Page 9 of 20
FM7.1 | Regional Injuries: Head, Neck, Trunk, Limbs & Spine — SDL Guide
Learning Objectives
- Classify scalp wounds and describe their forensic significance
- Identify and describe the types of skull fractures and their mechanisms
- Differentiate epidural, subdural, subarachnoid, and intracerebral haemorrhages by source vessel, location, and clinical course
- Explain the mechanism of coup and contre-coup brain injury and its forensic significance for reconstructing the point of impact
- Describe the forensically significant injury patterns of the neck, chest, abdomen, limbs, and genital organs
- Classify spinal cord injuries and describe the forensic significance of railway spine
- Apply IPC sections 319–321 (hurt/grievous hurt) and 299–304 (culpable homicide/murder) to regional injury findings
INSTRUCTIONS
Regional injuries are the daily currency of forensic medical practice in India. Every assault case, every road traffic death, every suspicious fall requires the forensic physician to catalogue injuries by region, describe them precisely, and translate them into medico-legal language that maps onto IPC categories. This module organises that knowledge systematically — from the scalp to the spinal cord — with emphasis on the patterns that most commonly determine criminal charges and civil liability.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old labourer is brought to casualty after being struck on the back of the head with a blunt object during a fight. He was fully conscious at the scene and reportedly 'spoke clearly' to police. By the time the ambulance arrives at hospital, 45 minutes later, he is unconscious and not responding to commands. CT scan shows a lens-shaped hyperdense collection over the right temporal convexity. He dies before surgery. The police charge the attacker with murder (IPC 302). The defence argues the victim had a pre-existing condition and the blow was not lethal. You must provide the court with a medico-legal opinion on the mechanism of death, the type of injury responsible, and whether the blow was 'sufficient in the ordinary course of nature to cause death.' This module teaches you the anatomy of that opinion.
WHY THIS MATTERS
Regional injury analysis is the backbone of most forensic medical opinions in India. The majority of IPC cases involving bodily harm — assault (IPC 319–321), grievous hurt (IPC 320), culpable homicide (IPC 299), and murder (IPC 300) — require a forensic physician to classify the injuries, estimate their severity, and opine on whether they were sufficient to cause death or grievous hurt. Head injuries account for the majority of trauma deaths in India, and the coup/contre-coup mechanism is one of the most frequently misunderstood concepts in both clinical and legal settings. Precise knowledge of intracranial haemorrhage types determines whether a 'lucid interval' followed by deterioration makes neurological sense (epidural haematoma — yes) or not (subdural — usually not classically, though acute subdurals can also produce rapid deterioration). This knowledge directly shapes the medico-legal opinion on survivability and intent.
RECALL
From Year-1 Anatomy and Physiology:
• Meningeal layers: dura mater (outermost, tough, adherent to skull base at sutures), arachnoid (middle, avascular), pia mater (innermost, adherent to brain surface). The subdural space lies between dura and arachnoid; the subarachnoid space between arachnoid and pia.
• Middle meningeal artery: branch of maxillary artery, runs in an extradural groove on the inner surface of the temporal bone — the source vessel for epidural haematoma.
• Bridging veins: drain from brain cortex to dural sinuses, crossing the subdural space — vulnerable to tearing in deceleration injuries.
• Skull base anatomy: cribriform plate, optic canals, petrous temporal bone, foramen magnum — the weak points where basilar fractures occur.
• IPC framework: IPC 319 (simple hurt), IPC 320 (grievous hurt — 8 categories including emasculation, permanent privation of sight/hearing, fracture/dislocation of bone), IPC 299 (culpable homicide), IPC 300 (murder — 4 exceptions define culpable homicide NOT amounting to murder).
Head Injuries: Scalp Wounds and Skull Fractures
The scalp and skull are the first structural targets of cranial trauma, and their injury patterns provide the first forensic clues about the mechanism, force, and direction of impact. Scalp wounds follow the same classification as all mechanical wounds: abrasions (superficial, epidermis only, reveal direction of force if in a linear pattern), contusions (blunt force haemorrhage in soft tissue — the 'black eye' equivalent of the scalp; may extend along fascial planes far from the point of impact), lacerations (blunt force tears — irregular margins, no sharp edge, may contain tissue bridges across the wound, which distinguishes them from incised wounds), and incised wounds (from sharp weapons — clean, straight margins, no tissue bridges). The important medicolegal point is that scalp lacerations and incised wounds can be confused — a short, clean-edged scalp laceration from a blunt object with a sharp edge (e.g., a hammer face or the sharp edge of a stone) may resemble an incised wound. The distinguishing feature is the tissue bridge (thin strands of dermis crossing the wound, visible on cleaning) — present in lacerations, absent in incised wounds.
Skull fractures are classified by morphology and mechanism:
Linear fracture: a single crack in the skull without displacement of the bone; the most common type, caused by relatively low-velocity blunt impact over a broad area. Forensically significant as it marks the site of force application, but brain injury may be minimal unless the fracture crosses a dural venous sinus or meningeal artery groove.
Depressed fracture: a segment of skull bone driven inward below the level of the adjacent outer table. Produced by a high-velocity impact over a small area (a hammer blow, a stone corner, a baseball bat). The depressed fragment may lacerate the dura and brain. The pattern of depression may match the shape of the weapon.
Pond fracture (indented fracture): a smooth, saucer-shaped concave depression without fracture lines radiating from the centre; seen in infants and young children, whose skulls are elastic enough to deform without cracking. In adults, requires significant force.
Contre-coup fracture: fracture on the opposite side of the skull from the impact site — produced by a rapid deceleration (e.g., the head hitting the ground) where the brain continues moving and impacts the far wall of the skull. Distinct from the contre-coup brain injury at the opposite pole.
Hinge fracture (transverse basilar fracture): a fracture running transversely across the base of the skull, creating a 'hinge' effect; produced by side-to-side compression of the head, typically when a vehicle wheel runs over the skull. The fracture line typically passes through the base, separating the skull into an anterior and posterior half. Associated with massive brainstem injury and is usually fatal.
Ring fracture: a circular fracture around the foramen magnum; caused by axial loading — the skull is driven down onto the vertebral column, or the column is driven up into the skull. Seen in falls from height landing on feet and in some diving accidents.
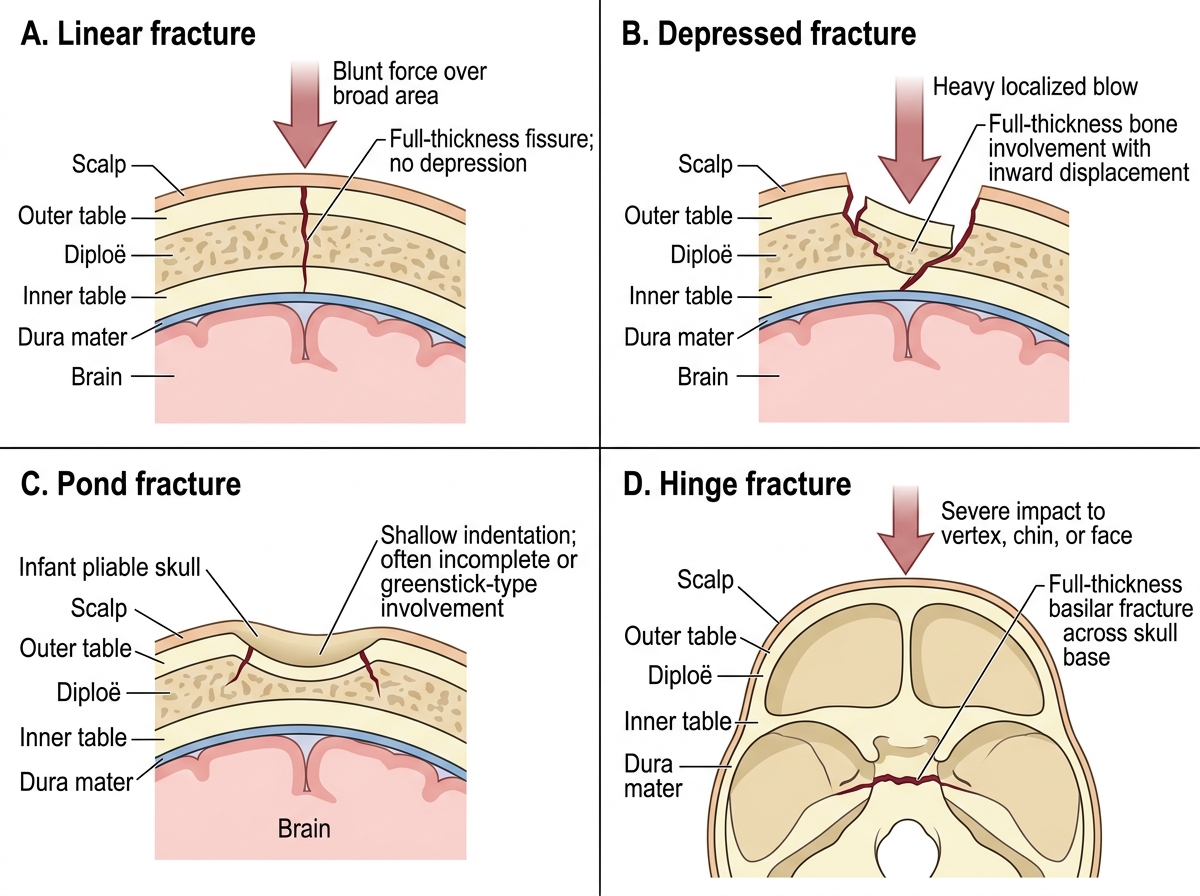
Types of Skull Fractures
Intracranial Haemorrhages: Types, Pathophysiology and Recognition
Intracranial haemorrhages are the principal cause of death and disability from head injuries in forensic cases. Their correct identification is essential for both clinical management (before death) and medico-legal opinion (post-mortem). The four main types differ in their anatomical location, source vessel, CT appearance, and clinical trajectory — and these differences carry direct forensic implications.
Epidural haematoma (EDH) accumulates between the inner surface of the skull and the outer surface of the dura mater. The most common source is the middle meningeal artery, torn at the point of a temporal skull fracture. Because arterial pressure drives rapid accumulation, EDH can expand to 50–100 mL within 30–60 minutes. The classic presentation is a lucid interval — a period of transient consciousness or reduced symptoms after the initial impact, followed by progressive deterioration as haematoma volume increases and transtentorial herniation occurs. The lucid interval is classic but NOT universally present — approximately 30–40% of EDH cases do not show it. On CT, EDH appears as a biconvex (lens-shaped) hyperdense collection adherent to the inner skull table, bounded by cranial sutures (which the dura adheres to, limiting spread across suture lines). EDH is largely a surgical emergency: death is preventable with timely evacuation.
Subdural haematoma (SDH) accumulates between the dura mater and the arachnoid membrane. The source is typically the bridging veins — cortical veins that pass from the brain surface to the dural sinuses, crossing the subdural space. These are ruptured by deceleration forces that cause relative movement between the brain and the overlying dura. SDH is classified by time course: acute (within 72 hours — typically from significant trauma, arterial component possible, high mortality); subacute (3–21 days — from moderate trauma, often in elderly with cerebral atrophy); chronic (>21 days — often in elderly, may follow trivial trauma or even be unrecognised; presents with progressive cognitive decline). On CT, SDH appears as a crescent-shaped collection that follows the brain's contour (crossing suture lines, unlike EDH). The lucid interval is not a feature of SDH in the same classical sense.
Subarachnoid haemorrhage (SAH) occurs between the arachnoid and pia mater — the subarachnoid space, which contains CSF. Traumatic SAH results from tearing of small cortical vessels or extension of parenchymal injury into the subarachnoid space. Spontaneous SAH most commonly results from rupture of a berry (saccular) aneurysm at circle of Willis branch points. The forensic distinction matters: a person with a ruptured berry aneurysm who collapses and sustains a head injury may be misidentified as a trauma victim. SAH classically presents with sudden-onset 'thunderclap' headache; CT shows bright blood in the basal cisterns and sylvian fissures.
Intracerebral haematoma (ICH) is a collection of blood within the brain parenchyma. It results from direct tissue laceration, rupture of penetrating vessels, or haemorrhagic contusion coalescing. Trauma-related ICH is typically in the frontal and temporal lobes (sites of contre-coup injury). On CT, it appears as a hyperdense mass within the white matter.
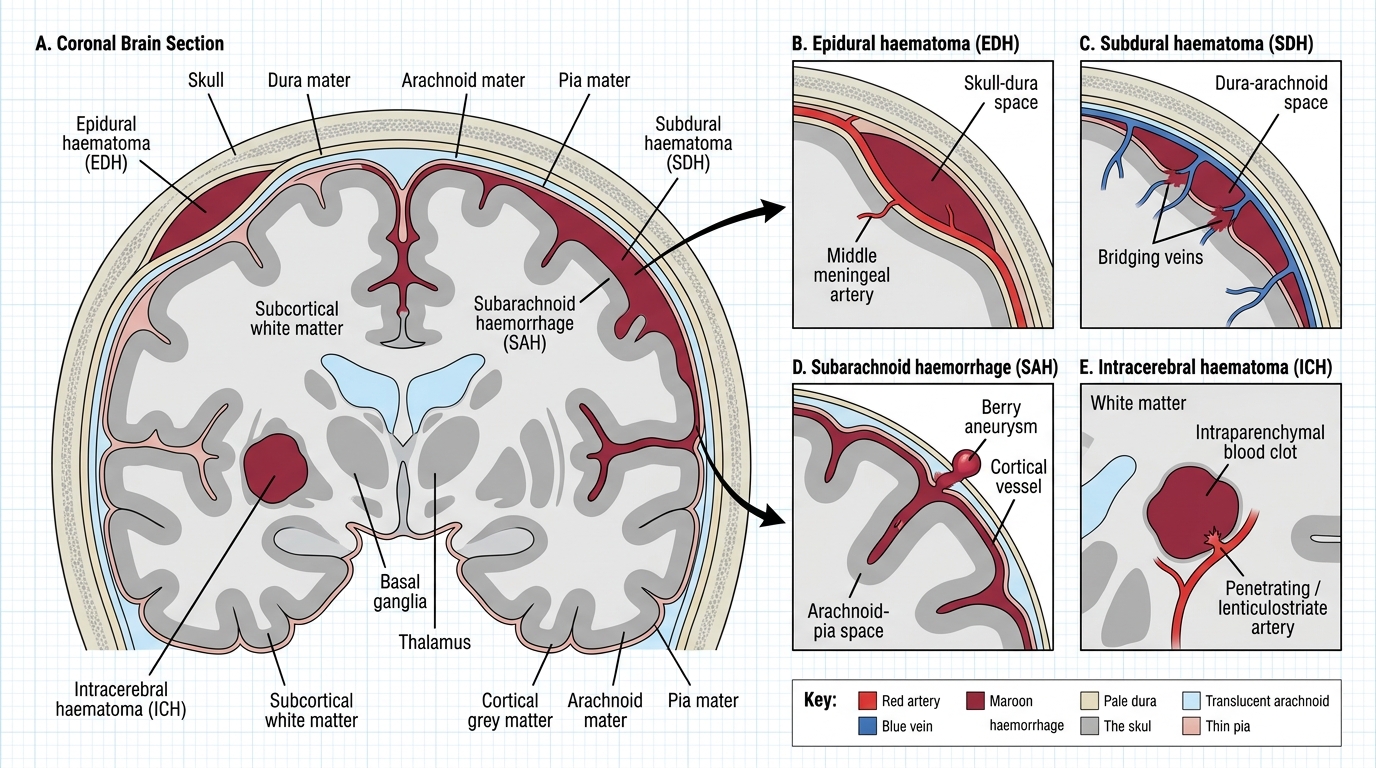
Intracranial Haemorrhage Locations and Source Vessels
| Type | Space | Source vessel | CT appearance | Classic feature | Forensic note |
|---|---|---|---|---|---|
| Epidural (EDH) | Skull-dura | Middle meningeal artery | Biconvex (lens-shaped) | Lucid interval (not invariable) | Preventable death if evacuated early |
| Subdural (SDH) | Dura-arachnoid | Bridging veins | Crescent-shaped | Insidious in chronic form | Deceleration; elderly prone |
| Subarachnoid (SAH) | Arachnoid-pia | Cortical vessels / aneurysm | Blood in basal cisterns | 'Thunderclap' headache | Distinguish traumatic from spontaneous |
| Intracerebral (ICH) | Brain substance | Penetrating vessels | Hyperdense parenchymal mass | Contre-coup sites (frontal/temporal) | Assess contusion coalescence |
SELF-CHECK
A 30-year-old man sustains a head blow in a fight. He walks away from the scene, talks to his wife for 20 minutes, then collapses. He is taken to hospital unconscious. CT shows a biconvex hyperdense collection over the left temporal convexity with a linear skull fracture. Which haematoma type is this, and what is the source vessel?
A. Subdural haematoma; bridging veins ruptured by the blow and accumulated slowly
B. Epidural haematoma; middle meningeal artery torn at the site of the temporal skull fracture
C. Subarachnoid haemorrhage; berry aneurysm at the circle of Willis ruptured after the blow
D. Intracerebral haematoma; contre-coup injury to the right frontal lobe
Reveal Answer
Answer: B. Epidural haematoma; middle meningeal artery torn at the site of the temporal skull fracture
The biconvex (lens-shaped) hyperdense collection over the temporal convexity, associated with a linear skull fracture, is an epidural haematoma (EDH). The source is the middle meningeal artery, which runs in a groove on the inner surface of the temporal bone and is commonly torn when the temporal bone fractures. The lucid interval — the 20 minutes of apparent normality before collapse — is the classic clinical course of expanding arterial EDH and is one of the most important diagnostic clues in both clinical and forensic settings.
Coup and Contre-Coup Brain Injuries
Coup and contre-coup injuries represent one of the most important and most frequently misunderstood concepts in forensic head injury assessment — and one of the most commonly tested. The distinction matters forensically because it allows the physician to reconstruct the site of impact from brain injury findings, even when the external scalp examination is unhelpful or misleading.
Coup injury refers to injury at the site of impact — the point on the brain directly beneath the point where force was applied to the skull. When the head is struck by a moving object (e.g., a hammer blow) while the head is relatively stationary, the local skull deformation and inertial forces cause injury at the impact site. Coup injury typically produces local scalp contusion or laceration, a skull fracture at the impact site, and brain contusion or haemorrhage at the coup pole.
Contre-coup injury refers to injury at the pole opposite to the impact site. It occurs when a moving head decelerates suddenly (hits the ground, hits a wall), because the brain continues moving by inertia and impacts the skull on the far side from the initial contact. The contre-coup mechanism is most severe when the head is moving and the impacting surface is relatively large and flat — the classic scenario being the head hitting the ground in a fall. Contre-coup injury is characteristically seen at the frontal and temporal poles when the occiput (back of the head) hits the ground — the brain's anterior poles slam into the rough floor of the anterior cranial fossa.
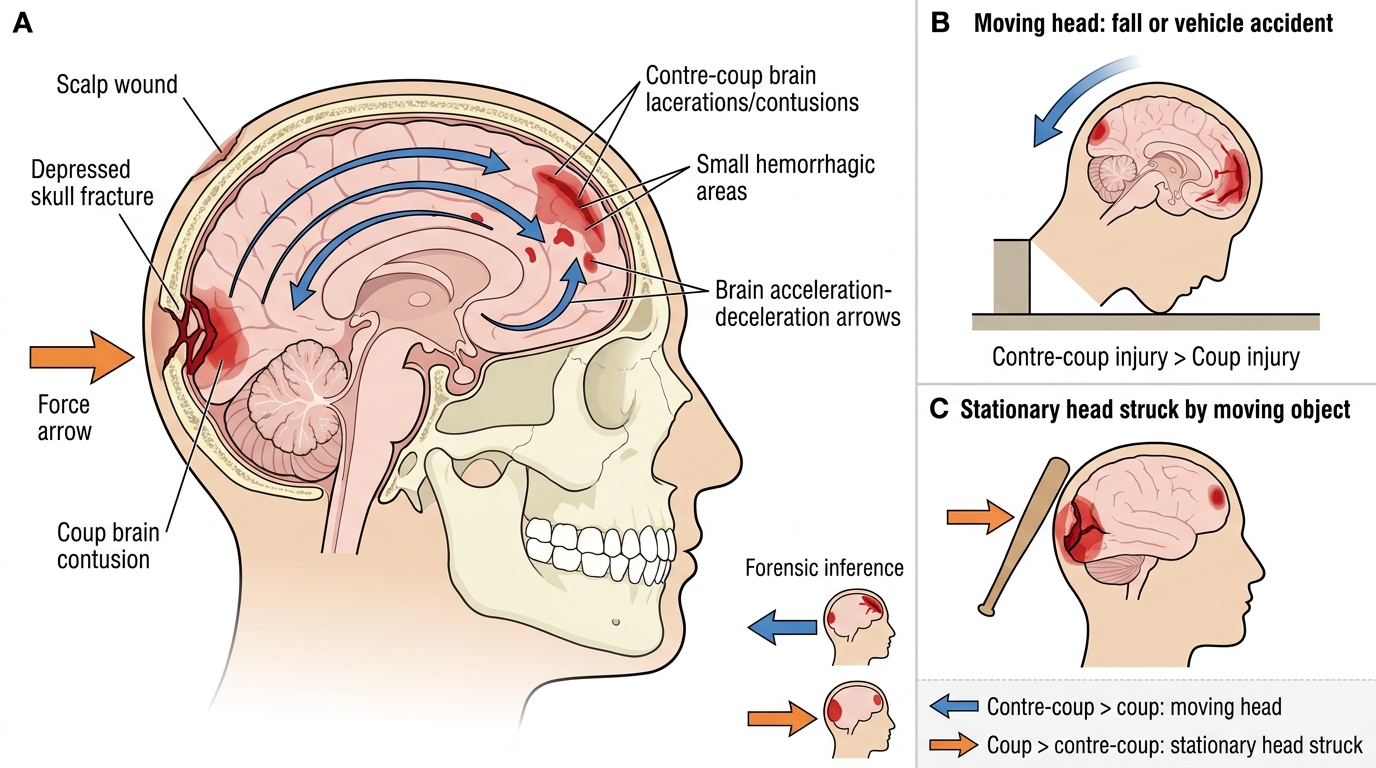
Coup and Contre-Coup Brain Injury Mechanism
The forensic significance is profound: when a fall victim has a scalp injury at the back of the head (occiput) but the brain contusions and haemorrhage are predominantly at the frontal poles, the physician should not conclude that 'the victim was hit in the front of the head' — the contre-coup mechanism explains the mismatch. Conversely, when the brain injury is predominantly under the point of scalp impact, the coup mechanism predominates.
In practice, both coup AND contre-coup injuries may coexist — the brain may show contusions at both poles. The relative severity of coup vs contre-coup injury allows inference about whether the head was moving or relatively stationary at the time of impact: predominantly contre-coup > coup suggests the head was moving (a fall, vehicle accident); predominantly coup > contre-coup suggests the head was stationary and was struck by a moving object (a blow with a weapon). This distinction is forensically critical in differentiating a fall from an assault.
Diffuse Axonal Injury (DAI) occurs when rotational acceleration-deceleration forces stretch and shear axons throughout the white matter, particularly at grey-white matter junctions. It does not produce a focal haematoma; instead, it causes widespread microscopic axonal disruption. DAI is the mechanism behind many severe head injuries with poor outcomes despite normal initial CT scans. Forensically, DAI can cause profound coma and death — the physician should not dismiss a severe head injury case because 'the CT was normal.' MRI and histopathology (beta-APP staining of axons) confirm DAI post-mortem.