Page 2 of 20
FM6.1 | Firearms: Types, Ammunition & Terminology — SDL Guide (Part 2)
Mechanism of Firing and Ballistic Terminology
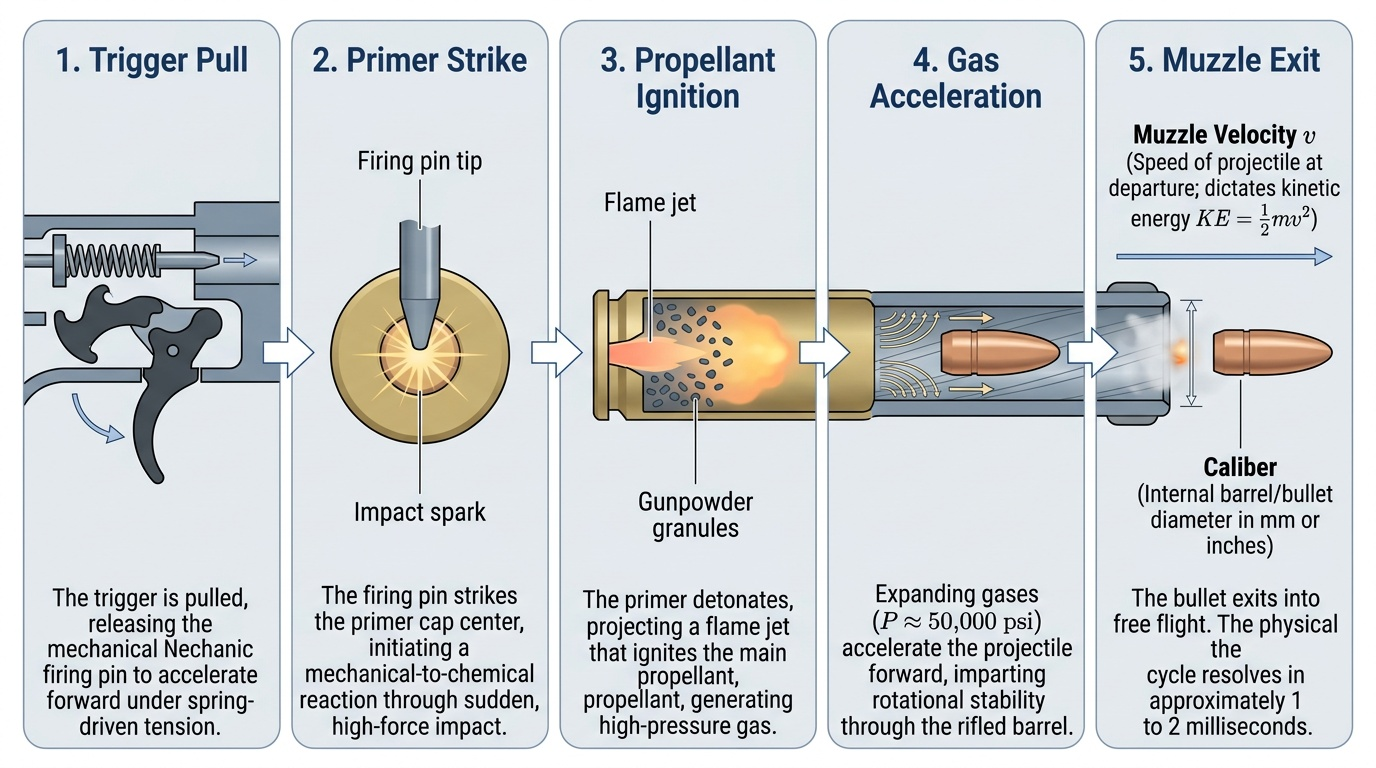
Understanding the sequence of events between trigger pull and bullet impact allows the forensic physician to reason from wound characteristics backwards to the circumstances of the shooting. The firing cycle begins when the trigger is pulled, releasing the firing pin or hammer to strike the primer. The primer detonates, sending a flame jet into the propellant charge, which ignites and generates a large volume of gas at extremely high pressure (up to 50,000 psi in a rifle). This gas propels the bullet from the cartridge case, down the barrel, and out the muzzle — the entire process taking approximately 1–2 milliseconds.
Provided image
Key ballistic terminology that appears in forensic reports and court testimony:
Caliber refers to the internal diameter of the barrel — and by extension, to the bullet diameter that fits it. Caliber is stated in either inches (e.g., .38, .45, .303) or millimetres (e.g., 9 mm, 7.62 mm). Caliber also designates the cartridge type: a .38 Special cartridge fires a bullet of .38-caliber. Note that caliber is not the same as power — a .22 rifle bullet may be far more lethal than a large-caliber pistol bullet because of its higher velocity.
Muzzle velocity is the speed of the bullet as it leaves the barrel, measured in metres per second (m/s) or feet per second (fps). Typical values: pistols 250–450 m/s; rifles 750–1000 m/s. Muzzle velocity is the primary determinant of tissue destruction, because kinetic energy scales with the square of velocity (KE = ½mv²).
Range in the forensic context means the distance between the muzzle and the target at the time of firing. This is the key parameter the forensic physician must estimate from wound characteristics. It is not the maximum range the weapon can fire. Range estimation is covered in the next module (FM6.2).
Trajectory is the path of the bullet from muzzle to target. An understanding of trajectory, combined with wound track direction at autopsy, allows reconstruction of the shooter's position relative to the victim.
Recoil is the backward force experienced by the shooter on firing. Recoil from large-caliber weapons produces characteristic powder burns on the thumb web of the shooting hand — the presence of these burns on a deceased person is significant evidence in determining whether the wound is self-inflicted.
Choking in Shotguns and Its Forensic Significance
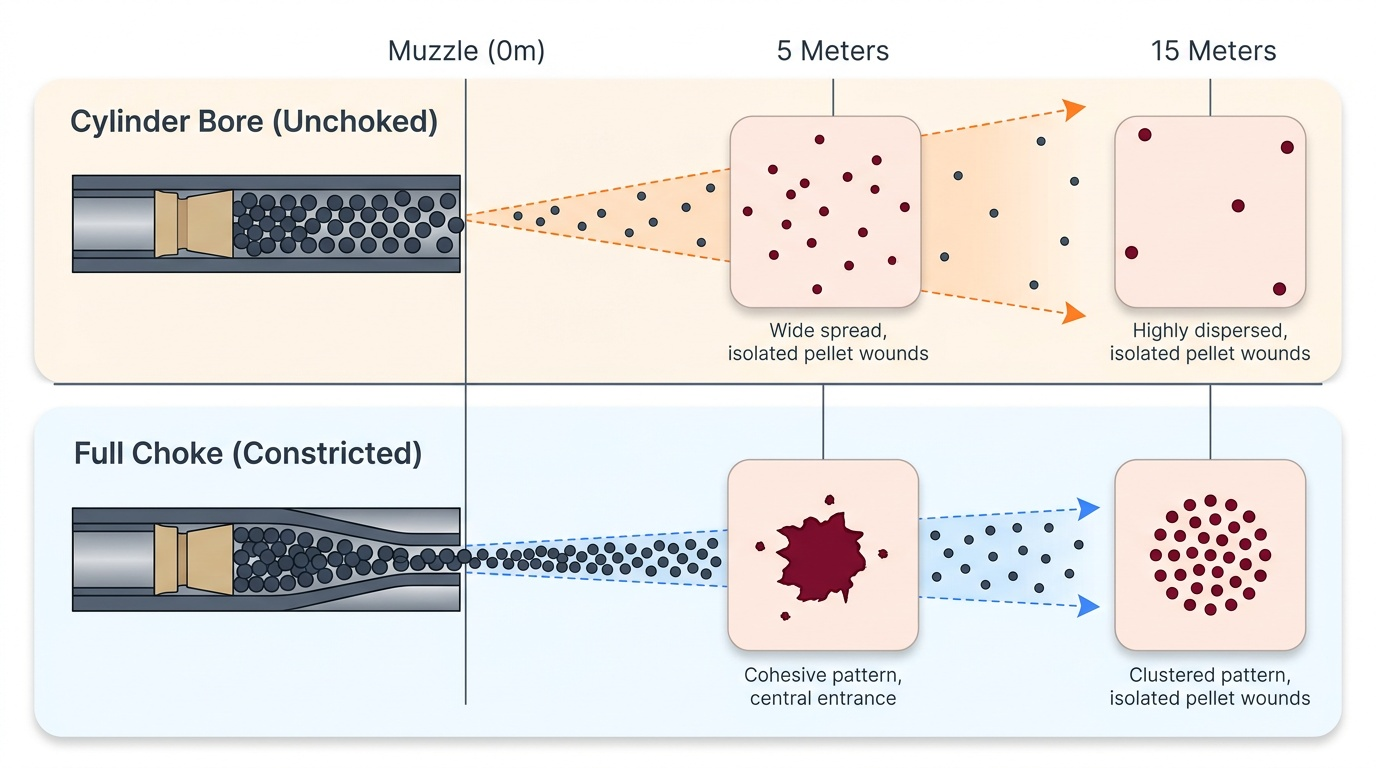
Choke refers to a constriction at or near the muzzle end of a shotgun barrel that controls the spread (divergence) of the pellet charge after leaving the muzzle. Understanding choke is essential for interpreting shotgun wounds because the pellet spread diameter at the target is a function of both range and choke setting — a forensic physician cannot estimate range from pellet spread without knowing the choke.
In an unchoked (cylinder bore) shotgun, the pellets begin to spread immediately on leaving the muzzle. In a choked barrel, the constriction squeezes the pellet charge into a tighter column, delaying their divergence and maintaining a smaller spread pattern over a longer distance. The principal choke designations, from tightest to most open, are: full choke (smallest aperture, tightest pattern), improved modified, modified choke, improved cylinder, and cylinder bore (no choke, widest pattern at any given distance).
Forensically, pellet spread in a shotgun wound is used as follows: at contact and very close range (under 30 cm), all pellets enter through a single wound — the pellets have not yet separated — producing a single, large, circular entrance wound with ragged margins. At intermediate ranges (approximately 1–2 metres), individual satellite pellet holes begin to appear around a central wound. At distant range (beyond approximately 3–5 metres for cylinder bore), the pellets have completely separated and each produces an individual entry wound; the pattern's diameter divided by a spread constant gives an estimate of range. Full choke shifts these distances: what cylinder bore shows at 2 m, full choke may not show until 4–5 m.
Provided image
When conducting a post-mortem on a suspected shotgun death, the forensic physician must record the number of individual pellet holes, the diameter of the total wound pattern, and the distribution of wad (the plastic cup that propels the pellets) — all of which contribute to range estimation and reconstruction of events.
CLINICAL PEARL
Country-made firearms (katta/desi katta) in India present unique forensic challenges. These improvised weapons often use black powder and improvised projectiles (ball bearings, nails, lead slugs cast from melted objects). The wounds they produce may be atypical — irregular entrance wounds, multiple irregular projectile tracks, heavy sooting even at intermediate ranges because of inefficient powder combustion. When you encounter an atypical firearm wound with inconsistent findings, always consider the possibility of a country-made weapon. The medicolegal opinion should state that the wound is 'consistent with a firearm injury, likely from a country-made or improvised weapon' rather than attributing it to a specific factory-loaded firearm. Laboratory analysis of the residue (SEM-EDX) will guide further characterisation. Additionally, country-made guns may lack rifling, making bullet-to-barrel matching impossible — the investigative chain must rely more heavily on GSR and wound morphology.
Medicolegal Documentation and Evidence Preservation
When a firearm is recovered at a scene or submitted as an exhibit, the forensic physician and forensic scientist share responsibility for its proper documentation, handling, and chain-of-custody preservation. Failure at this stage can render ballistic evidence inadmissible in court — the expert witness's opinion is only as strong as the integrity of the exhibit on which it is based.
Documentation of the firearm should include: type of weapon (handgun/rifle/shotgun, revolver/semi-auto), manufacturer and model if legible, serial number (its absence may indicate illicit modification — erasure or obliteration of serial number is itself an offence under the Arms Act 1959), caliber designation stamped on the barrel or frame, and the condition of the weapon (loaded/unloaded, safety on/off, number of rounds in cylinder or magazine). The firearm should never be handled without gloves, and its position relative to the body at the scene must be recorded and photographed before it is moved.
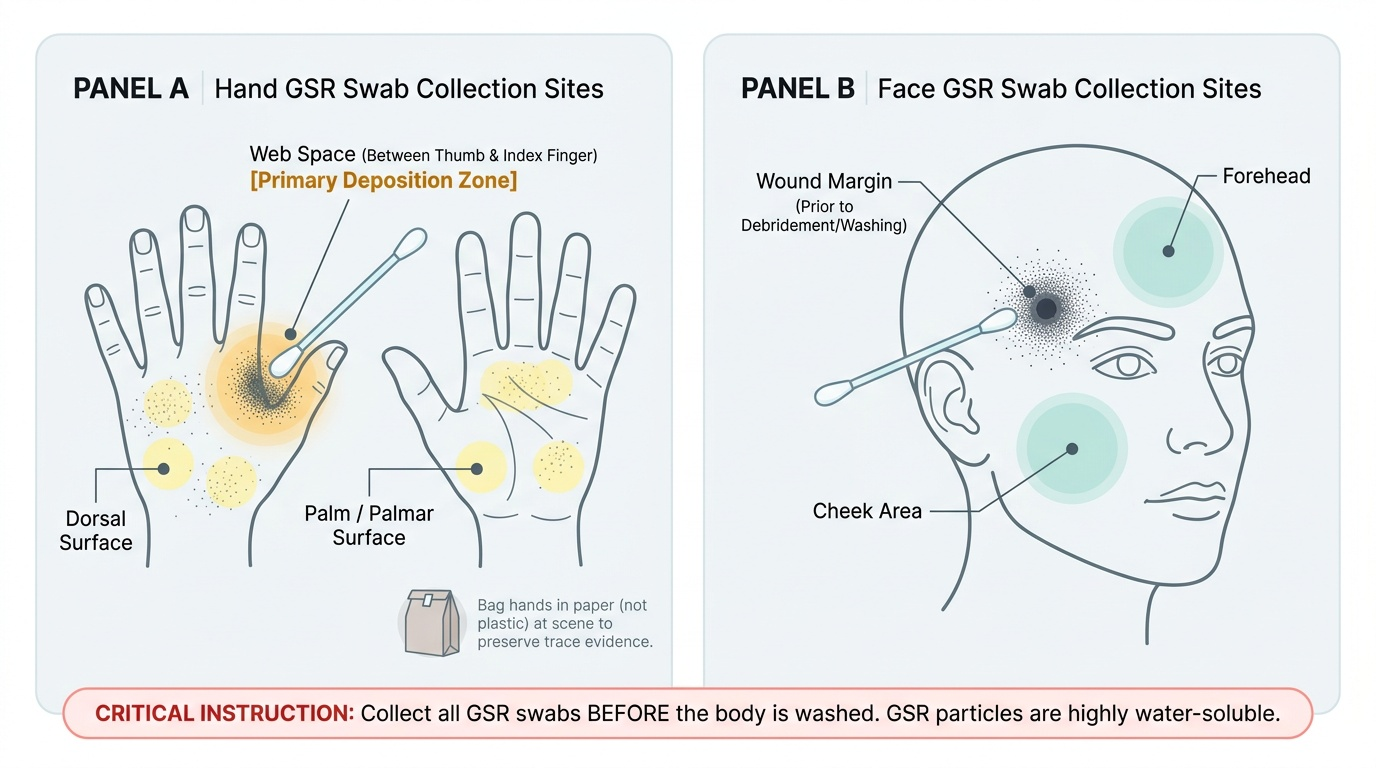
Gunshot residue (GSR) collection from the wound margins, the victim's hands, face, and clothing must occur before the body is washed — GSR particles are water-soluble and will be lost with washing. The hands of the deceased should be bagged in paper (not plastic, which traps moisture) at the scene. Swabs from the wound margins are collected using pre-moistened cotton swabs and placed in sealed, labelled containers. Clothing must be individually bagged, labelled, and submitted to the forensic science laboratory.
Provided image
All exhibits — firearm, ammunition, bullet recovered from body, cartridge cases, swabs — travel in a documented chain of custody from scene to laboratory to court. Every transfer must be recorded with date, time, person receiving, and condition of exhibit. Breaks in chain of custody are a standard line of challenge for defence counsel.