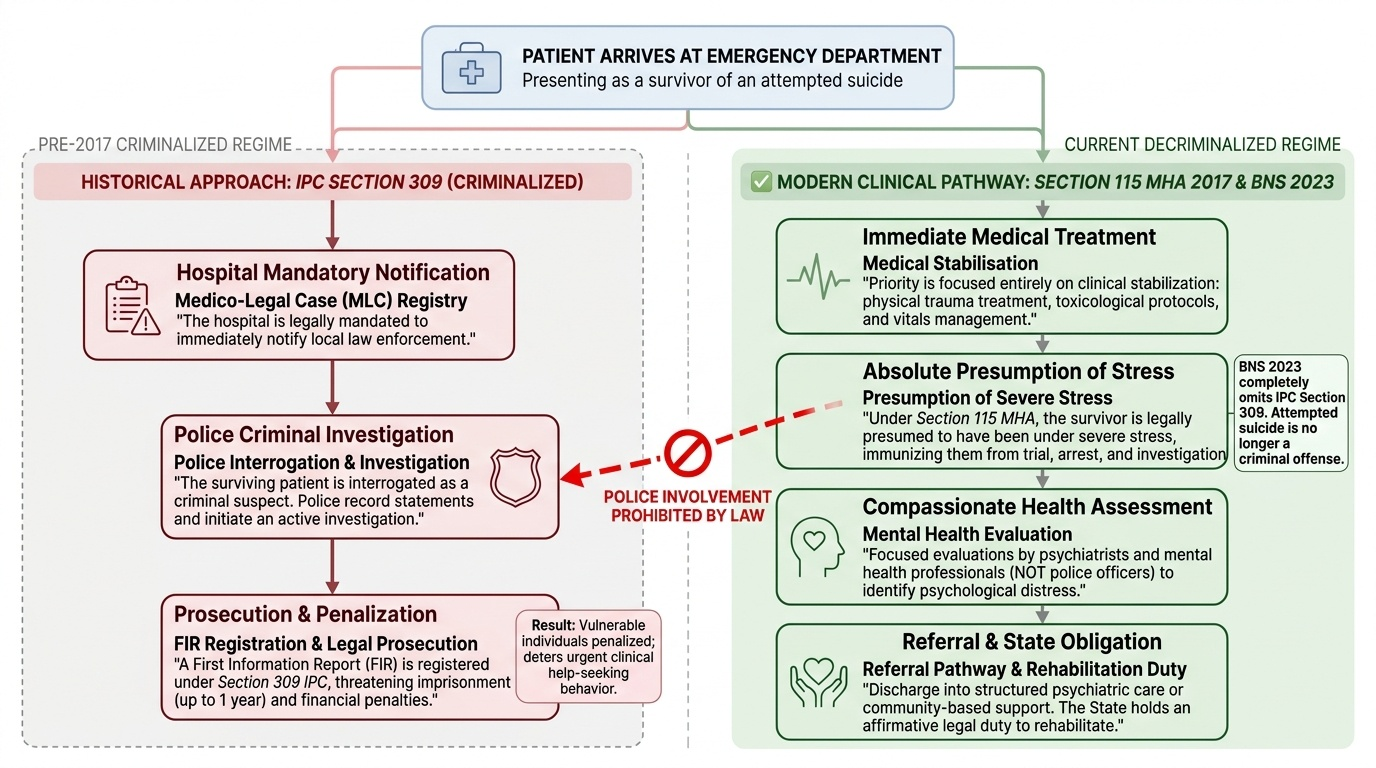
The provision reads: "Notwithstanding anything contained in section 309 of the Indian Penal Code, any person who attempts to commit suicide shall be presumed, unless proved otherwise, to have severe stress and shall not be tried and punished under the said Code."
What this means: A person who has attempted to commit suicide is legally presumed to have been acting under severe stress at the time of the attempt — not with criminal intent. This is a presumption in the person's favour that effectively decriminalises the act of attempting suicide. They cannot be arrested, charged, prosecuted, or punished for the attempt. The provision explicitly overrides the criminalisation that previously existed under IPC Section 309.
Historical context: IPC Section 309 criminalised attempted suicide — a person who attempted and survived could face imprisonment up to one year and/or a fine. This provision was widely criticised by the medical community and mental health advocates as counter-productive: it punished the most vulnerable people (those in mental health crises) and deterred help-seeking. The Law Commission of India (in its 210th report, 2008) recommended decriminalisation. Section 115 MHA 2017 gave effect to this recommendation.
The BNS and attempt to suicide: The Bharatiya Nyaya Sanhita 2023 has omitted the equivalent of IPC Section 309 entirely — attempt to commit suicide is not a criminal offence under BNS. This is consistent with and reinforces the MHA 2017 Section 115 framework. For cases after 01 July 2024, there is simply no criminal provision under which an attempted suicide can be prosecuted.
Forensic implications of Section 115:
- Police response to attempted suicide: Police who are called to a suicide attempt must NOT treat the surviving person as a criminal suspect, must NOT take them into custody as an accused, and MUST refer them to mental health services. Section 115 creates an affirmative duty on the government to rehabilitate persons who have attempted suicide, which includes access to mental health care.
- Documentation by the treating physician: When a person is brought in after a suicide attempt, the treating physician's notes should reflect assessment of mental state, severity of suicidal ideation, and the need for mental health referral — NOT a complaint or a police referral as if the person were a criminal.
- Limitations of Section 115: The provision applies to genuine suicide attempts, not to cases where a person feigns a suicide attempt for strategic purposes (e.g., to escape an adverse situation, to coerce a family member). The forensic physician may be asked to opine on the genuineness of a claimed suicide attempt — the same principles of malingering detection (SDL fpsy2) apply.
- Recent amendments: The Mental Healthcare (Amendment) Act 2024 (if enacted and notified) and associated rules under MHA 2017 continue to refine implementation details. Students should note that the MHA 2017 itself was only partially notified in some states, and the Central Mental Health Authority was constituted with some delay — in practice, implementation has been uneven across India.
Provided image
Mental Health Establishments, DMHA, and the Forensic Physician's Obligations
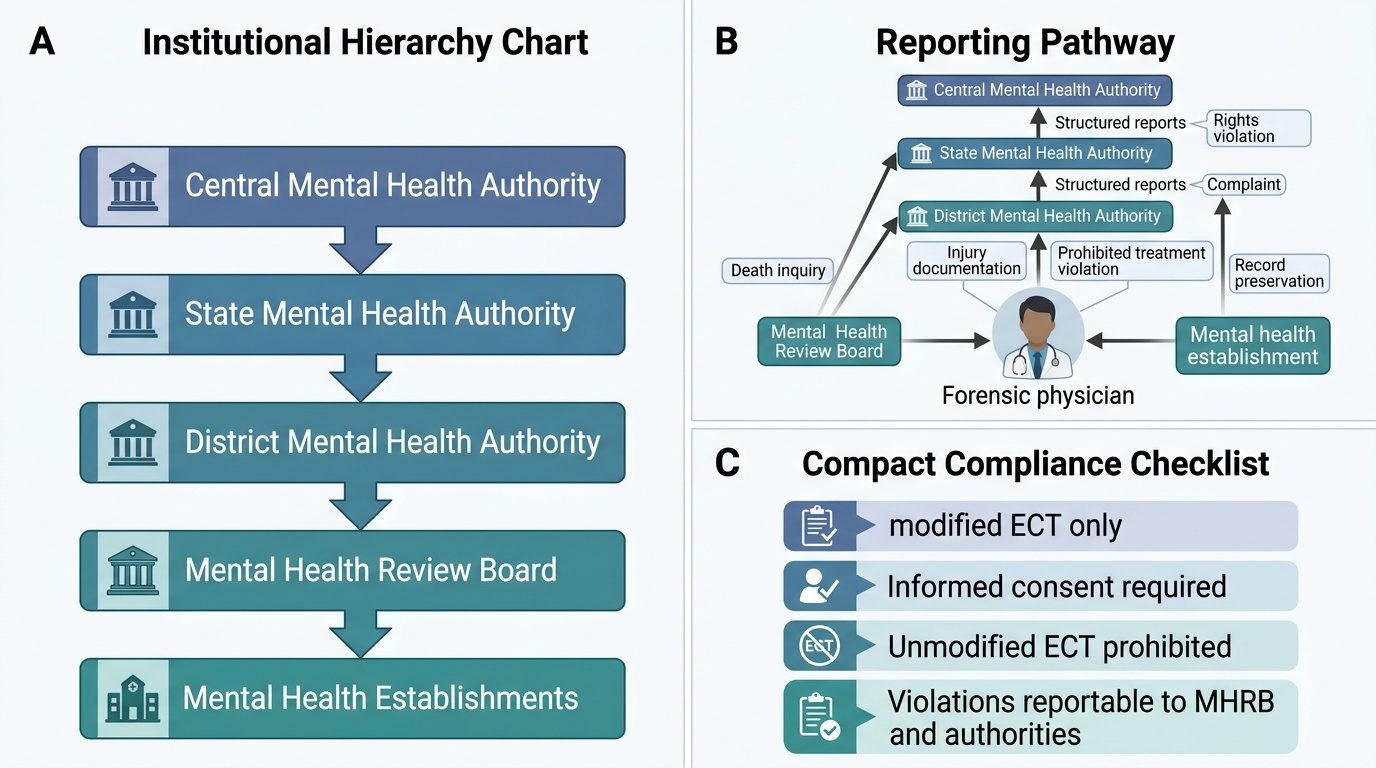
The MHA 2017 created a comprehensive institutional architecture — a network of authorities, review boards, and licensing requirements — that governs the operation of mental health services in India. The forensic physician operates within this architecture and must understand the reporting and compliance obligations it imposes.
Mental Health Establishment (MHE): Any health establishment that provides mental health services — including a general hospital with a psychiatric ward — must be registered as an MHE with the relevant state authority. Unregistered facilities providing psychiatric care violate the Act. Prisons and correctional facilities are also subject to MHA 2017 provisions for the mental health care of inmates.
Central Mental Health Authority (CMHA): The CMHA is constituted at the national level under Chapter VI of MHA 2017. Its functions include: maintaining a national register of MHEs, monitoring and reviewing the rights of persons with mental illness, developing programmes for mental health services, and advising the central government on policy.
District Mental Health Authority (DMHA): Each district has a DMHA responsible for: registering MHEs within the district, maintaining records of Advance Directives, constituting or supporting the Mental Health Review Board, conducting regular inspections of MHEs, and receiving and investigating complaints from persons with mental illness or their families.
Forensic physician's reporting obligations under MHA 2017:
- Deaths in MHEs: Every death occurring in a registered MHE must be reported to the DMHA. The forensic physician conducting the post-mortem on such a death must submit their report not only to the police but also to the DMHA for the authority's quality review and accountability functions.
- Sexual assault in MHEs: Instances of sexual assault on persons with mental illness within an MHE must be reported to the DMHA and the police. The MHE's clinical records must be preserved and made available for investigation.
- Improper use of physical restraints or seclusion: Cases where restraint or seclusion has been used in violation of the Act's standards must be reported. The forensic physician, if called as an expert witness in disciplinary or criminal proceedings arising from such violations, must assess the clinical justification and procedural compliance against the MHA 2017 standards.
- Prisons — special provisions (Section 103-105): The MHA 2017 contains specific provisions for mentally ill prisoners. The government must ensure that every prison has facilities for basic mental health assessment and care; prisoners with mental illness must be transferred to mental health establishments if inpatient psychiatric care is required; prison medical officers have specific obligations to assess and report on the mental health status of prisoners as required by the Magistrate.
National Mental Health Policy and NMHP: The National Mental Health Programme (NMHP) and the District Mental Health Programme (DMHP) are the policy and programme frameworks within which MHA 2017 is implemented at the district level. The forensic physician in a government posting will encounter NMHP structures — mental health teams at district hospitals, community mental health workers — and must coordinate with them in implementing the MHA 2017 framework.
MHA 2017 Institutional Architecture and Forensic Reporting
CLINICAL PEARL
Five MHA 2017 provisions that the forensic physician must be able to cite from memory:
- Advance Directive (Sections 5-11): Any person may specify their treatment preferences in a registered Advance Directive. It is binding. The treating team cannot override it except in immediate life-threatening emergencies.
- ECT prohibitions (Section 94): Unmodified ECT (without anaesthesia/muscle relaxant) is absolutely prohibited. ECT on minors (under 18) is absolutely prohibited. These are zero-exception rules.
- Section 115: A person who attempts suicide is presumed to have been under severe stress — NOT criminally liable. Police must refer, not arrest. Physicians must treat and refer to mental health services, not initiate criminal proceedings.
- Involuntary admission requires two psychiatrists + Magistrate: One psychiatrist alone cannot authorise sustained involuntary admission. This is the judicial safeguard against arbitrary deprivation of liberty.
- Mental Health Act 1987 is repealed: ANY citation of the 1987 Act in a current medicolegal document is an error. The operative statute is the Mental Healthcare Act 2017. This is the most common factual error in forensic psychiatry examinations.
SELF-CHECK
Under Section 115 of the Mental Healthcare Act 2017, when a person who has survived a suicide attempt is brought to the emergency department, what is the correct legal and clinical approach?
A. Notify the police immediately so they can file an FIR under IPC Section 309
B. Treat the person medically, then call the police — Section 309 IPC is still operative
C. Treat the person medically and refer for mental health assessment — the person is presumed to be under severe stress and cannot be prosecuted for the attempt
D. Detain the person in the hospital until a psychiatric board certifies they are not dangerous
Reveal Answer
Answer: C. Treat the person medically and refer for mental health assessment — the person is presumed to be under severe stress and cannot be prosecuted for the attempt
Section 115 MHA 2017 creates a legal presumption that a person who attempted suicide was under severe stress — they shall NOT be tried and punished under IPC Section 309. BNS (which replaced IPC from 01 July 2024) has omitted attempt-to-suicide as a criminal offence entirely. Therefore the police should NOT be called to file an FIR for attempted suicide; IPC Section 309 is not applicable under MHA 2017 (and BNS has removed the equivalent provision entirely). The correct approach is: medical stabilisation, mental health assessment, and referral to psychiatric care. The government has an affirmative duty to provide rehabilitation.